Download as pdf or txt
You might also like
- Pass Ultrasound Physics Exam Study Guide ReviewFrom EverandPass Ultrasound Physics Exam Study Guide ReviewRating: 4.5 out of 5 stars4.5/5 (2)
- Charlotte Fiell, Peter Fiell The Story of Design From The Paleolithic To The Present (2016)Document516 pagesCharlotte Fiell, Peter Fiell The Story of Design From The Paleolithic To The Present (2016)Eylül Gökbudak100% (2)
- Maximillien de Lafayette PDFDocument43 pagesMaximillien de Lafayette PDFAmeli Apuy80% (10)
- Reviewer For NCMB312 Skills Lab FINALSDocument12 pagesReviewer For NCMB312 Skills Lab FINALSchrisver008No ratings yet
- Pulse Oximetry Update in AnaesthesiaDocument4 pagesPulse Oximetry Update in AnaesthesiaConstantineSemenchukNo ratings yet
- (Auditory Brainstem Response) : Presented By: HemaniDocument42 pages(Auditory Brainstem Response) : Presented By: HemaniHemaniNo ratings yet
- Pulseless Ventricular Tachycardia/Ventricular Fibrillation Algorithm (Figure 8-5)Document1 pagePulseless Ventricular Tachycardia/Ventricular Fibrillation Algorithm (Figure 8-5)Dyan IslamiNo ratings yet
- N1614836189AnesthesiaDocument10 pagesN1614836189AnesthesiaVivek MathewsNo ratings yet
- Eathing IDI 2015Document58 pagesEathing IDI 2015Syamsul Bahri AkhasNo ratings yet
- Monitoring Intra Operatif: Mindi Widayani NRP 122.022.1115 FK UPN "Veteran" JakartaDocument21 pagesMonitoring Intra Operatif: Mindi Widayani NRP 122.022.1115 FK UPN "Veteran" Jakartaputri wulandariNo ratings yet
- Smith Spiro RevisitedDocument76 pagesSmith Spiro Revisitedsstefan888No ratings yet
- ABR ShortDocument50 pagesABR ShortLau Teik BengNo ratings yet
- Anesthesia EquipmentDocument21 pagesAnesthesia EquipmentAna KhNo ratings yet
- PSGDocument57 pagesPSGsg1964No ratings yet
- Reflex Measurements: Quick GuideDocument10 pagesReflex Measurements: Quick GuidefilippobNo ratings yet
- Mechanical Ventilator: Parameters of Mechanical VentilationDocument7 pagesMechanical Ventilator: Parameters of Mechanical Ventilationpraveen joseNo ratings yet
- Role of Pacing With High Frequency Shock in Reversion of Acute Episodes of Atrial Fibrillation and Atypical Atrial FlutterDocument23 pagesRole of Pacing With High Frequency Shock in Reversion of Acute Episodes of Atrial Fibrillation and Atypical Atrial FlutterdcicareNo ratings yet
- Auditory Brainstem ResponseDocument18 pagesAuditory Brainstem ResponseFree dataNo ratings yet
- Ecg in Emergency: Adi SulistyantoDocument41 pagesEcg in Emergency: Adi Sulistyantomech_pilot2203No ratings yet
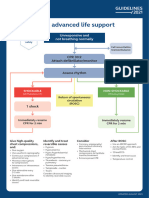
- Adult Advanced Life Support Algorithm 2021 Aug 2023Document1 pageAdult Advanced Life Support Algorithm 2021 Aug 2023cknihilnewNo ratings yet
- Electrical and Electronic CommunicationDocument5 pagesElectrical and Electronic CommunicationGillyn SiaronNo ratings yet
- Cardiopulmonary Resuscitation (CPR) : Gözde İnan, MD Kutluk Pampal, MDDocument60 pagesCardiopulmonary Resuscitation (CPR) : Gözde İnan, MD Kutluk Pampal, MDSarper Hikmet TAZENo ratings yet
- Pulse Oxymetry.1654268763516Document46 pagesPulse Oxymetry.1654268763516ConstantineSemenchukNo ratings yet
- Algorithms of AHA 2020Document23 pagesAlgorithms of AHA 2020Emirhan llkhanNo ratings yet
- (Electroencephalogram) An Introduction: By: Muhammad Farooq Supervisors: Dr. Aamir Saeed Malik Dr. Mohd Zuki Bin YousaffDocument31 pages(Electroencephalogram) An Introduction: By: Muhammad Farooq Supervisors: Dr. Aamir Saeed Malik Dr. Mohd Zuki Bin YousafffarooqespnNo ratings yet
- Interpretation On Pulmonary Function TestDocument105 pagesInterpretation On Pulmonary Function Testsalmamaged7619No ratings yet
- Ratnawati - Spirometry For Diagnosis OLDDocument61 pagesRatnawati - Spirometry For Diagnosis OLDAndry Wahyudi AgusNo ratings yet
- Immediate Life SupportDocument63 pagesImmediate Life Supportmatrixkhalifa9955No ratings yet
