Professional Documents
Culture Documents
Jurnal 2
Jurnal 2
Uploaded by
ANASTA INSPIRASIOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Jurnal 2
Jurnal 2
Uploaded by
ANASTA INSPIRASICopyright:
Available Formats
Copyright 2012 American Nephrology Nurses’ Association (ANNA) All rights reserved.
No part of this document may be reproduced or transmitted in any form
without the written permission of the American Nephrology Nurses' Association.
Venous Needle Dislodgement Continuing Nursing
In Patients on Hemodialysis Education
Billie Axley
Joan Speranza-Reid
Helen Williams
emodialysis treatments have
H
Copyright 2012 American Nephrology Nurses’ Association
become routine, but complica-
tions still occur, ranging from Axley, B., Speranza-Reid, J., & Williams, H. (2012). Venous needle dislodgement in
the most common (headache, patients on hemodialysis. Nephrology Nursing Journal, 39(6), 435-445.
cramps) to the less frequent yet more
serious complication of substantial Venous needle dislodgement is a potential serious complication of hemodialysis therapy.
blood loss related to venous needle In 2012, the American Nephrology Nurses’ Association (ANNA) created a collaborative
dislodgement (sometimes abbreviat- special project workgroup to review venous needle dislodgement occurrence, conse-
ed as VND). Venous needle dislodge- quences, and recommended practices, and to develop strategies and resources on venous
ment happens when the venous fistu- needle dislodgement to be used by nephrology nurses and other healthcare professionals,
la needle becomes dislocated out of as well as by patients and their families. The ANNA Venous Needle Dislodgement
the vascular access, resulting in blood Special Project Workgroup conducted a literature review and also surveyed nephrology
loss. This can lead to a rapidly declin- nurses about their experiences with venous needle dislodgement and their recommenda-
ing blood volume in the patient and tions for needed resources. This article discusses the results of the literature review and
may cause morbidity and mortality if survey, and provides resources on venous needle dislodgement, including a venous nee-
not discovered quickly. At typical hemo- dle dislodgement risk assessment tool, education materials, and practice recommenda-
dialysis blood flow rates of 400 to 500 tions.
mL/minute, it can take only minutes
for the patient to lose over 40% of his Key Words: Venous needle dislodgement, hemodialysis, venous access site, end
or her blood volume (the point at stage renal disease, blood loss, taping techniques, bloodlines, needles,
which hemorrhagic shock occurs) catheters, patient education.
(Gutierrez, Reines, & Wulf-Gutierrez, Goal
2004). In a scientific abstract presented To provide an overview of venous needle dislodgement in patients undergoing
at the 2008 American Society of Neph- hemodialysis and prevention strategies.
rology (ASN), Sandroni, Sherockman,
Objectives
1. Describe the serious impact that can occur from venous needle dislodgement.
2. Explain the findings regarding incidence of venous needle dislodgement as discov-
Billie Axley, MSN, RN, CNN, is Director,
Quality and Initiatives, Fresenius Medical Care, ered by the ANNA Venous Needle Dislodgement Survey and Literature Review.
Franklin, TN, and a member of ANNA’s Music City 3. Discuss practice recommendations for nephrology nurses and other healthcare
Chapter. She may be contacted directly via e-mail at providers who treat patients undergoing hemodialysis.
billie.axley@fmc-na.com
Joan Speranza-Reid, BSHM, RN, CNN, is
Director of Renal Services, CVPH Medical Center,
Plattsburgh, NY, Hemodialysis Special Practice
Network Facilitator for ANNA, and a member of
ANNA’s Northeast TriState Chapter. This offering for 1.4 contact hours is provided by the American Nephrology Nurses’
Association (ANNA).
Helen Williams, MSN, RN, CNN, is an
Assistant and Special Projects Manager, Denver American Nephrology Nurses’ Association is accredited as a provider of continuing nursing
Acute Dialysis, Fresenius Medical Care, Denver, education by the American Nurses Credentialing Center Commission on Accreditation.
CO, Commissioner the Nephrology Nursing
Certification Commission, and a member of
ANNA is a provider approved by the California Board of Registered Nursing, provider number
ANNA’s High County Chapter. CEP 00910.
Accreditation status does not imply endorsement by ANNA or ANCC of any commercial product.
Statement of Disclosure: The authors reported no
actual or potential conflict of interest in relation to This CNE article meets the Nephrology Nursing Certification Commission’s (NNCC’s) continu-
this continuing nursing education activity. ing nursing education requirements for certification and recertification.
Nephrology Nursing Journal November-December 2012 Vol. 39, No. 6 435
Copyright 2012 American Nephrology Nurses’ Association (ANNA) All rights reserved. No part of this document may be reproduced or transmitted in any form
without the written permission of the American Nephrology Nurses' Association.
Venous Needle Dislodgement in Patients on Hemodialysis
and Hayes-Light (2008) reported venous needle dislodgement and dislodgement event can range from
from a study involving 300 patients advocated for staff and patient educa- minimal blood loss to a fatal hemor-
an observed incidence in their hospi- tion concerning the importance of rhage (Pennsylvania Patient Safety
tal system of one catastrophic hemor- keeping the patient’s access visible at Authority, 2010). In its analysis of
rhage resulting from venous needle all times. Education of all nephrolo- reports of bleeding during dialysis,
dislodgement per 126,718 treatments. gy/dialysis staff and patients on dialy- the VA National Center for Patient
The authors indicated if the annual sis on prevention of accidental line Safety found that 40 of the 47 events
incidence of such events nationally separation and venous needle dis- were termed “serious bleeding epi-
was similar to the incidence they lodgement were promoted as a “top sodes” (Veterans Health Administration,
observed, it could be estimated that priority during hemodialysis” by 2008, p. 1) (which they defined as
over 400 events occur annually in the Saibu and colleagues (2011, p. 515). more than 100 mL), many of which
United States (Sandroni et al., 2008). The risk of complications from “required hospital admission and
venous needle dislodgement is mag- some resulted in death of the patient”
Background nified by dislodgements that do not (Veterans Health Administration, 2008,
trigger a venous pressure alarm to p. 3). A series of articles directed to
Venous needle dislodgement has alert patient care staff or the patient the public concerning safety in dialy-
been described as “…a potentially (Sandroni et al., 2008). Venous needle sis by Fields (2010) included an article
life-threatening complication of dialy- dislodgement during hemodialysis that related the story of a patient on
sis…” (Hurst, 2011a, p. 148). An advi- without triggering a venous pressure dialysis who “never really recovered”
sory from the Pennsylvania Patient alarm was reported in an online med- from a loss of blood from her venous
Safety Authority (2010) indicated that ical device safety report from 1998 “tube” and spotlighted the event as a
32 event reports involving needle dis- that described “…the back pressure “catastrophic hemorrhage during
connections were received during a created by the narrow-bore needles treatment” (p. 2). Fields (2010) also
one-year period from November 1, prevented the machine’s venous pres- reported that ProPublica examined
2008, through October 31, 2009. sure monitors from sensing the loss of records for more than 1500 dialysis
These submitted events represented pressure created by the dislodge- clinics in five states from 2002-2009
6.1% of all hemodialysis events ment” (ECRI Institute, 1998, p 1). and found at least one fatality that
reported to the Pennsylvania Patient The report continued to say that even resulted from needle dislodgements
Safety Authority during that period. if the venous needle is fully or partial- in each of the five states plus “dozens
These data were limited to reports ly dislodged from the patient, the of additional cases in which patients
from hospital-operated dialysis facili- venous pressure monitor is likely to required hospitalization, blood trans-
ties (Pennsylvania Patient Safety continue sensing the pressure created fusions, or other emergency interven-
Authority, 2010). A Patient Safety by the needle’s flow resistance. The tions” (p. 4). Fields (2010) also de-
Advisory from the U.S. Department conclusion of the ECRI Institute scribed the compelling physical and
of Veterans Affairs (VA) in 2008 report indicated that although the psychosocial suffering of five patients
reviewed 47 root cause analyses and venous pressure monitor may be able on hemodialysis and their families
safety reports received from March 1, to reliably detect a large pressure due to line separations, needle dis-
2002, to April 30, 2008, that con- change, needle flow resistance makes lodgement, and staff error that result-
cerned bleeding episodes during the it “unlikely” for the monitor to detect ed in significant blood loss during a
hemodialysis treatment. In this analy- the smaller drop in pressure associat- dialysis procedure. Hurst (2009) has
sis, the 47 reported patient events ed with needle dislodgement (ECRI advocated that just as fire drills are
“…involved dislodgement of the Institute, 1998). In addressing unde- practiced and smoke detectors are
venous needle or disconnection of the tected venous needle dislodgement, used to prevent harm, the healthcare
venous bloodline at the dialysis the ECRI Institute (1998) stated the community must learn from past
catheter attachment” (Veterans Health problem was not unique to any specif- venous needle dislodgement inci-
Administration, 2008, p. 3). In its ic brand or model of hemodialysis dents, be vigilant, and use available
