
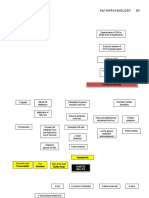
Annotated Group 2 Impetigo Concept Mapping 1
Annotated Group 2 Impetigo Concept Mapping 1
You might also like
- Hinmans Atlas of Pediatric Urology SurgeryDocument950 pagesHinmans Atlas of Pediatric Urology SurgeryDian Auliah Sari HafiedNo ratings yet
- Primary Aldosteronism - A Multidimensional SyndromeDocument18 pagesPrimary Aldosteronism - A Multidimensional SyndromeErwin SiahaanNo ratings yet
- Clinical Reasoning Questions - CollaborationDocument4 pagesClinical Reasoning Questions - CollaborationMohammad OmarNo ratings yet
- 1.MOD On GERON (1) CommunicationDocument19 pages1.MOD On GERON (1) CommunicationPatricia VasquezNo ratings yet
- Concept Mapping: Hodgskin'S Disease ComplicationDocument4 pagesConcept Mapping: Hodgskin'S Disease ComplicationAsterlyn ConiendoNo ratings yet
- BioethicsCasesEEI 316232215 PDFDocument38 pagesBioethicsCasesEEI 316232215 PDFAman UllahNo ratings yet
- Musculoskeletal Physical Therapy AssessmentDocument6 pagesMusculoskeletal Physical Therapy Assessmentlecturio100% (1)
- Anatomy and Physiology DengueDocument5 pagesAnatomy and Physiology Denguenva226No ratings yet
- NVS Written ReportDocument20 pagesNVS Written ReportbabiNo ratings yet
- NCPDocument5 pagesNCPAthea Melosantos100% (1)
- Streptococcus Pneumonae: Pathophysiology of CopdDocument1 pageStreptococcus Pneumonae: Pathophysiology of CopdDimpal ChoudharyNo ratings yet
- Open I Tibia Fibula (R) Lacerated Wounded Leg: Our Lady of Fatima UniversityDocument21 pagesOpen I Tibia Fibula (R) Lacerated Wounded Leg: Our Lady of Fatima UniversityPOTENCIANA MAROMANo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals and Objectives Nursing Interventions and Rationale Evaluation Subjective: NOC: Swallowing Status Goal: NIC: SwallowingDocument10 pagesCues Nursing Diagnosis Background Knowledge Goals and Objectives Nursing Interventions and Rationale Evaluation Subjective: NOC: Swallowing Status Goal: NIC: SwallowingSkyla FiestaNo ratings yet
- Surgical NCP DRUG STUDY PATHOPHYSIOLOGYDocument38 pagesSurgical NCP DRUG STUDY PATHOPHYSIOLOGYBrandy Jaffar100% (1)
- NCP Potts DiseaseDocument2 pagesNCP Potts Diseasearcitap0% (1)
- Potts DiseaseDocument8 pagesPotts Diseaseaimeeros0% (2)
- Pathophysiology of Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar Nonketotic Syndrome EtiologyDocument2 pagesPathophysiology of Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar Nonketotic Syndrome EtiologyJaylord VerazonNo ratings yet
- Pathophysiology Cushing S SyndromeDocument4 pagesPathophysiology Cushing S SyndromeMaria Luisa VillalunaNo ratings yet
- Health Assessment ToolDocument3 pagesHealth Assessment ToolGail GenturalezNo ratings yet
- Kawasaki DiseaseDocument7 pagesKawasaki DiseaseRitamariaNo ratings yet
- Lyceum of The Philippines University - Batangas CollegeDocument120 pagesLyceum of The Philippines University - Batangas CollegeKMNo ratings yet
- Amoebiasis Case StudyDocument13 pagesAmoebiasis Case StudymelvinpasionaNo ratings yet
- Cerebrovascular DiseaseDocument4 pagesCerebrovascular DiseasekathyfacaNo ratings yet
- DOH Approved Medicinal PlantsDocument15 pagesDOH Approved Medicinal PlantsRENSON HERMOGINONo ratings yet
- IV Flow Rate QuizDocument3 pagesIV Flow Rate QuizSheferely BayauaNo ratings yet
- Multiple Physical Injuries Secondary To Vehicular AccidentDocument31 pagesMultiple Physical Injuries Secondary To Vehicular AccidentJane Arian BerzabalNo ratings yet
