Download as pdf or txt
You might also like
- Visual Mnemonics Pharmacology 3rd Edition 0wv DR NotesDocument335 pagesVisual Mnemonics Pharmacology 3rd Edition 0wv DR NotesJulia Rae Delos Santos100% (2)
- EUOGS OSCE Booklet 2020Document26 pagesEUOGS OSCE Booklet 2020Amanda Leow100% (1)
- KKH Baby Bear Book 2010 2nd EditionDocument305 pagesKKH Baby Bear Book 2010 2nd EditionErnest Ho100% (4)
- Cardio InternetDocument46 pagesCardio InternetnaimNo ratings yet
- Bojar PediatricDocument123 pagesBojar PediatricLuqman AlwiNo ratings yet
- Coarctation of The AortaDocument2 pagesCoarctation of The AortaDavid Cheng0% (1)
- Acyanotic Congenital Heart DiseaseDocument48 pagesAcyanotic Congenital Heart DiseasenabillagusrinaNo ratings yet
- Cardiovascular Dysfunction: (Patent Ductus Arteriosus)Document6 pagesCardiovascular Dysfunction: (Patent Ductus Arteriosus)Jc MacujaNo ratings yet
- Congenital Heart DefectsDocument45 pagesCongenital Heart Defectskathylaine100% (1)
- Tetralogy of Fallot: Arianna Jasminemabunga Bsn-2BDocument30 pagesTetralogy of Fallot: Arianna Jasminemabunga Bsn-2BArianna Jasmine MabungaNo ratings yet
- Pediatric History Taking Chart PDFDocument2 pagesPediatric History Taking Chart PDFHerlene Lyneth ZalamedaNo ratings yet
- Cardiovascular DiseasesDocument8 pagesCardiovascular DiseasesRebecca MarshallNo ratings yet
- Idiopathic Thrombocytopenic PurpuraDocument10 pagesIdiopathic Thrombocytopenic Purpuramariakolanda100% (1)
- Tetralogy of FallotDocument38 pagesTetralogy of FallotJohn Paul MedalloNo ratings yet
- NCLEX SampleDocument12 pagesNCLEX SampleYasser AhmedNo ratings yet
- Cardiovascular Disease PDFDocument6 pagesCardiovascular Disease PDFPerry SinNo ratings yet
- Cyanosis in The NewbornDocument32 pagesCyanosis in The Newbornimma_2014No ratings yet
- Acyanotic Congenital Heart DiseaseDocument10 pagesAcyanotic Congenital Heart DiseaseSuraj SolankiNo ratings yet
- Congenital Heart DiseaseDocument106 pagesCongenital Heart DiseaseHarold DiasanaNo ratings yet
- Oral Revalida Im Cases Dec. 12 and 13 2020Document16 pagesOral Revalida Im Cases Dec. 12 and 13 2020Bea Y. Bas-ongNo ratings yet
- 25 Cardiovascular DiseaseDocument35 pages25 Cardiovascular DiseaseBramantyo NugrosNo ratings yet
- 4 PEDIA 8 - Bleeding DisordersDocument5 pages4 PEDIA 8 - Bleeding DisordersRainy Liony DuhNo ratings yet
- Cardio Vascular DisordersDocument62 pagesCardio Vascular DisordersUday Kumar100% (1)
- Atrial Septal DefectDocument12 pagesAtrial Septal DefectNurruhaizi Aizi100% (1)
- Patent Ductus Arteriosus 6. Aortic Stenosis: Signs and Symptoms: Signs and SymptomsDocument3 pagesPatent Ductus Arteriosus 6. Aortic Stenosis: Signs and Symptoms: Signs and SymptomsKIANA LOUISE ROMANONo ratings yet
- ASD Atrial Septal Defect PDFDocument9 pagesASD Atrial Septal Defect PDFAco AjjahNo ratings yet
- Valvular Heart DiseaseDocument43 pagesValvular Heart Diseaseurmila prajapatiNo ratings yet
- Idiopathic Thrombocytopenic Purpura (ITP)Document7 pagesIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiNo ratings yet
- Hirschsprung's Disease - AthigamanDocument128 pagesHirschsprung's Disease - Athigamanprived100% (4)
- Pyloric StenosisDocument11 pagesPyloric StenosisJustin CharlesNo ratings yet