- Automated Detection of Obstructive Sleep Apnoea by Single-Lead ECG Through ELM ClassificationDocument4 pagesAutomated Detection of Obstructive Sleep Apnoea by Single-Lead ECG Through ELM ClassificationbengheniaNo ratings yet
- TBR AclsDocument9 pagesTBR Aclsric_vir_014No ratings yet
- Drug Study PediaDocument18 pagesDrug Study PediaCyx17No ratings yet
- Assessment Nursing Diagnosis Background Knowledge Planning Intervention Rationale Evaluation Subjective: Short Term: Independent: IndependentDocument4 pagesAssessment Nursing Diagnosis Background Knowledge Planning Intervention Rationale Evaluation Subjective: Short Term: Independent: IndependentAlyssa Marie SantosNo ratings yet
- ACLS Book (New)Document23 pagesACLS Book (New)Essa AyazNo ratings yet
- Body CT - Chest HRCTDocument5 pagesBody CT - Chest HRCTKelum BuddhikaNo ratings yet
- Seckel ARDSComplicatedICUPatientsDocument64 pagesSeckel ARDSComplicatedICUPatientsxcopy.bhNo ratings yet
- 2017 CCRespiratory Monitoring and Management (1) (002) .PPTX 10-4-NOTEFORMATDocument33 pages2017 CCRespiratory Monitoring and Management (1) (002) .PPTX 10-4-NOTEFORMATmichelleNo ratings yet
- Case Presentation On Supraventricular TachycardiaDocument64 pagesCase Presentation On Supraventricular TachycardiaHazel AsperaNo ratings yet
- The AASM Manual For The Scoring of Sleep and Associated EventsDocument34 pagesThe AASM Manual For The Scoring of Sleep and Associated Eventssenseilu8713No ratings yet
- Hatice Özkardesler, 66 Years, Female. Comes To Your Clinic Due To Husband Cannot Sleep !Document68 pagesHatice Özkardesler, 66 Years, Female. Comes To Your Clinic Due To Husband Cannot Sleep !عبدالعزيز رحمانيNo ratings yet
- Assr, Vemp, VNG, OaeDocument8 pagesAssr, Vemp, VNG, OaeSuprit Sn100% (1)
- Agilent UV-Vis Compliance With USPDocument6 pagesAgilent UV-Vis Compliance With USPwahNo ratings yet
- Adult Respiratory Distress Syndrome: Mazen Kherallah, MD, FCCPDocument51 pagesAdult Respiratory Distress Syndrome: Mazen Kherallah, MD, FCCPArsitoNo ratings yet
- Eeg Circuit Design: NSF ProjectDocument136 pagesEeg Circuit Design: NSF ProjectJesus Peña100% (2)
- Monitoring / Tiva / AwarenessDocument51 pagesMonitoring / Tiva / AwarenessDurgesh PadoleNo ratings yet
- ACLS ReportDocument58 pagesACLS ReportCamille Honeyleith FernandoNo ratings yet
- Sistem Saraf Pusat (Central Nervous System)Document23 pagesSistem Saraf Pusat (Central Nervous System)Ruspata BhyantariNo ratings yet
- Assessment of HearingDocument51 pagesAssessment of HearingSwetha PasupuletiNo ratings yet
- EegDocument33 pagesEegaryan.choudhary011101No ratings yet
- Eeg Circuit Design: NSF ProjectDocument136 pagesEeg Circuit Design: NSF Projectrhycardo5902No ratings yet
- Extubation Criteria & Delayed EmergenceDocument3 pagesExtubation Criteria & Delayed EmergenceMohonaNo ratings yet
- (E) 2016 VERBRAECKEN Diagnostic Techniques TEXTDocument4 pages(E) 2016 VERBRAECKEN Diagnostic Techniques TEXTJPNo ratings yet
- Auditory Brainstem Evoked Response (Abr)Document37 pagesAuditory Brainstem Evoked Response (Abr)Nitin Sharma100% (2)
- Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanDocument64 pagesDepartemen Kardiologi FK USU RSUP. H. Adam Malik MedanBonitavanyNo ratings yet
- Performance of Electroencephalogram Derived ParameDocument8 pagesPerformance of Electroencephalogram Derived ParameRENAULTNo ratings yet
- Pulmonary Function TestsDocument35 pagesPulmonary Function Testsnirilib100% (4)
- Tuning Fork TestDocument56 pagesTuning Fork TestAbdur RaqibNo ratings yet
- ECE3041 - Biomedical Instrumentation and Measurements TASK-2Document3 pagesECE3041 - Biomedical Instrumentation and Measurements TASK-2Manasi NaradeNo ratings yet
- Auditory Brainstem Response - ABR - in Clinical Practice PDFDocument9 pagesAuditory Brainstem Response - ABR - in Clinical Practice PDFary wisma dewiNo ratings yet
- Diagnostic AudiologyDocument8 pagesDiagnostic AudiologyAyushman KhatriNo ratings yet