- Group 5 - Experiment No.10 - Culture and SensitivityDocument11 pagesGroup 5 - Experiment No.10 - Culture and SensitivityPMG BrightNo ratings yet
- 100 Item MEDICAL SURGICAL Nursing Examination Correct Answers andDocument12 pages100 Item MEDICAL SURGICAL Nursing Examination Correct Answers andZyntrx VillasNo ratings yet
- Pott Disease 1223292121651385 8Document54 pagesPott Disease 1223292121651385 8Ismail SalimNo ratings yet
- Vii. Pathophysiology A. AlgorithmDocument2 pagesVii. Pathophysiology A. AlgorithmJonna Mae TurquezaNo ratings yet
- Queenie Rose Domingo - Drug Study (Silver Sulfadiazine)Document1 pageQueenie Rose Domingo - Drug Study (Silver Sulfadiazine)Sheryl Ann Barit PedinesNo ratings yet
- Tetanus PathoDocument3 pagesTetanus PathoElisha Gine AndalesNo ratings yet
- PathophysiologyDocument9 pagesPathophysiologySuzette PipoNo ratings yet
- SLE PathophysiologyDocument3 pagesSLE PathophysiologyyasiraNo ratings yet
- FNCP On Elevated Blood Pressure 2Document4 pagesFNCP On Elevated Blood Pressure 2Aaron EspirituNo ratings yet
- ValeraJMP ACT3Document6 pagesValeraJMP ACT3JMICHELLE VALERANo ratings yet
- Anatomy and Phsyiology of MeningococcemiaDocument2 pagesAnatomy and Phsyiology of MeningococcemiaKevin Comahig100% (1)
- Psych - Chapter 23 Into To Milieu ManagementDocument4 pagesPsych - Chapter 23 Into To Milieu ManagementKaren かれんNo ratings yet
- ScriptDocument2 pagesScriptKeith AquinoNo ratings yet
- Acute Cholecystolithiasis - G4 SB2Document125 pagesAcute Cholecystolithiasis - G4 SB2Jeofy PamaNo ratings yet
- COPAR Tally SheetDocument3 pagesCOPAR Tally SheetAnna SarmientoNo ratings yet
- I. Isbar: I Identity of PatientDocument2 pagesI. Isbar: I Identity of PatientAziil LiizaNo ratings yet
- Case Study On Toxic GoiterDocument5 pagesCase Study On Toxic GoiterRein EstradaNo ratings yet
- Uremic EncephalophatyDocument48 pagesUremic EncephalophatySindi LadayaNo ratings yet
- Splints and Casts Indications and MethodsDocument9 pagesSplints and Casts Indications and MethodsJay GaneshNo ratings yet
- Pneumonia PathoDocument2 pagesPneumonia PathoDerick Nyl PascualNo ratings yet
- What Is Prednisolone?Document12 pagesWhat Is Prednisolone?Chandni SeelochanNo ratings yet
- Pathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsDocument4 pagesPathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsLovely DaroleNo ratings yet
- Resource Unit. AdwcwdDocument6 pagesResource Unit. AdwcwdGreg Martin OrbegosoNo ratings yet
- Nasogastric Tube Feeding ML4763 PDFDocument7 pagesNasogastric Tube Feeding ML4763 PDFStereo PodNo ratings yet
- A Drug Study On FansidarDocument7 pagesA Drug Study On FansidarCasey EmellanoNo ratings yet
- Chronic PyelonephritisDocument5 pagesChronic PyelonephritisIsak ShatikaNo ratings yet
- Ineffective Tissue PerfusionDocument5 pagesIneffective Tissue PerfusionKryza Dale Bunado BaticanNo ratings yet
- Case Presentation OsteomylitisDocument64 pagesCase Presentation OsteomylitisDemi Rose Bolivar100% (1)
- BSN4D-SG2 DM Type2Document201 pagesBSN4D-SG2 DM Type2Charisse CaydanNo ratings yet
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingDocument43 pagesPamantasan NG Cabuyao College of Health Allied Sciences College of NursingSofea MustaffaNo ratings yet
- NCP Impaired Physical MobilityDocument9 pagesNCP Impaired Physical MobilityChristian Apelo SerquillosNo ratings yet