2006 End Stage Renal Disease machines or tubing sets. The VA, in technologies to provide safe care.
(ESRD) Patient Survey, the Renal its Patient Safety Advisory on bleed-
Physicians Association (RPA) (2007) ing episodes during dialysis, found ANNA Venous Needle
found that 5.1% of the 1056 patients similar general information from the Dislodgement Special Project
responded positively when asked if majority of its analyzed events. There Workgroup
the needle had ever, in the last three was no statistical difference between
months, come out of their access site the incidence of complications and The American Nephrology Nurses’
before their dialysis treatment was fin- the brand of dialysis machine in- Association (ANNA) convened a col-
ished. volved in their analysis (Veterans laborative special project workgroup,
Saibu and colleagues (2011) re- Health Administration, 2008). the ANNA Venous Needle Dislodge-
ported a patient death resulting from Consequences of a venous needle ment Special Project Workgroup, to
436 Nephrology Nursing Journal November-December 2012 Vol. 39, No. 6
Copyright 2012 American Nephrology Nurses’ Association (ANNA) All rights reserved. No part of this document may be reproduced or transmitted in any form
without the written permission of the American Nephrology Nurses' Association.
review recommendations of care for ANNA Venous Needle ed they were concerned about venous
venous needle dislodgement preven- Dislodgement Survey Results needle dislodgement very often or
tion and detection, and to present Responses were received from often (see Table 3). An additional
these recommendations in easy-to-use 1173 nephrology nurses. Over 70% of 23.1% rated their concern as occa-
tools. A literature review was per- respondents reported they practiced sional. Of the 1156 survey respon-
formed for occurrences and conse- in chronic hemodialysis and 43.1% in dents to the question about the poten-
quences of venous needle dislodge- acute care (the percentages exceeded tial benefit of a venous needle dis-
ment and to identify best practice rec- 100% because respondents were lodgement risk assessment, 71.2% (n =
ommendations for prevention of asked to identify all areas in which 823) indicated they would find such a
venous needle dislodgement. To gath- they practice) (see Table 1). The tool to be beneficial. To the question
er information from nephrology nurs- ANNA Venous Needle Dislodgement about the benefit of education materi-
es on the occurrence and implications Survey results revealed that 76.6% al on how to reduce the risk of venous
of venous needle dislodgement in the (n = 894) of the 1166 responders to needle dislodgement, a resounding
hemodialysis population, the ANNA the survey question about observanc- 85.3% (n = 996) of the responders
Venous Needle Dislodgement Special es of venous needle dislodgement indicated that education material
Project Workgroup developed the indicated they had seen a venous nee- would be of benefit. The survey also
ANNA Venous Needle Dislodgement dle dislodgement in the past five offered respondents the opportunity
Survey and distributed it to the years, with 8.2% (n = 96) of these hav- to share additional comments about
ANNA nephrology nurse member- ing seen five events or more in this venous needle dislodgement. The
ship. Questions included in the sur- time period (see Table 2). Slightly respondents offered their views of cri-
vey were: more than half (57.9%) of the 1162 teria for patients they thought were at
• Identification of practice area. respondents to the question of how risk for venous needle dislodgement,
• Have you seen a venous needle often they were concerned about factors that contributed to the
dislodgement in the past five venous needle dislodgement indicat- patient’s risk, and interventions they
years?
• How often are you concerned
about venous needle dislodge- Table 1
ment? ANNA Venous Needle Dislodgement Survey:
• Would a screening tool assist you Respondent Practice Areas
in the assessment of a patient’s
risk of venous needle dislodge- Chronic Hemodialysis 70.7% (827)
ment and be of benefit to you? Acute Care 43.1% (504)
• Would educational material on Nursing Education 8.4% (98)
how to reduce the risk of venous Continuous Renal Replacement Therapy 8.3% (97)
needle dislodgement be of bene-
Therapeutic Apheresis 4.4% (51)
fit to you?
• Please share additional com- Pediatric Nephrology 3.7% (43)
ments about venous needle dis- Other Areas with less than 3% 11.7% (140)
lodgement. *Respondents were asked to list all of their practice areas. There were 1783
responses from 1170 respondents, indicating that many respondents work in multi-
ple areas.
Table 2
ANNA Venous Needle Dislodgement Survey: Observed Venous Needle Dislodgements
Have you seen a venous needle dislodgement in the past five years?
Acute Care Chronic Hemodialysis
All Respondents Practice Area Practice Area
Yes, 1 to 2 times 50.0% (583) 52.0% (262) 50.0% (412)
Yes, 3 to 4 times 18.4% (215) 16.3% (82) 21.4% (176)
Yes, 5 or greater times 8.2% (96) 8.7% (44) 8.8% (72)
No 23.3% (272) 23.0% (116) 19.8% (163)
Total Respondents to the Question 1166 504 823
Nephrology Nursing Journal November-December 2012 Vol. 39, No. 6 437
Copyright 2012 American Nephrology Nurses’ Association (ANNA) All rights reserved. No part of this document may be reproduced or transmitted in any form
without the written permission of the American Nephrology Nurses' Association.
Venous Needle Dislodgement in Patients on Hemodialysis
Table 3 Patients who experience hypo-
ANNA Venous Needle Dislodgement Survey: tension or muscle cramps during
Concern about Venous Needle Dislodgement treatment.
• Needle security is at risk with
How often are you concerned about venous needle dislodgement? excessive movement of the ac-
Very Often 34.8% (404) cess limb.
• The patient may become dia-
Often 23.1% (269)
phoretic, causing the tape to
Occasionally 23.1% (269) loosen.