- Approach To Cyanotic Heart Disease Christopher Cheung Santokh Dhillon PDFDocument13 pagesApproach To Cyanotic Heart Disease Christopher Cheung Santokh Dhillon PDFsuckeydluffyNo ratings yet
- Congenital Heart Disease Made EasyDocument30 pagesCongenital Heart Disease Made EasyChristian HarnatNo ratings yet
- Cardiomyopathy and MyocarditisDocument8 pagesCardiomyopathy and Myocarditisoddone_out100% (1)
- 1.basic Final McqsDocument78 pages1.basic Final McqsPrabhat KcNo ratings yet
- Atrial Septal DefectDocument3 pagesAtrial Septal Defectsyahid_unsriNo ratings yet
- Lecture Hemophilia and Thrombocytopenic PurpuraDocument55 pagesLecture Hemophilia and Thrombocytopenic PurpuraaymenNo ratings yet
- Final Exam NotesDocument24 pagesFinal Exam NotesNicholeGarcesCisnerosNo ratings yet
- History and Physical Exam Skills List: Opening VisitDocument7 pagesHistory and Physical Exam Skills List: Opening VisitAnonymous Sfcml4GvZNo ratings yet
- Rheumatic Heart Disease AustrliaDocument63 pagesRheumatic Heart Disease AustrliaMuhammad Reza100% (2)
- How To Read A CTG - Geeky MedicsDocument10 pagesHow To Read A CTG - Geeky MedicsDivyesh DholariyaNo ratings yet
- BT CT PT PTTDocument31 pagesBT CT PT PTTCristineVillablancaNo ratings yet
- Med Surg MidtermDocument17 pagesMed Surg Midtermjhan grabierNo ratings yet
- Nephroblastoma FinalDocument24 pagesNephroblastoma FinalKrissy_Singh_211No ratings yet
- Gynecology and Obstretics Assignment (MCQS)Document9 pagesGynecology and Obstretics Assignment (MCQS)Jehanzeb AkramNo ratings yet
- Rheumatic Heart Disease and Infective EndocarditisDocument10 pagesRheumatic Heart Disease and Infective Endocarditisapi-19840404No ratings yet
- Congenital Development of Urinary SystemDocument31 pagesCongenital Development of Urinary SystemRinxas VerinxtNo ratings yet
- Signs of Respiratory Distress in Your Child: Signs To Look ForDocument2 pagesSigns of Respiratory Distress in Your Child: Signs To Look ForMa GynNo ratings yet
- Newborn Physical AssessmentDocument2 pagesNewborn Physical AssessmentEunice May Saban AldaNo ratings yet
- Mal Presentations Mal PositionsDocument4 pagesMal Presentations Mal PositionsMelissa Aina Mohd YusofNo ratings yet
- Ventricular Septal DefectDocument8 pagesVentricular Septal DefectMarina RotaruNo ratings yet
- Sudden Cardiac Death: Ischaemic Heart DiseaseDocument4 pagesSudden Cardiac Death: Ischaemic Heart Diseasenmyza89No ratings yet
- Thalassemia (Revised)Document5 pagesThalassemia (Revised)AradhanaRamchandaniNo ratings yet
- O and G Notes Notebank NumberedDocument173 pagesO and G Notes Notebank NumberedPerscitus Ali القحطانيNo ratings yet
- Approach To Short Stature (Autosaved)Document34 pagesApproach To Short Stature (Autosaved)Sahil Dhamija100% (1)
- Newborn Respiratory Distress 11.28.2011Document41 pagesNewborn Respiratory Distress 11.28.2011Emily EresumaNo ratings yet
- Developmental Milestone of Preschool AgeDocument3 pagesDevelopmental Milestone of Preschool AgeJessa Mae BacuganNo ratings yet
- Fetal CirculationDocument19 pagesFetal Circulation3sshhhNo ratings yet
- Kawasaki Disease LectureDocument25 pagesKawasaki Disease LectureAlif ZainalNo ratings yet