- Case Study 1 (Pneumonia)Document13 pagesCase Study 1 (Pneumonia)Kate EscotonNo ratings yet
- Case Pres A1-RhdDocument11 pagesCase Pres A1-RhdCharm TanyaNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Indri Drug EruptionDocument45 pagesIndri Drug EruptionIndrii GraciaNo ratings yet
- Acrodermatitis EnteropathicaDocument4 pagesAcrodermatitis EnteropathicaIntan FajrinNo ratings yet
- 40 Normal Labor and DystociaDocument47 pages40 Normal Labor and DystociaCitra Wulandari SofyanNo ratings yet
- GAG ReflexDocument4 pagesGAG Reflexdrgayen6042No ratings yet
- Body Types Module 5Document3 pagesBody Types Module 5a2a4alensunnyNo ratings yet
- Premature Atrial Contractions: A Wolf in Sheep's Clothing?Document3 pagesPremature Atrial Contractions: A Wolf in Sheep's Clothing?daindesNo ratings yet
- ChecklistDocument3 pagesChecklistRodel Aguila SañoNo ratings yet
- Rekambys Epar Product Information - en PDFDocument74 pagesRekambys Epar Product Information - en PDFCamelia AirineiNo ratings yet
- Paraneoplastic Syndromes in Lung CancerDocument35 pagesParaneoplastic Syndromes in Lung CancerEl FaroukNo ratings yet
- 6th Course For Somatosensory Rehabilitation of PainDocument10 pages6th Course For Somatosensory Rehabilitation of PainGerry OconnorNo ratings yet
- Global Health Priorities and ProgramsDocument22 pagesGlobal Health Priorities and ProgramsNalu ChangNo ratings yet
- DUMMYZ005 : LPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Document2 pagesDUMMYZ005 : LPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Yatin VermaNo ratings yet
- Klinefelter SyndromeDocument28 pagesKlinefelter SyndromeKimberly Anne Marica0% (1)
- Comorbidity Guideline PDFDocument446 pagesComorbidity Guideline PDFglenNo ratings yet
- Burns SeminarDocument66 pagesBurns SeminarPratibha Thakur100% (1)
- Wad GuidelinesDocument23 pagesWad GuidelinesDharam PandeyNo ratings yet
- Hospital Preparedness For Pandemic Outbreaks A Comparative Perspective of National and Global GuidelinesDocument7 pagesHospital Preparedness For Pandemic Outbreaks A Comparative Perspective of National and Global GuidelinesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unit 4 Capstone PowerpointDocument8 pagesUnit 4 Capstone Powerpointapi-269707483No ratings yet
- NCP CellulitisDocument2 pagesNCP CellulitisAira AlaroNo ratings yet
- SulpirideDocument4 pagesSulpirideIsmail Ali SyahbanaNo ratings yet
- LidocaineDocument27 pagesLidocaineNadya PrafitaNo ratings yet
- Dermatology Slides - Introduction To Clinical DermatologyDocument34 pagesDermatology Slides - Introduction To Clinical DermatologyAzry Mustapa100% (1)
- J Annemergmed 2017 01 018Document14 pagesJ Annemergmed 2017 01 018Jorge BarriosNo ratings yet
- Mood Disorders-Causes and TreatmentsDocument9 pagesMood Disorders-Causes and TreatmentsMica MoradaNo ratings yet
- DSMES Intervention Tracking Form (Chart 7)Document1 pageDSMES Intervention Tracking Form (Chart 7)Bryan MorteraNo ratings yet
- Scientific American HM PDFDocument37 pagesScientific American HM PDFGina VarlanNo ratings yet
- LOGIQ Book XP EnhancedDocument30 pagesLOGIQ Book XP EnhancedartiboNo ratings yet
- The Placebo EffectDocument14 pagesThe Placebo EffectMichelle WenasNo ratings yet
- Nurs 233 Summative Clinical Evaluation-AfDocument3 pagesNurs 233 Summative Clinical Evaluation-Afapi-596284176No ratings yet
























































