Seldom 17.8% (207)
Never 1.1% (13) Patients who refuse to keep the
Total Responses 1162 access areas and bloodlines uncov-
ered.
• Lascano and Anderson (2011)
Table 4 addressed the importance of en-
Summary of Risk Factors Associated with Venous suring that the patient’s access
Needle Dislodgement and needles are visible at all
times.
• Confused, restless, agitated patients; patients who are cognitively impaired, • The issue of patients who fall
and patients with dementia asleep with their access covered,
• Patients who experience hypotension or have muscle cramps during treatment resulting in unintended access
• Patients who refuse to keep the access areas and bloodlines uncovered limb movement and dislodgement,
was mentioned multiple times as
• Taping technique
a risk for venous needle dislodge-
• Staff observation ment in the ANNA Venous
• Patients on nocturnal and/or home hemodialysis Needle Dislodgement Survey.
• Visibility was noted as an issue in
the VA analysis (Veterans Health
perceived would reduce that risk. The Confused, restless, agitated Administration, 2008).
literature review supported the infor- patients; patients who are cogni- • Intentional dislodgement by a
mation obtained in the ANNA tively impaired; and patients with patient was mentioned several
Venous Needle Dislodgement Survey dementia. times as a risk in the ANNA Ve-
responses. • The VA analysis of root cause nous Needle Dislodgement Survey.
analysis and safety reports of
bleeding during dialysis at VA Taping technique.
Information from the ANNA Venous
dialysis centers found that “75% • ANNA Venous Needle Dislodge-
Needle Dislodgement Survey and
of the most significant bleeds ment Survey respondents repeat-
The Literature Review
occurred in patients who were edly indicated that taping tech-
restless, confused, agitated, or nique was critical to prevent
Assessment of the Risk uncooperative” (Veterans Health venous needle dislodgement.
Van Waeleghem, Chamney, Lindley, Administration, 2008, p. 1). Factors related to securing the
Olausson, & Pancirova (2008) recom- • Lascano and Anderson (2011) needles included an access that is
mended that all patients be assessed reported that high-acuity patients in a difficult location or has a
for their level of risk for venous nee- with altered mental status are at a deep angle of cannulation.
dle dislodgement. Risk factors associ- higher-than-average risk for venous • A Cleveland Clinic improvement
ated with venous needle dislodge- needle dislodgement. This in- project included training staff on
ment have been identified in the cludes patients who may be con- anchoring needle taping tech-
ANNA Venous Needle Dislodgement fused because of Alzheimer’s dis- nique (Lascano & Anderson,
Survey along with multiple journal ease. Other conditions, such as 2011).
articles and publications reviewed in sedation or infection, can also • Preparing the skin and the cor-
the literature review (see Table 4) lead to an altered mental state. rect technique for the secure tap-
(Amato, Hlebovy, King, & Salai, Patients with a reduced level of ing of the access needles are
2008; Gomez, 2011; Hurst, 2009, consciousness and communica- addressed in the ANNA Core
2011a; Laird, 2011; Lindley, 2005; tion challenges may not be able Curriculum for Nephrology Nursing
McCabe, McArtney, Lomas, & Moir, to alert staff to a problem. (Dinwiddie, 2008).
2009; Sandroni, 2005; Sandroni et al., • The ANNA Venous Needle Dis-
2008; RPA, 2007). lodgement Survey results indi-
438 Nephrology Nursing Journal November-December 2012 Vol. 39, No. 6
Copyright 2012 American Nephrology Nurses’ Association (ANNA) All rights reserved. No part of this document may be reproduced or transmitted in any form
without the written permission of the American Nephrology Nurses' Association.
cated that patients with excessive Patients on nocturnal and/or and patients should be aware of
hair in the access taping areas on home hemodialysis. venous needle dislodgement and its
may experience loosening of the • Hurst (2011b) has discussed possible consequences, and also
tape securing the needle(s) during venous needle dislodgement pre- advocated for the education of pa-
the hemodialysis treatment. One vention for the home hemodialy- tients/family as a “fundamental” role
experience with tape seeming to sis population and suggested that of the nephrology nurse.
lose its adherence to the patient’s patients should not rely solely on Dialysis provider organizations
skin was described as loosening the dialysis machine’s internal should each develop evidence-based
over time into the treatment. alarm. Hurst (2011b) urged in- policies and procedures that are
• Patients who experience sweating creased “awareness and vigi- designed to foster a safe and effective
(such as the sweating that can lance” by anyone who receives treatment environment for the pa-
occur with hypotension or in a dialysis and their caregivers. tient. To ensure safe care, it is essential
patient with diabetes who experi- • A number of ANNA Venous that opportunities are provided for
ences hypoglycemia) have been Needle Dislodgement Survey staff to learn about these expectations
identified as at risk for loosening respondents described using a and be updated on venous needle dis-
of the tape that is securing the device that can detect blood loss lodgement recommended practices
needles (Van Waeleghem et al., to the environment to monitor and technologies on a regular basis.
2008). the venous needle access site of
• The ANNA Venous Needle Dis- patients on nocturnal and home Practice Recommendations
lodgement Survey respondents hemodialysis.
indicated even a small amount of • Laird (2011) recommended that Based on the literature review
leakage around the needle site patients on nocturnal hemodialy- and the results of the ANNA Venous
can cause tape to become loos- sis use an approved moisture Needle Dislodgement Survey, there
ened, increasing the risk of alarm device during their hemo- are important practice recommenda-
venous needle dislodgement. dialysis treatments in addition to tions that can be implemented to pre-
doing proper taping. Laird (2011) vent venous needle dislodgement.
Staff observation. also advocated for patients keep-
• Patient observation by the staff ing needle insertion sites and Prepare for Cannulation
was noted as a risk factor by res- bloodlines visible during the Of the Access Sites
pondents to the ANNA Venous hemodialysis procedure, not tap- Cleaning of the selected access
Needle Dislodgement Survey. ing bloodlines to an object, and cannulation sites and allowing the
not disabling pressure alarms on areas to dry before cannulation serves
Staffing. the dialysis machine. a dual purpose. Removal of bacteria
• Ensuring adequate staff-to-patient from the skin helps prevent access
staffing ratios to allow routine Education and Awareness infection. Some disinfectant solutions
monitoring of the patient’s access must be allowed to dry to be effective.
during the hemodialysis treat- Venous needle dislodgement was Allowing adequate time for the site to
ment was a recommendation of evidenced in the literature as a com- dry before performing cannulation
respondents in the ANNA Venous plication of hemodialysis with poten- also helps to prepare the skin surface
Needle Dislodgement Survey. tial for harm. Multiple factors were so the tape will be better able to ad-
• The importance of monitoring of identified that can contribute to the here (Dinwiddie, 2008; Van Waeleghem
the patient’s access as a factor risk of venous needle dislodgement. et al., 2008).
affecting the risk of venous needle This reality demands a combination
dislodgement was noted by Van of vigilance in monitoring and ongo- Tape the Needles Securely
Waeleghem et al. (2008), who ing assessment of the patients, the Taping the needles securely is
recommended that all patients dialysis machines, and other tech- key to preventing dislodgement
should be monitored routinely nologies that nephrology nurses use (Lindley et al., 2010a; Mactier &
and that higher risk patients and manage. Lascano and Anderson Worth, 2007). The use of a chevron
require a higher level of observa- (2011) indicated that expectations of taping configuration is indicated as a
tion. this high level of nursing care can method to secure the needle in the
• Regarding staffing, Hurst (2011a) only be achieved when staff have access vessel (Hurst, 2011b; Laird,
noted that venous needle dis- been provided with education about 2011; Van Waeleghem et al., 2008).
lodgement can occur any time the importance of the “safety first” General guidelines for securing
and anywhere, and can happen message as it relates to venous needle hemodialysis access needles can be
in “apparently routine treatments dislodgement. Van Waeleghem et al. found in the ANNA Core Curriculum for
and with fully staffed units” (p. 149). (2008) listed as their first practice rec- Nephrology Nursing (Amato et al.,
ommendation that patient care staff 2008). Mactier and Worth (2007)
Nephrology Nursing Journal November-December 2012 Vol. 39, No. 6 439
Copyright 2012 American Nephrology Nurses’ Association (ANNA) All rights reserved. No part of this document may be reproduced or transmitted in any form
without the written permission of the American Nephrology Nurses' Association.