- Endocarditis: (Post Strep Infection)Document8 pagesEndocarditis: (Post Strep Infection)Eben Ezar Dela CruzNo ratings yet
- Gyne Case COCDocument37 pagesGyne Case COCLian BaylosisNo ratings yet
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Neuro Anatomy Neuro AssessmentDocument96 pagesNeuro Anatomy Neuro AssessmentJulia Rae Delos SantosNo ratings yet
- Neuro Anatomy Neuro AssessmentDocument96 pagesNeuro Anatomy Neuro AssessmentJulia Rae Delos SantosNo ratings yet
- Session 2 GiDocument12 pagesSession 2 GiJulia Rae Delos SantosNo ratings yet
- IICP TransesDocument3 pagesIICP TransesJulia Rae Delos SantosNo ratings yet
- Increased Intracranial PressureDocument48 pagesIncreased Intracranial PressureJulia Rae Delos SantosNo ratings yet
- Thyroid CancerDocument5 pagesThyroid CancerJulia Rae Delos SantosNo ratings yet
- MS Lec Gi P1Document6 pagesMS Lec Gi P1Julia Rae Delos SantosNo ratings yet
- The Digestive System Powerpoint 1227698045024899 8Document44 pagesThe Digestive System Powerpoint 1227698045024899 8Julia Rae Delos Santos100% (1)
- Cancer Ms LecDocument16 pagesCancer Ms LecJulia Rae Delos Santos100% (1)
- Surgical InstrumentsDocument78 pagesSurgical InstrumentsJulia Rae Delos SantosNo ratings yet
- DRUG STUDY - Delos SantosDocument1 pageDRUG STUDY - Delos SantosJulia Rae Delos SantosNo ratings yet
- Trans Notes TemplateDocument1 pageTrans Notes TemplateJulia Rae Delos SantosNo ratings yet
- NURSING CARE PLAN Urinary IncontinenceDocument5 pagesNURSING CARE PLAN Urinary IncontinenceJulia Rae Delos SantosNo ratings yet
- ValvularDocument2 pagesValvularJulia Rae Delos SantosNo ratings yet
- Disturbed Thoughts NCPDocument1 pageDisturbed Thoughts NCPJulia Rae Delos SantosNo ratings yet
- NSG Journal - Delos SantosDocument2 pagesNSG Journal - Delos SantosJulia Rae Delos SantosNo ratings yet
- NursingJournal Delos SantosDocument2 pagesNursingJournal Delos SantosJulia Rae Delos SantosNo ratings yet
- Infectious Diseases of The HeartDocument2 pagesInfectious Diseases of The HeartJulia Rae Delos SantosNo ratings yet
- Sickle Cell & ThalassemiaDocument3 pagesSickle Cell & ThalassemiaJulia Rae Delos SantosNo ratings yet
- LeukemiaDocument3 pagesLeukemiaJulia Rae Delos SantosNo ratings yet
- Hypertension: 1. Systolic and Diastolic HypertensionDocument3 pagesHypertension: 1. Systolic and Diastolic HypertensionJulia Rae Delos SantosNo ratings yet
- Buerger'S Disease Raynaud'S Disease Buerger'S Disease Raynaud'S DiseaseDocument4 pagesBuerger'S Disease Raynaud'S Disease Buerger'S Disease Raynaud'S DiseaseJulia Rae Delos SantosNo ratings yet
- Electrocardiogram Interpretation and Nursing InterDocument4 pagesElectrocardiogram Interpretation and Nursing InterJulia Rae Delos SantosNo ratings yet
- Book Cardio ConceptDocument29 pagesBook Cardio ConceptJulia Rae Delos SantosNo ratings yet
- Coronary Artery DiseaseDocument2 pagesCoronary Artery DiseaseJulia Rae Delos SantosNo ratings yet
- G6PD, Polycythemia Vera, ITP, Hemophilia, DICDocument6 pagesG6PD, Polycythemia Vera, ITP, Hemophilia, DICJulia Rae Delos SantosNo ratings yet
- Inflammation & Wound Healing Part 1Document2 pagesInflammation & Wound Healing Part 1Julia Rae Delos SantosNo ratings yet