Download as pdf or txt
You might also like
- Hinmans Atlas of Pediatric Urology SurgeryDocument950 pagesHinmans Atlas of Pediatric Urology SurgeryDian Auliah Sari HafiedNo ratings yet
- Primary Aldosteronism - A Multidimensional SyndromeDocument18 pagesPrimary Aldosteronism - A Multidimensional SyndromeErwin SiahaanNo ratings yet
- Clinical Reasoning Questions - CollaborationDocument4 pagesClinical Reasoning Questions - CollaborationMohammad OmarNo ratings yet
- 1.MOD On GERON (1) CommunicationDocument19 pages1.MOD On GERON (1) CommunicationPatricia VasquezNo ratings yet
- Concept Mapping: Hodgskin'S Disease ComplicationDocument4 pagesConcept Mapping: Hodgskin'S Disease ComplicationAsterlyn ConiendoNo ratings yet
- BioethicsCasesEEI 316232215 PDFDocument38 pagesBioethicsCasesEEI 316232215 PDFAman UllahNo ratings yet
- Musculoskeletal Physical Therapy AssessmentDocument6 pagesMusculoskeletal Physical Therapy Assessmentlecturio100% (1)
- Anatomy and Physiology DengueDocument5 pagesAnatomy and Physiology Denguenva226No ratings yet
- NVS Written ReportDocument20 pagesNVS Written ReportbabiNo ratings yet
- NCPDocument5 pagesNCPAthea Melosantos100% (1)
- Streptococcus Pneumonae: Pathophysiology of CopdDocument1 pageStreptococcus Pneumonae: Pathophysiology of CopdDimpal ChoudharyNo ratings yet
- Open I Tibia Fibula (R) Lacerated Wounded Leg: Our Lady of Fatima UniversityDocument21 pagesOpen I Tibia Fibula (R) Lacerated Wounded Leg: Our Lady of Fatima UniversityPOTENCIANA MAROMANo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals and Objectives Nursing Interventions and Rationale Evaluation Subjective: NOC: Swallowing Status Goal: NIC: SwallowingDocument10 pagesCues Nursing Diagnosis Background Knowledge Goals and Objectives Nursing Interventions and Rationale Evaluation Subjective: NOC: Swallowing Status Goal: NIC: SwallowingSkyla FiestaNo ratings yet
- Surgical NCP DRUG STUDY PATHOPHYSIOLOGYDocument38 pagesSurgical NCP DRUG STUDY PATHOPHYSIOLOGYBrandy Jaffar100% (1)
- NCP Potts DiseaseDocument2 pagesNCP Potts Diseasearcitap0% (1)
- Potts DiseaseDocument8 pagesPotts Diseaseaimeeros0% (2)
- Pathophysiology of Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar Nonketotic Syndrome EtiologyDocument2 pagesPathophysiology of Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar Nonketotic Syndrome EtiologyJaylord VerazonNo ratings yet
- Pathophysiology Cushing S SyndromeDocument4 pagesPathophysiology Cushing S SyndromeMaria Luisa VillalunaNo ratings yet
- Health Assessment ToolDocument3 pagesHealth Assessment ToolGail GenturalezNo ratings yet
- Kawasaki DiseaseDocument7 pagesKawasaki DiseaseRitamariaNo ratings yet
- Lyceum of The Philippines University - Batangas CollegeDocument120 pagesLyceum of The Philippines University - Batangas CollegeKMNo ratings yet
- Amoebiasis Case StudyDocument13 pagesAmoebiasis Case StudymelvinpasionaNo ratings yet
- Cerebrovascular DiseaseDocument4 pagesCerebrovascular DiseasekathyfacaNo ratings yet
- DOH Approved Medicinal PlantsDocument15 pagesDOH Approved Medicinal PlantsRENSON HERMOGINONo ratings yet
- IV Flow Rate QuizDocument3 pagesIV Flow Rate QuizSheferely BayauaNo ratings yet
- Multiple Physical Injuries Secondary To Vehicular AccidentDocument31 pagesMultiple Physical Injuries Secondary To Vehicular AccidentJane Arian BerzabalNo ratings yet