Venous Needle Dislodgement in Patients on Hemodialysis
reported on results from discussion of access sites and line connections change the venous pressure alarm
procedures for prevention of venous should remain uncovered to allow staff limit range. It was indicated in the lit-
needle dislodgement at a Venous to visually monitor these areas to erature that it could be helpful in
Needle Dislodgement Workshop that ensure patient safety” (U.S. De- monitoring for venous needle dis-
took place in the United Kingdom in partment of Health and Human lodgement to set the limits in an asy-
2006. This workshop was held after Services [(DHHS], & Centers for mmetrical pattern (such as -30/+70)
“…9 units had experienced 10 Medicare & Medicaid Services [CMS], with the lower limit of the venous
episodes of fistula needle dislodge- 2008, p. 20384). If there is venous nee- pressure alarm as close as possible to
ment in 6 months” (Mactier & Worth, dle dislodgement, patients and staff the current venous pressure. This
2007, p. 9). While the authors indicat- will be able to visualize the event and may increase the possibility of the
ed that a specific method for securing take action immediately (Lindley et al., machine sounding an alarm if a ve-
access needles was not agreed upon at 2010b). Access checks should be part nous needle dislodgement occurs
the workshop, what was agreed upon of regular rounds to be sure the access (Hurst, 2009; Mactier & Worth, 2007;
was that the dialysis units should needles are in the vessels and securely Van Waeleghem et al., 2008).
develop their own clear guidelines for taped (Hurst, 2009; Pennsylvania
securing access needles (Mactier & Patient Safety Authority, 2012). Monitor Dialysis Catheters
Worth, 2007). Monitoring catheter accesses
Use of Dialysis Machine Safety should be included in the nephrology
Replace Tape if Repositioning Devices nurses’ ongoing risk assessment of
The Needle Hemodialysis machines have venous needle dislodgement. Cathe-
The tape should not just be loos- methods of displaying the measure- ters have luer lock connections that
ened and then re-used after making a ment of venous pressure during the can be a source of blood loss if they
needle adjustment. This tape may dialysis treatment with a default range are not connected tightly or if the luer
have lost its stickiness in the process, for alarm parameters. However, re- lock is not threaded properly. Clip
leaving the tape and the needle only ported incidents of venous needle dis- devices have been used to help hold
loosely in contact with the skin. Fresh lodgement without a machine alarm the catheter ports and bloodlines
tape should be applied to ensure the sounding are found in the literature together and to prevent disconnec-
security of the needle (Van Waeleghem (ECRI Institute, 1998, Mactier & tion (Fields, 2010).
et al., 2008). Worth, 2007, Sandroni, 2005). Sev-
eral authors have indicated that the Use of Moisture Monitors
Secure Bloodlines machines involved in venous needle Enuresis pads, designed for
In their article on venous needle dislodgements were tested after the detecting moisture, have been des-
dislodgement and how to minimize incidents, only to find that the alarms cribed as having been used off-label
the risk, Van Waeleghem et al. (2008) were functioning and responded cor- in an attempt to protect high-risk
indicated that the bloodlines should rectly within the default alarm limits patients from venous needle dislodge-
be looped loosely “…to allow move- (Sandroni, 2005; Sandroni, et al., 2008; ment; however, these pads have been
ment of the patient and to prevent Van Waeleghem et al., 2008). Van found incapable of detecting very
bloodline pulling on the needles” (p Waeleghem and colleagues (2008) small volumes of moisture, making
164). Keeping the bloodlines taped/ concluded that even when the alarm them ineffective as an early warning
attached to the patient was suggested limits are set, the drop in venous pres- device for blood leaks (Hurst, 2009;
as an intervention to help prevent an sure may be too small to activate the Sandroni, 2005; Van Waeleghem et
accidental dislodgement in the simple alarm, for example, when “…the al., 2008).
act of shifting position in a chair or access pressure is too low or because
rolling over in a bed. Bloodlines the needle is incompletely dislodged Use of a Detection Device for
should be secured to the patient dur- or obstructed by material covering Blood in the Environment
ing treatment and not secured to an the needle sites” (p. 166). The venous A number of researchers have
object, such as the dialysis chair, blan- pressure alarm safety feature cannot recommended the use an FDA-ap-
kets, or the bed rail (RPA, 2012a, be used as the only defense for proved device for blood in the envi-
2012b; Sandroni et al., 2008; Van venous needle dislodgement. Vigil- ronment with high-risk patients and
Waeleghem et al., 2008). ance and monitoring by staff are for patients doing home hemodialysis
essential to provide safety from this (Ahlmen et al., 2008; Cowperthwaite,
Assure Access Visibility potential complication (Veterans Rivers, Sundstrom, & Hegbrant,
It is essential for the access to be Health Administration, 2008) 2011; Fields, 2010; Hurst, 2009;
visible at all times (Gomez, 2011; RPA, Sandroni et al., 2008). An FDA-
2007). The April 18, 2008, Medicare Set the Venous Pressure approved safety device, Redsense®, is
Final Rule for Conditions for Alarm Limit specifically designed for use on a dial-
Coverage statement includes “…the Some machines allow the user to ysis access to detect blood loss at the
440 Nephrology Nursing Journal November-December 2012 Vol. 39, No. 6
Copyright 2012 American Nephrology Nurses’ Association (ANNA) All rights reserved. No part of this document may be reproduced or transmitted in any form
without the written permission of the American Nephrology Nurses' Association.
access site and sound an alarm if it ing recommendations in easy-to-use staff, patients, and other caregivers
occurs. The device is connected by an tools to assist healthcare providers (see Figure 2). The recommendations
optic fiber to a sensor patch with and patients to proactively minimize start with the need to be aware of risk
adhesive that allows it to be placed on the risk of venous needle dislodge- factors for venous needle dislodge-
the venous needle site (Ahlmen et al., ment. A venous needle dislodgement ment and the consequences of venous
2008). The manufacturer’s literature risk assessment tool for nephrology needle dislodgement. Recommen-
indicates this device is able to detect nurses from the European Dialysis dations progress from preparing the
as little as 1 mL of blood (Takeuchi et and Transplant Nurses Association/ needle sites to securely taping the
al., 2010). European Renal Care Association needles, securing and positioning the
These practice recommendations (EDTNA/ERCA) (2010) was adapted bloodlines, maintaining visibility, and
for the prevention of venous needle and revisions made based upon the monitoring the access during treat-
dislodgement are supported in the ANNA Venous Needle Dislodgement ment. The tool concludes with venous
ANNA Core Curriculum for Nephrology Survey recommended risk criteria. A pressure monitoring recommenda-
Nursing, with recommendations to poster for patient care staff education tions and technologic advancements
securely lock luer lock connections on from the EDTNA/ERCA work was of devices intended to detect blood
all bloodlines and access lines; con- adapted and revised based upon loss to the environment from dis-
nect both arterial and venous blood- nephrology nurses’ indications of rec- lodgement of the venous needle.