- Intraoperative Neurophysiological Monitoring in Hemifacial Spasm: A Practical GuideFrom EverandIntraoperative Neurophysiological Monitoring in Hemifacial Spasm: A Practical GuideNo ratings yet
- Or) Y E: Far RN Sra NN Ny:00 0)Document10 pagesOr) Y E: Far RN Sra NN Ny:00 0)goguito rrvaNo ratings yet
- X Complex K Complex K Complea: AASM Scoring Manual Version 2.5 31Document10 pagesX Complex K Complex K Complea: AASM Scoring Manual Version 2.5 31goguito rrvaNo ratings yet
- The AASM Manual: For The Scoring of SleepDocument10 pagesThe AASM Manual: For The Scoring of Sleepgoguito rrvaNo ratings yet
- 01-10 OcrDocument10 pages01-10 Ocrgoguito rrvaNo ratings yet
- Road Safety Banner 2018Document18 pagesRoad Safety Banner 2018Safety ManagerNo ratings yet
- 2nd Dispatch DLPD - IIT JEE - Class XI - English - PC (Physics) PDFDocument162 pages2nd Dispatch DLPD - IIT JEE - Class XI - English - PC (Physics) PDFRaja Bisht50% (8)
- 1 Apogee General PDFDocument12 pages1 Apogee General PDFJoanNo ratings yet
- Class 3 4 KeyDocument12 pagesClass 3 4 Keyshivamsingh.fscNo ratings yet
- Unit-4 Disaster Management NotesDocument33 pagesUnit-4 Disaster Management Notesholalo6378No ratings yet
- Production Unit - 4Document24 pagesProduction Unit - 4Goutham AppuNo ratings yet
- Click The Blue Buttons Below To Navigate Part 1 More EfficientlyDocument89 pagesClick The Blue Buttons Below To Navigate Part 1 More Efficientlyelite writerNo ratings yet
- Chapter-1 FinalDocument8 pagesChapter-1 FinalHazel NutNo ratings yet
- Entr CH 1Document7 pagesEntr CH 184kaveri8650% (2)
- Development of "Mang Kepweng's Lab": A Mobile Android Information On Herbal PlantsDocument160 pagesDevelopment of "Mang Kepweng's Lab": A Mobile Android Information On Herbal PlantsMac John Teves Poblete100% (3)
- Circular Motion IB N07 A2Document2 pagesCircular Motion IB N07 A2superpooh-1No ratings yet
- Zupcasti Par B-F B 35Document4 pagesZupcasti Par B-F B 35Stefan MilojevicNo ratings yet
- Ishan Parmar - Performance MarketingDocument2 pagesIshan Parmar - Performance MarketingVaibhav RaghuvanshiNo ratings yet
- CORDILLERADocument27 pagesCORDILLERAmaria kyla andradeNo ratings yet
- Investigate The Impact of Social Media On Students: Cardiff Metropolitan UniversityDocument57 pagesInvestigate The Impact of Social Media On Students: Cardiff Metropolitan UniversityKarlo JayNo ratings yet
- Revision Notes On Alternating Current For NEET 2023 - Free PDF DownloadDocument20 pagesRevision Notes On Alternating Current For NEET 2023 - Free PDF Downloadbiswaranjannayak259No ratings yet
- S 0009840 X 07001941 ADocument3 pagesS 0009840 X 07001941 Aaristarchos76No ratings yet
- Quarter 3 - Module 1-W3: Computer Systems Servicing (CSS)Document3 pagesQuarter 3 - Module 1-W3: Computer Systems Servicing (CSS)AC BalioNo ratings yet
- AI523 Data Sheet, 2, en USDocument12 pagesAI523 Data Sheet, 2, en USJozz LivelyNo ratings yet
- BPSCL Industrial TrainingDocument28 pagesBPSCL Industrial TrainingAbhigyan PrakashNo ratings yet
- Listeria Monocytogenes and Other Listeria Species PDFDocument27 pagesListeria Monocytogenes and Other Listeria Species PDFkurniawan0031No ratings yet
- JSA Wet End or Dryer Bearing Inspection Paper MillDocument6 pagesJSA Wet End or Dryer Bearing Inspection Paper MillMlayeh MohamedNo ratings yet
- ImmigrationDocument4 pagesImmigrationJen AnnNo ratings yet
- MPCA Response 5.29.20Document2 pagesMPCA Response 5.29.20Duluth News TribuneNo ratings yet
- Eneos Sustina Product Data Sheet 2016Document2 pagesEneos Sustina Product Data Sheet 2016dan0410No ratings yet
- Kono Subarashii Sekai Ni Shukufuku Wo! Volume 2 PDFDocument198 pagesKono Subarashii Sekai Ni Shukufuku Wo! Volume 2 PDFRokhi NNo ratings yet
- Modelling Nutrient Utilization in Farm AnimalsDocument432 pagesModelling Nutrient Utilization in Farm AnimalsHéctor W Moreno QNo ratings yet
- Buku SDKIDocument246 pagesBuku SDKIAdi Pramono100% (1)