- Group 5 - Experiment No.10 - Culture and SensitivityDocument11 pagesGroup 5 - Experiment No.10 - Culture and SensitivityPMG BrightNo ratings yet
- 100 Item MEDICAL SURGICAL Nursing Examination Correct Answers andDocument12 pages100 Item MEDICAL SURGICAL Nursing Examination Correct Answers andZyntrx VillasNo ratings yet
- Pott Disease 1223292121651385 8Document54 pagesPott Disease 1223292121651385 8Ismail SalimNo ratings yet
- Vii. Pathophysiology A. AlgorithmDocument2 pagesVii. Pathophysiology A. AlgorithmJonna Mae TurquezaNo ratings yet
- Queenie Rose Domingo - Drug Study (Silver Sulfadiazine)Document1 pageQueenie Rose Domingo - Drug Study (Silver Sulfadiazine)Sheryl Ann Barit PedinesNo ratings yet
- Tetanus PathoDocument3 pagesTetanus PathoElisha Gine AndalesNo ratings yet
- PathophysiologyDocument9 pagesPathophysiologySuzette PipoNo ratings yet
- SLE PathophysiologyDocument3 pagesSLE PathophysiologyyasiraNo ratings yet
- FNCP On Elevated Blood Pressure 2Document4 pagesFNCP On Elevated Blood Pressure 2Aaron EspirituNo ratings yet
- ValeraJMP ACT3Document6 pagesValeraJMP ACT3JMICHELLE VALERANo ratings yet
- Anatomy and Phsyiology of MeningococcemiaDocument2 pagesAnatomy and Phsyiology of MeningococcemiaKevin Comahig100% (1)
- Psych - Chapter 23 Into To Milieu ManagementDocument4 pagesPsych - Chapter 23 Into To Milieu ManagementKaren かれんNo ratings yet
- ScriptDocument2 pagesScriptKeith AquinoNo ratings yet
- Acute Cholecystolithiasis - G4 SB2Document125 pagesAcute Cholecystolithiasis - G4 SB2Jeofy PamaNo ratings yet
- COPAR Tally SheetDocument3 pagesCOPAR Tally SheetAnna SarmientoNo ratings yet
- I. Isbar: I Identity of PatientDocument2 pagesI. Isbar: I Identity of PatientAziil LiizaNo ratings yet
- Case Study On Toxic GoiterDocument5 pagesCase Study On Toxic GoiterRein EstradaNo ratings yet
- Uremic EncephalophatyDocument48 pagesUremic EncephalophatySindi LadayaNo ratings yet
- Splints and Casts Indications and MethodsDocument9 pagesSplints and Casts Indications and MethodsJay GaneshNo ratings yet
- Pneumonia PathoDocument2 pagesPneumonia PathoDerick Nyl PascualNo ratings yet
- What Is Prednisolone?Document12 pagesWhat Is Prednisolone?Chandni SeelochanNo ratings yet
- Pathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsDocument4 pagesPathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsLovely DaroleNo ratings yet
- Resource Unit. AdwcwdDocument6 pagesResource Unit. AdwcwdGreg Martin OrbegosoNo ratings yet
- Nasogastric Tube Feeding ML4763 PDFDocument7 pagesNasogastric Tube Feeding ML4763 PDFStereo PodNo ratings yet
- A Drug Study On FansidarDocument7 pagesA Drug Study On FansidarCasey EmellanoNo ratings yet
- Chronic PyelonephritisDocument5 pagesChronic PyelonephritisIsak ShatikaNo ratings yet
- Ineffective Tissue PerfusionDocument5 pagesIneffective Tissue PerfusionKryza Dale Bunado BaticanNo ratings yet
- Case Presentation OsteomylitisDocument64 pagesCase Presentation OsteomylitisDemi Rose Bolivar100% (1)
- BSN4D-SG2 DM Type2Document201 pagesBSN4D-SG2 DM Type2Charisse CaydanNo ratings yet
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingDocument43 pagesPamantasan NG Cabuyao College of Health Allied Sciences College of NursingSofea MustaffaNo ratings yet
- NCP Impaired Physical MobilityDocument9 pagesNCP Impaired Physical MobilityChristian Apelo SerquillosNo ratings yet