lines to access lines at the initiation of ommended practices to reduce the Dialysis staff who have an under-
the hemodialysis treatment; and risks for venous needle dislodgement. standing of the risks of venous needle
achieve complete stasis of access nee- In addition, a patient education tool dislodgement and strategies to reduce
dle sites before the patient leaves was developed to assist in education these risks can discuss the risks and
and/or clamp and cap central venous of patients/family on how they can strategies with patients, families, and
catheters limbs (Dinwiddie, 2008). help to minimize their risk of venous other healthcare providers. The
ANNA’s Nephrology Nursing Scope needle dislodgement during hemo- ANNA Venous Needle Dislodgement
and Standards of Practice (Gomez, dialysis. Special Project Workgroup developed
2011) indicate that the nursing assess- The tools adapted and revised by an education tool, Help Us Keep You
ment should include the integrity of the ANNA Venous Needle Dislodge- Safe!, that can be used as a handout as
the extracorporeal circuit, connec- ment Special Project Workgroup are well as a poster in the dialysis unit to
tions, and delivery system alarms, designed to present recommended assist in initiating this important discus-
and monitoring of the patient practices as supported by current lit- sion (see Figure 3). This patient educa-
throughout the hemodialysis treat- erature and as reported in nurses’ tion resource was designed as a simple
ment. In addition, patient teaching experiences with venous needle dis- and visual message for the education
recommendations with consideration lodgement obtained from the ANNA of patients and families of their roles in
of the patient and family’s health liter- Venous Needle Dislodgement Survey. helping the patient care staff keep
acy should include the patient’s role These tools have been provided in patients safe during treatment.
in safe delivery of treatment, such as the format of a pocket card, a poster, All three of these resources were
being aware of the effects of move- and a one-page handout. designed to serve as reminders of
ment on the access and the need to The pocket card is entitled how patients can be at risk for venous
keep the access site and extracorpore- “Assessment of the Risk for a Serious needle dislodgement and to provide
al connections uncovered. The Venous Needle Dislodgement Inci- recommendations for how to mini-
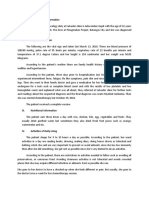
nephrology nursing process of care dent” (see Figure 1). The literature mize the risk of venous needle dis-
for hemodialysis should include an supports the need for assessing the lodgement.
individualized approach to educate patient for potential risk of venous
patients and families regarding signs needle dislodgement as key to pre- Conclusion
and symptoms that should be venting its occurrence (Lindley, 2005;
promptly reported to patient care staff McCabe et al., 2009). The “Assess- A literature review and the results
(Gomez, 2011). ment of the Risk” tool is designed to of the ANNA Venous Needle Dis-
assist the nephrology nurse in per- lodgement Survey validate venous
Resources forming a four-level assessment of needle dislodgement as a potential
patient risk and to provide recom- complication of hemodialysis thera-
In response to the ANNA Ve- mendations for interventions that cor- py. Patient care staff and patient
nous Needle Dislodgement Survey relate with each of four identified awareness of the risk have been iden-
and the literature review, the ANNA patient levels of risk. tified in the literature review, and the
Venous Needle Dislodgement Special The poster, Venous Needle Dis- ANNA Venous Needle Dislodgement
Project Workgroup reviewed existing lodgement (VND): How to Minimize the Survey is an important factor in the
venous needle dislodgement educa- Risks, was designed to provide prac- prevention of venous needle dis-
tion materials with the goal of provid- tice recommendations for patient care lodgement.
Nephrology Nursing Journal November-December 2012 Vol. 39, No. 6 441
Copyright 2012 American Nephrology Nurses’ Association (ANNA) All rights reserved. No part of this document may be reproduced or transmitted in any form
without the written permission of the American Nephrology Nurses' Association.
Venous Needle Dislodgement in Patients on Hemodialysis
Figure 1
Pocket Card: Assessment of the Risk for a Serious Venous Needle Dislodgement Incident
442 Nephrology Nursing Journal November-December 2012 Vol. 39, No. 6
Copyright 2012 American Nephrology Nurses’ Association (ANNA) All rights reserved. No part of this document may be reproduced or transmitted in any form
without the written permission of the American Nephrology Nurses' Association.
Figure 2
Poster from the ANNA Venous Needle Dislodgement Special Project Workgroup
Nephrology Nursing Journal November-December 2012 Vol. 39, No. 6 443
Copyright 2012 American Nephrology Nurses’ Association (ANNA) All rights reserved. No part of this document may be reproduced or transmitted in any form
without the written permission of the American Nephrology Nurses' Association.
Venous Needle Dislodgement in Patients on Hemodialysis
Figure 3
References
Patient Education Resource: Help Us Keep You Safe! Amato, R.L., Hlebovy, D., King, B. &
Salai, P.B. (2008). Hemodialysis. In
C.S. Counts (Ed.) Core curriculum for
nephrology nursing (pp. 622-734).
Pitman, NJ: American Nephrology
Nurses’ Association.
Ahlmen, J., Gydell-Leight, K., Hadimeri,
H., Hernandez, H., Rogland, B., &
Strombom, U. (2008). A new safety
device for hemodialysis. Hemodialysis
International, 12, 264-267.
Cowperthwaite, J., Rivers, A., Sundström,
M., & Hegbrant, J. (2011, February
11). Assessment of a device to detect
venous needle dislodgement (VND).
Abstract presented at the Meeting of
the Annual Dialysis Conference,
Phoenix, AZ.
Dinwiddie, L.C. (2008). Vascular access
for hemodialysis. In C.S. Counts
(Ed.) Core curriculum for nephrology
nursing (pp. 756-758). Pitman, NJ:
American Nephrology Nurses’
Association.
ECRI Institute. (1998). Undetected venous
line needle dislodgement during
hemodialysis. Medical device safety
reports (online). Retrieved from
http://www.mdsr.ecri.org/summa-
ry/detail.aspx?doc_id=8300
European Dialysis and Transplant Nurses
Association/European Renal Care
Association (EDTNA/ERCA) (2010,
September 20). Venous needle dislodge-
ment (VND) recommendations for renal
nurses on how to minimize the risks.
Venous Needle Dislodgement Work-
group. Poster session presented at the
39th Annual Meeting of EDTNA/
ERCA, Dublin, Ireland.