- Book Onco ConceptDocument42 pagesBook Onco ConceptJulia Rae Delos SantosNo ratings yet
- Hema ConceptsDocument12 pagesHema ConceptsJulia Rae Delos SantosNo ratings yet
- NitroglycerinDocument1 pageNitroglycerinzyr2189No ratings yet
- Patient Information Intermittent Claudication and Exercise TherapyDocument11 pagesPatient Information Intermittent Claudication and Exercise TherapyRifat MahmudNo ratings yet
- Ventricular Septal DefectDocument43 pagesVentricular Septal DefectmalekNo ratings yet
- La Salle University Nursing Department Ozamiz CityDocument5 pagesLa Salle University Nursing Department Ozamiz CityNicole OrtegaNo ratings yet
- Summary and ConclusionDocument4 pagesSummary and Conclusionhamodi222No ratings yet
- ECG Lecture 4Document44 pagesECG Lecture 4asdasdasdasNo ratings yet
- Stroke CaseDocument1 pageStroke CasemphebanggrainiNo ratings yet
- Can't Miss ECG FindingsDocument61 pagesCan't Miss ECG FindingsVikrantNo ratings yet
- Try Out CompilationDocument17 pagesTry Out CompilationRendi RafsanjaniNo ratings yet
- AtherosclerosisDocument27 pagesAtherosclerosisAnonymous wesmz90Oh1No ratings yet
- Pi Is 0022347617311927Document1 pagePi Is 0022347617311927Umesh BabuNo ratings yet
- Research Poster PresentationDocument1 pageResearch Poster Presentationapi-328441669No ratings yet
- Case Scenario CHFDocument2 pagesCase Scenario CHFchetankumarbhumireddyNo ratings yet
- Examination of The Cardiovascular SystemDocument2 pagesExamination of The Cardiovascular Systemkenners98% (44)
- MURMURDocument21 pagesMURMURtoyyibNo ratings yet
- ECG Nutshell - Beta Free VersionDocument24 pagesECG Nutshell - Beta Free Versionnaveen prasanthNo ratings yet
- Verapamil HydrochlorideDocument3 pagesVerapamil HydrochlorideAndrea Huecas TriaNo ratings yet
- Cardiac Cycle & Heart Sounds Flashcards - QuizletDocument11 pagesCardiac Cycle & Heart Sounds Flashcards - QuizletRadijska Postaja KoprivnicaNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanMariel GamaloNo ratings yet
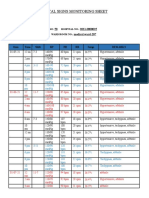
- Vital Signs Monitoring SheetDocument2 pagesVital Signs Monitoring SheetRenea Joy ArruejoNo ratings yet
- Congenital Heart Disease (Part I) : Shenzhou Hospital He LihuiDocument26 pagesCongenital Heart Disease (Part I) : Shenzhou Hospital He LihuiTaran JOt100% (1)
- Cardiology Board ReviewDocument6 pagesCardiology Board ReviewAousam Raouf100% (1)
- Heart Disease in Malaysia (2014) : Puteri Syazreen Athillah Nabilah HamidDocument2 pagesHeart Disease in Malaysia (2014) : Puteri Syazreen Athillah Nabilah HamidCIK FATHINNo ratings yet
- Stroke MsDocument57 pagesStroke MsAishwarya ShahNo ratings yet
- Icd 9 TindakanDocument6 pagesIcd 9 TindakanmirnaNo ratings yet
- Acute Coronary Syndrome: Case PresentationDocument4 pagesAcute Coronary Syndrome: Case PresentationJunathan L. DelgadoNo ratings yet
- Referat Terapi Hipertensi Restisten Elfarini 406151044Document19 pagesReferat Terapi Hipertensi Restisten Elfarini 406151044Elfa RiniNo ratings yet
- Nursing 202: Module B Cardiovascular System AlterationsDocument121 pagesNursing 202: Module B Cardiovascular System AlterationssenthilmnurseNo ratings yet
- 2 - AtherosclerosisDocument16 pages2 - AtherosclerosisUnnati PatelNo ratings yet