- Case Study 1 (Pneumonia)Document13 pagesCase Study 1 (Pneumonia)Kate EscotonNo ratings yet
- Case Pres A1-RhdDocument11 pagesCase Pres A1-RhdCharm TanyaNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Indri Drug EruptionDocument45 pagesIndri Drug EruptionIndrii GraciaNo ratings yet
- Acrodermatitis EnteropathicaDocument4 pagesAcrodermatitis EnteropathicaIntan FajrinNo ratings yet
- 40 Normal Labor and DystociaDocument47 pages40 Normal Labor and DystociaCitra Wulandari SofyanNo ratings yet
- GAG ReflexDocument4 pagesGAG Reflexdrgayen6042No ratings yet
- Body Types Module 5Document3 pagesBody Types Module 5a2a4alensunnyNo ratings yet
- Premature Atrial Contractions: A Wolf in Sheep's Clothing?Document3 pagesPremature Atrial Contractions: A Wolf in Sheep's Clothing?daindesNo ratings yet
- ChecklistDocument3 pagesChecklistRodel Aguila SañoNo ratings yet
- Rekambys Epar Product Information - en PDFDocument74 pagesRekambys Epar Product Information - en PDFCamelia AirineiNo ratings yet
- Paraneoplastic Syndromes in Lung CancerDocument35 pagesParaneoplastic Syndromes in Lung CancerEl FaroukNo ratings yet
- 6th Course For Somatosensory Rehabilitation of PainDocument10 pages6th Course For Somatosensory Rehabilitation of PainGerry OconnorNo ratings yet
- Global Health Priorities and ProgramsDocument22 pagesGlobal Health Priorities and ProgramsNalu ChangNo ratings yet
- DUMMYZ005 : LPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Document2 pagesDUMMYZ005 : LPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Yatin VermaNo ratings yet
- Klinefelter SyndromeDocument28 pagesKlinefelter SyndromeKimberly Anne Marica0% (1)
- Comorbidity Guideline PDFDocument446 pagesComorbidity Guideline PDFglenNo ratings yet
- Burns SeminarDocument66 pagesBurns SeminarPratibha Thakur100% (1)
- Wad GuidelinesDocument23 pagesWad GuidelinesDharam PandeyNo ratings yet
- Hospital Preparedness For Pandemic Outbreaks A Comparative Perspective of National and Global GuidelinesDocument7 pagesHospital Preparedness For Pandemic Outbreaks A Comparative Perspective of National and Global GuidelinesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unit 4 Capstone PowerpointDocument8 pagesUnit 4 Capstone Powerpointapi-269707483No ratings yet
- NCP CellulitisDocument2 pagesNCP CellulitisAira AlaroNo ratings yet
- SulpirideDocument4 pagesSulpirideIsmail Ali SyahbanaNo ratings yet
- LidocaineDocument27 pagesLidocaineNadya PrafitaNo ratings yet
- Dermatology Slides - Introduction To Clinical DermatologyDocument34 pagesDermatology Slides - Introduction To Clinical DermatologyAzry Mustapa100% (1)
- J Annemergmed 2017 01 018Document14 pagesJ Annemergmed 2017 01 018Jorge BarriosNo ratings yet
- Mood Disorders-Causes and TreatmentsDocument9 pagesMood Disorders-Causes and TreatmentsMica MoradaNo ratings yet
- DSMES Intervention Tracking Form (Chart 7)Document1 pageDSMES Intervention Tracking Form (Chart 7)Bryan MorteraNo ratings yet
- Scientific American HM PDFDocument37 pagesScientific American HM PDFGina VarlanNo ratings yet
- LOGIQ Book XP EnhancedDocument30 pagesLOGIQ Book XP EnhancedartiboNo ratings yet
- The Placebo EffectDocument14 pagesThe Placebo EffectMichelle WenasNo ratings yet
- Nurs 233 Summative Clinical Evaluation-AfDocument3 pagesNurs 233 Summative Clinical Evaluation-Afapi-596284176No ratings yet