Fields, R. (2010). When needles dislodge,
dialysis can turn deadly. Retrieved from
http://www.propublica.org/article/w
hen-needles-dislodge-dialysis-can-
turn-deadly
Gomez, N.J. (Ed.) (2011). Nephrology
nursing process of care – Hemo-
dialysis. Nephrology nursing scope and
As a result, the ANNA Venous ment of patients and family members standards of practice (7th ed., pp. 132-
Needle Dislodgement Special Project to minimize the risks of venous nee- 138). Pitman, NJ: American Nephro-
logy Nurses’ Association.
Workgroup developed a tool contain- dle dislodgement in hemodialysis. Gutierrez, G., Reines, H.D., & Wulf-
ing recommendations for the assess- Nephrology nurses must lead the Gutierrez, M. (2004). Clinical re-
ment of the risk of venous needle dis- way in their essential roles of working view: Hemorrhagic shock. Critical
lodgement and an education resource collaboratively with all patient care Care, 8(5), 373-381.
with proactive recommendations that staff, patients, and families to reduce Hurst, J. (2009). It can happen without
can be utilized by all patient care staff the significant and potentially fatal warning: Venous needle dislodge-
collaboratively to minimize the risk of complication that can occur from loss ment. Renal Business Today, 4(9), 18-
venous needle dislodgement. The of blood due to venous needle dis- 22.
patient education resource can be of lodgement. Hurst, J. (2010). A costly complication:
value for the education and engage- Venous needle dislodgement. Renal
Business Today, 5(9), 18-22.
444 Nephrology Nursing Journal November-December 2012 Vol. 39, No. 6
Copyright 2012 American Nephrology Nurses’ Association (ANNA) All rights reserved. No part of this document may be reproduced or transmitted in any form
without the written permission of the American Nephrology Nurses' Association.
Hurst, J. (2011a). Venous needle dislodge- International Conference, Hamburg, Journal of the American Society of
ment: A universal concern. European Germany. Nephrology, 19(Abstract Issue), 891A.
Nephrology, 5(2), 148-151. Retrieved Pennsylvania Patient Safety Authority. Retrieved from http://www.asn-
from http://www.touchbriefings.com/ (2010). Hemodialysis administration: online.org/education/kidneyweek/ar
ebooks/A1uupa/euneph52/ Strategies to ensure safe patient care. chives
Hurst, J. (2011b). Venous needle dislodge- Pennsylvania Patient Safety Authority, Takeuchi, A., Ishida, K., Morohoshi, Y.,
ment precautions. AAKP Renalife, 7(3), 87-96. Shinbo, T., Hirose, M., & Ikeda, N.
28(1). 8-9. Retrieved from http:// Renal Physicians Association (RPA). (2010). Study of light transmission
www.aakp.org/userfiles/File/AAKP_ (2007). Health and safety survey to through gauze pad effected by blood
Renalife-July%202011%20%20Final. improve patient safety in end stage renal or liquids to detect needle dislodge-
pdf disease: Report of findings from the ment [Abstract]. Journal of Clinical
Laird, P. (2011, November 1). Taking ESRD patient survey. Rockville, MD: Monitoring & Computing, 24, 35-39.
hemodialysis home safely. Renal Author. U.S. Department of Health and Human
Business Today. Retrieved from Renal Physicians Association (RPA). Services (DHHS), & Centers for
http://www.renalbusiness.com/arti- (2012a). Dialysis safety: What patients Medicare & Medicaid Services
cles/2011/10/taking-hemodialysis- need to know. Retrieved from (CMS). (2008).Centers for Medicare
home-safely.aspx http://www.kidneypatientsafety.org & Medicaid Programs; Conditions of
Lascano, M., & Anderson, M.B. (2011, Renal Physicians Association (RPA). coverage for end stage renal disease
November 11). Venous needle dislodge- (2012b). Keeping kidney patients safe: facilities; Final Rule (42 CFR Parts
ment prevention in hospital based RPA-Includes venous needle dislodgement 405, 410, 413 et al.). Federal Register,
hemodialysis. Abstract presented at as one of six main areas of patient safety 71(73), 20384. Retrieved from http://
the meeting of the American Society concern in hemodialysis. Retrieved from www.cms.hhs.gov/CfCsAndCoPs/D
of Nephrology, Philadelphia, PA. http://www.kidneypatientsafety.org ownloads/ESRDfinalrule0415.pdf
Lindley, E.J. (2005). Venous needle dislodge- Saibu, R., Mitchell, P., Alleyne, J., Van Waeleghem, J.P., Chamney, M.,
ment during hemodialysis: An unresolved Blackman, J., DeConcilio, K.,Joseph, Lindley, E.J., Olausson, S., &
risk of catastrophic hemorrhage. Re- A., & Salifu, M.O. (2011). Dialysis Pancirova, J. (2008). Venous needle
trieved from http://www/edtnaer- line separation: Maximizing patient dislodgment: How to minimize the
ca.org/pages/education/journal- safety through education and visibili- risks. Journal of Renal Care, 34(4), 163-
club/summary2005_2php ty of access site for patients on 168.
Lindley, E.J., Chamney, M., Olausson, S., hemodialysis. Nephrology Nursing Jour- Veterans Health Administration. (2008).
Pancirova, J., Sundstrom, M., nal, 38(6), 515-519, 526. Patient safety advisory: Bleeding episodes
Tattersall, J.E., & Van Waeleghem, Sandroni, S. (2005, June). Venous needle dis- during dialysis. Retrieved from http:/
J.P., on behalf of the EDTNA/ERCA lodgement during hemodialysis: An unre- /www.patientsafety.gov/alerts/Bleed
VND Project Group. (2010a, solved risk of catastrophic hemorrhage. ingEpisodesDuringDialysisAD09-
September 20). Venous needle dislodge- Briefing paper presented for discus- 02.pdf
ment survey Part 1: Frequency and prac- sion for the EDTNA/ERCA Journal
tice patterns. Presented at the meeting Club. Additional Reading
of the 39th Annual EDTNA/ERCA Sandroni, S., Sherockman, T., & Hayes- Lascano, M.E. (2011). Keeping kidney pa-
Conference, Dublin, Ireland. Light, K. (2008). Catastrophic hem- tients safe: Venous needle dislodgement.
Lindley, E.J., Chamney, M., Olausson, S., orrhage from venous needle dis- Retrieved from http://www.kidney-
Pancirova, J., Sundstrom, M., Tattersall, lodgement during hemodialysis: pateintsafety.org
J.E., & Van Waeleghem, J.P. on Continued risk of avoidable death
behalf of the EDTNA/ERCA VND and progress toward a solution.
Project Group. (2010b, September
20). Venous needle dislodgement survey
Part 2: Risk factors and outcomes.
Presented at the Meeting of the 39th
Nephrology Nursing Journal Editorial Board Statements of Disclosure
Annual EDTNA/ERCA Conference,
Dublin, Ireland. In accordance with ANCC governing rules Nephrology Nursing Journal Editorial Board statements of disclosure
Mactier, R., & Worth, D. (2007). Mini- are published with each CNE offering. The statements of disclosure for this offering are published below.
mizing the risks of needle dislodge- Deborah H. Brooks, MSN, APN-BC, CNN-NP, disclosed that she is on the Consultant Presenter Bureau and the
ment during haemodialysis. Artery, Advisory Board for Affymax, Inc.
41(3). 9-13. Paula Dutka, MSN, RN, CNN, disclosed that she has received grant/research support from Keryx, Amgen,
McCabe, M., McArtney, S., Lomas, K., & Rockwell, Fibrogen, Dynovox, and Otsuka; and she is on the Consultant and Presenter Bureau and the
Moir, C. (2009, September 8). Nephrology Nurse Advisory Board for Affymax/Takeda.
Minimizing the risk of venous needle dis- Patricia B. McCarley, MSN, RN, ACNPc, CNN, disclosed that she is on the Consultant Presenter Bureau for
lodgement using a patient risk assessment Amgen, Genzyme, and OrthoBiotech. She is also on the Advisory Board for Amgen, Genzyme, and Roche and
tool. Abstract presented at the is the recipient of unrestricted educational grants from OrthoBiotech and Roche.
Meeting of 38th EDTNA/ERCA
Nephrology Nursing Journal November-December 2012 Vol. 39, No. 6 445
You might also like
- Time ManagementDocument54 pagesTime Managementsalhum100% (3)
- VND ArticleDocument11 pagesVND ArticleAmbar RahmanNo ratings yet
- Venous Thromboembolism in Patients Discharged From The Emergency Department With Ankle FracturesDocument13 pagesVenous Thromboembolism in Patients Discharged From The Emergency Department With Ankle FracturesSebastiano Della CasaNo ratings yet
- Fistula First BookletDocument10 pagesFistula First Bookletcharlenetan18100% (2)
- Aneurysmal Subarachnoid Hemorrhage.6Document19 pagesAneurysmal Subarachnoid Hemorrhage.6Aldy Setiawan PutraNo ratings yet
- Pi Is 0894731723005333Document62 pagesPi Is 0894731723005333ВалентинаNo ratings yet
- 1 s2.0 S2213333X20303498 MainDocument9 pages1 s2.0 S2213333X20303498 MainOncología CdsNo ratings yet
- Anesthesia-Related Cardiac Arrest: Background: MethodsDocument10 pagesAnesthesia-Related Cardiac Arrest: Background: MethodsIlona HiariejNo ratings yet
- 1 s2.0 S1052305717301088 MainDocument7 pages1 s2.0 S1052305717301088 MainAnonymous Tu0bG0BGNo ratings yet
- Cardio VacDocument6 pagesCardio VacstarzecNo ratings yet
- Intervesnsi Stroke 1Document9 pagesIntervesnsi Stroke 1Zilbran BerontaxNo ratings yet
- Intracranial Hemorrhage - Background, Pathophysiology, EpidemiologyDocument5 pagesIntracranial Hemorrhage - Background, Pathophysiology, EpidemiologyejtNo ratings yet
- Indonesian Journal of Global Health ResearchDocument10 pagesIndonesian Journal of Global Health ResearchcandraNo ratings yet
- 8 Donor Vigilance A Global UpdateDocument7 pages8 Donor Vigilance A Global UpdateLyonTrioréNo ratings yet
- International J of Stroke - 2010 - Amin Hanjani - Vertebrobasilar Flow Evaluation and Risk of Transient Ischaemic AttackDocument7 pagesInternational J of Stroke - 2010 - Amin Hanjani - Vertebrobasilar Flow Evaluation and Risk of Transient Ischaemic AttackJose Manuel Fuentes Del PozoNo ratings yet
- Complications of The Arteriovenous Fistula: A Systematic ReviewDocument45 pagesComplications of The Arteriovenous Fistula: A Systematic ReviewAnonymous ATdLPZNo ratings yet
- Complication of Av Shunt PDFDocument12 pagesComplication of Av Shunt PDFsitifathiyaNo ratings yet
- TEE Surgical Decision Making - June2020 PDFDocument43 pagesTEE Surgical Decision Making - June2020 PDFalina100% (1)
- Diagnosis and Management of Cerebral Venous Thrombosis A Scientific Statement From The American Heart AssociationDocument14 pagesDiagnosis and Management of Cerebral Venous Thrombosis A Scientific Statement From The American Heart AssociationAdmin neuro-usu.idNo ratings yet
- 2017 HSA Clinical PracticeDocument10 pages2017 HSA Clinical PracticeAndrea MartinezNo ratings yet
- Cerebral Venous ThrombosisDocument14 pagesCerebral Venous ThrombosisSrinivas PingaliNo ratings yet
- Ultrasound-Guided Subclavian Vein Catheterization. A Systematic Review and Meta-Analysis. Crit Care Med 2015Document10 pagesUltrasound-Guided Subclavian Vein Catheterization. A Systematic Review and Meta-Analysis. Crit Care Med 2015angelama1783riosNo ratings yet
- NoorlifeDocument24 pagesNoorlifeIqra AsimNo ratings yet
- Cardiac Catheter Draft 2017 Evidence TableDocument9 pagesCardiac Catheter Draft 2017 Evidence TableCarla Isabel De CastroNo ratings yet
- Haemodialysis and The Risk of Stroke: A Population-Based Cohort Study in Taiwan, A Country of High Incidence of End-Stage Renal DiseaseDocument6 pagesHaemodialysis and The Risk of Stroke: A Population-Based Cohort Study in Taiwan, A Country of High Incidence of End-Stage Renal DiseaseJeffry HaryantoNo ratings yet
- 05 N017 13566Document14 pages05 N017 13566sr.kumariNo ratings yet
- Rosero2016 Nationwide Incidence of Serious Complications of Epidural AnalgesiaDocument11 pagesRosero2016 Nationwide Incidence of Serious Complications of Epidural Analgesiacailin.hicuraNo ratings yet
- Specialised Vascular Services Service Specification AdultsDocument25 pagesSpecialised Vascular Services Service Specification AdultsDr-Iyad AljuaidiNo ratings yet
- Jorgensen 2019Document8 pagesJorgensen 2019Emeray EssenceNo ratings yet
- Management of Acute Limb Ischemia in The Pediatric PopulationDocument5 pagesManagement of Acute Limb Ischemia in The Pediatric PopulationPendidikan Dokter Unsyiah 2015No ratings yet
- Ts Jurnal Batak SarapDocument6 pagesTs Jurnal Batak SarapAdityaNo ratings yet
- Pi Is 1600613522261644Document3 pagesPi Is 1600613522261644Serque777No ratings yet
- Hagedorn 2019Document10 pagesHagedorn 2019Cinthya Añazco RomeroNo ratings yet
- Caroticocavernous Fistula - Radiology Reference Article - RadiopaediaDocument8 pagesCaroticocavernous Fistula - Radiology Reference Article - RadiopaediaKhushi TahilianiNo ratings yet
- Insuficienta Venoasa CronicaDocument15 pagesInsuficienta Venoasa CronicaSimona IonitaNo ratings yet
- Dextrocardia PaperDocument18 pagesDextrocardia PaperChrismicel GunarsoNo ratings yet
- Subarachnoid HemorrhageDocument10 pagesSubarachnoid HemorrhageRoberto López Mata100% (1)
- Arteriovenous Access For HemodialysisDocument11 pagesArteriovenous Access For Hemodialysislakshminivas PingaliNo ratings yet
- RD 137348Document51 pagesRD 137348Hendris CitraNo ratings yet
- Management of Epistaxis in Patients With Ventricular Assist Device: A Retrospective ReviewDocument6 pagesManagement of Epistaxis in Patients With Ventricular Assist Device: A Retrospective ReviewDenta HaritsaNo ratings yet
- 1 s2.0 S0741521416318535 MainDocument11 pages1 s2.0 S0741521416318535 MainRohib MalikNo ratings yet
- Policy Statement2010Document23 pagesPolicy Statement2010unyilNo ratings yet
- Epistaksis Dan TatalaksanaDocument4 pagesEpistaksis Dan TatalaksanametaferosiaNo ratings yet
- Fisiopato IsquemiaDocument12 pagesFisiopato IsquemiaMaría Luisa MantillaNo ratings yet
- Lentine Et Al 2012 Cardiac Disease Evaluation and Management Among Kidney and Liver Transplantation CandidatesDocument47 pagesLentine Et Al 2012 Cardiac Disease Evaluation and Management Among Kidney and Liver Transplantation CandidatesFabiola TiempoNo ratings yet
- Guias ASRA 2010 Anestesia Regional en Paciente AnticoaguladoDocument38 pagesGuias ASRA 2010 Anestesia Regional en Paciente AnticoaguladoJonathan Tipon Galvis100% (1)
- 2013 - BoghaniDocument11 pages2013 - Boghanialejandra gonzalezNo ratings yet
- Comparative Analysis of Radiocephalic Versus Brach PDFDocument7 pagesComparative Analysis of Radiocephalic Versus Brach PDFandikeNo ratings yet
- Review Articles: A Systematic Review On Internal Jugular Vein Thrombosis and Pulmonary EmbolismDocument5 pagesReview Articles: A Systematic Review On Internal Jugular Vein Thrombosis and Pulmonary EmbolismdevaNo ratings yet
- Ijhs 14488+4945 4957Document13 pagesIjhs 14488+4945 4957simeamaservameNo ratings yet
- Romagna Et Al-2012-Journal of Clinical Periodontology PDFDocument7 pagesRomagna Et Al-2012-Journal of Clinical Periodontology PDFChristine HacheNo ratings yet
- TDR1Document7 pagesTDR1Santanico De CVT deozaNo ratings yet
- Cerebral AneurysmsDocument12 pagesCerebral AneurysmsDyah Ayu Puspita AnggarsariNo ratings yet
- A-Line Complication PDFDocument8 pagesA-Line Complication PDFaeagesNo ratings yet
- Veins and HypertensionDocument9 pagesVeins and Hypertensionlavanya.aNo ratings yet
- Warrier 2008Document3 pagesWarrier 2008darkmatter1No ratings yet
- Racial Disparity in CVSDocument21 pagesRacial Disparity in CVSAndi MulyadiNo ratings yet
- Anesthesia-Related Cardiac Arrest: Background: MethodsDocument10 pagesAnesthesia-Related Cardiac Arrest: Background: MethodsUtari Mudhia Arisa PutriNo ratings yet
- Practice Guidelines For Perioperative Blood TransfusionDocument11 pagesPractice Guidelines For Perioperative Blood TransfusionDevie MaraNo ratings yet
- Vascular MalformationsFrom EverandVascular MalformationsAjay K. KhannaNo ratings yet
- Evidence-Based Podiatry: A Clinical Guide to Diagnosis and ManagementFrom EverandEvidence-Based Podiatry: A Clinical Guide to Diagnosis and ManagementDyane E. TowerNo ratings yet
- Research Paper (ENGL-253) 6Document17 pagesResearch Paper (ENGL-253) 6Slime DuckNo ratings yet
- Medical RecordDocument8 pagesMedical RecordKusumadewi WidiarsaNo ratings yet
- Hazard Psychosocial in Construction IndustryDocument9 pagesHazard Psychosocial in Construction IndustryYekti Arum NNo ratings yet
- Leitzmann - Vegetarian Diets - What Are The AdvantagesDocument11 pagesLeitzmann - Vegetarian Diets - What Are The Advantageswbechara103No ratings yet
- Screening Test For HCVDocument11 pagesScreening Test For HCVMohamed KhalidNo ratings yet
- History ObgynDocument37 pagesHistory ObgynRana WaelNo ratings yet
- The Incompetent Cervix 2Document30 pagesThe Incompetent Cervix 2api-3705046100% (3)
- Essential Intrapartum and Newborn CareDocument27 pagesEssential Intrapartum and Newborn CareKaren Mae AlcantaraNo ratings yet
- UK Requirements Checklist and Study MaterialsDocument2 pagesUK Requirements Checklist and Study MaterialsKrizle Adaza100% (1)
- High-Performance Recovery ScreenDocument1 pageHigh-Performance Recovery Screenjason morrisNo ratings yet
- 14. ĐỀ VIP 14 - Soạn chuẩn cấu trúc minh họa BGD năm 2023 - Môn TIẾNG ANH - Bản word có giải (TN6) .Image.MarkedDocument10 pages14. ĐỀ VIP 14 - Soạn chuẩn cấu trúc minh họa BGD năm 2023 - Môn TIẾNG ANH - Bản word có giải (TN6) .Image.Marked1807070085No ratings yet
- Uterine Prolapse: Prepared by Dipti PunjalDocument35 pagesUterine Prolapse: Prepared by Dipti PunjalDipti0% (1)
- Narration of Questionnaire AnneDocument2 pagesNarration of Questionnaire AnnekisNo ratings yet
- Sas 5Document2 pagesSas 5Hannahleth GorzonNo ratings yet
- Abortion: Realities & Responsibilities: Michael L. TanDocument21 pagesAbortion: Realities & Responsibilities: Michael L. TanJaironShaltzMaralitQuizonNo ratings yet
- STELLA Modeling of A Zombie InvasionDocument6 pagesSTELLA Modeling of A Zombie Invasionjarettd100% (1)
- GordonDocument4 pagesGordonFrancheska MicuNo ratings yet
- Nurse Patient Interaction FormDocument3 pagesNurse Patient Interaction FormNim FernandoNo ratings yet
- WHS01Document2 pagesWHS01Mohd ObaidullahNo ratings yet
- Nonsuch Hospital List Providers Updated Hospital ListDocument12 pagesNonsuch Hospital List Providers Updated Hospital ListagbaipissNo ratings yet
- Acute PainDocument1 pageAcute PainJohn Herrera TanchuanNo ratings yet
- Medical Billing and Coding SpecialistDocument2 pagesMedical Billing and Coding Specialistapi-77786926100% (3)
- SW Provider Directory 2018 1ST QTR - CompressedDocument20 pagesSW Provider Directory 2018 1ST QTR - CompressedStayWell InsuranceNo ratings yet
- CML JK 2016 - Dr. Johan KurniandaDocument32 pagesCML JK 2016 - Dr. Johan KurniandaFerry FaisalNo ratings yet
- l6 Diploma Unit 1 Specimen Paper v2 002Document4 pagesl6 Diploma Unit 1 Specimen Paper v2 002NadeeraKarimNo ratings yet
- Guide To Detox: Being Healthy Is A Revolutionary ActDocument20 pagesGuide To Detox: Being Healthy Is A Revolutionary Acta3llamNo ratings yet
- VIKKI13Document6 pagesVIKKI13Dillisrinivasarao NNo ratings yet
- ActSheet ResearchDocument23 pagesActSheet ResearchRoy Benedicto Jr.No ratings yet
- Good Thesis Statement For Down SyndromeDocument5 pagesGood Thesis Statement For Down Syndromejamiemillerpeoria100% (2)