Download as pdf or txt
You might also like
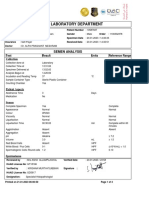
- Semen AnalysisDocument2 pagesSemen AnalysisThenunda തേനുണ്ടNo ratings yet
- DR Lal Pathlabs: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini Delhi 110085Document4 pagesDR Lal Pathlabs: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini Delhi 110085Shubham BhadouriyaNo ratings yet
- Clinical Cases and OSCEs in Surgery 2EDocument274 pagesClinical Cases and OSCEs in Surgery 2EHO YU CHANNo ratings yet
- 2013 Urology CatalogDocument233 pages2013 Urology CatalogAna LauraNo ratings yet
- Ige PDFDocument1 pageIge PDFAnonymous zXF5UgqP8No ratings yet
- Differential Diagnosis of JaundiceDocument4 pagesDifferential Diagnosis of JaundiceVirag PatilNo ratings yet
- PI e BIL - TOTAL 16Document2 pagesPI e BIL - TOTAL 16ilhamNo ratings yet
- Immediate Newborn Care (Autosaved)Document183 pagesImmediate Newborn Care (Autosaved)mftaganas100% (1)
- CBC Arikod HoimaDocument37 pagesCBC Arikod Hoimadaniel arikodNo ratings yet
- Endoscopic, Retrograde Cholangio Pancreatography ERCPDocument17 pagesEndoscopic, Retrograde Cholangio Pancreatography ERCPHamzeh AlmasriNo ratings yet
- Final Thesis Doc - 2020Document111 pagesFinal Thesis Doc - 2020Umar QuraishiNo ratings yet
- Ljl0wdga4zgftfjlachhji4oDocument3 pagesLjl0wdga4zgftfjlachhji4oAmitNo ratings yet
- Actionshowpdfpii S0272 638628232900006 9Document10 pagesActionshowpdfpii S0272 638628232900006 9Miguel Ángel DomínguezNo ratings yet
- Clsi H15 A3Document51 pagesClsi H15 A3Cristian Gutiérrez VeraNo ratings yet
- Lab - Report - BHAVISHKA JIDocument4 pagesLab - Report - BHAVISHKA JIYogeshKumarLoharNo ratings yet
- Empagliflozin and Linagliptin 2020 Sept FinalDocument65 pagesEmpagliflozin and Linagliptin 2020 Sept FinalJenny Calapati TorrijosNo ratings yet
- 1 Role of Ultrasound in The Evaluation of Acute Pelvic PainDocument11 pages1 Role of Ultrasound in The Evaluation of Acute Pelvic PainGhofran Ibrahim HassanNo ratings yet
- Anti-HCV Reagent Kit: B8P060 G71272R05Document8 pagesAnti-HCV Reagent Kit: B8P060 G71272R05LoloNo ratings yet
- 1 Hemoglobinopathies BookDocument26 pages1 Hemoglobinopathies BookRhoda Lom-ocNo ratings yet
- NMC Hospital Abu Dhabi - 2011!06!08Document16 pagesNMC Hospital Abu Dhabi - 2011!06!08Manjul TakleNo ratings yet
- Pgs Guidance Exam Book PDFDocument369 pagesPgs Guidance Exam Book PDFUsman IlyasNo ratings yet
- Clinical Laboratory Tests - Which, Why, and What Do The Results Mean? - LaboratorDocument34 pagesClinical Laboratory Tests - Which, Why, and What Do The Results Mean? - LaboratorGeorgeNo ratings yet
- Hepatology MRCP1Document87 pagesHepatology MRCP1Raouf Ra'fat SolimanNo ratings yet
- Niosomes PDFDocument165 pagesNiosomes PDFDr. Anil LandgeNo ratings yet
- JWALADocument2 pagesJWALAVaid Navdeep Singh100% (1)
- Blood CollectionDocument47 pagesBlood CollectionNawab din BakhashNo ratings yet
- Hema2 Lec Lab 1Document48 pagesHema2 Lec Lab 1Yo Issei HyodonoNo ratings yet
- Streptococcal PharyngitisDocument28 pagesStreptococcal PharyngitissylviaNo ratings yet
- Clinical Radiology Handbook v1.0Document162 pagesClinical Radiology Handbook v1.0Zulqarnain AbidNo ratings yet
- NormaltestreportDocument1 pageNormaltestreportTayyeb KhanNo ratings yet
- Sedimen UrinDocument73 pagesSedimen UrinHerbanu PramonoNo ratings yet
- Newborn Screening Panel of Disorders: Management ProtocolDocument56 pagesNewborn Screening Panel of Disorders: Management ProtocolRay Arvin DyNo ratings yet
- Shaukat Khanum Memorial Cancer Hospital & Research CentreDocument2 pagesShaukat Khanum Memorial Cancer Hospital & Research CentreUsama AjmalNo ratings yet
- Patient Feedback FormDocument2 pagesPatient Feedback FormKAVI SUSINo ratings yet
- The Urinary The Urinary SedimentDocument116 pagesThe Urinary The Urinary SedimentMahda WasilaNo ratings yet
- 9789386478122Document15 pages9789386478122ruacondungmanhNo ratings yet
- Clsi Auto5 ADocument61 pagesClsi Auto5 ACristian Gutiérrez VeraNo ratings yet
- Clsi GP23 ADocument45 pagesClsi GP23 ACristian Gutiérrez VeraNo ratings yet
- Procedures For The Collection of Diagnostic Blood Specimens by Venipuncture Approved Standard-Sixth EditionDocument56 pagesProcedures For The Collection of Diagnostic Blood Specimens by Venipuncture Approved Standard-Sixth EditionCYNTHIANo ratings yet
- Kidney DoctorsDocument11 pagesKidney DoctorsmamunmnNo ratings yet
- CMC Handbook For Management of COVID19Document91 pagesCMC Handbook For Management of COVID19Tata Lokesh Kumar100% (1)
- Nuclear Medicine Training AccredditationDocument15 pagesNuclear Medicine Training Accredditationpriya selvarajNo ratings yet
- MABB Presentation 5 24 2022Document39 pagesMABB Presentation 5 24 2022Ayman MehassebNo ratings yet
- CancerDocument23 pagesCancerpitkoliNo ratings yet
- Capsules DR Mohammed EidDocument246 pagesCapsules DR Mohammed EidMohammad BanisalmanNo ratings yet
- Nabl 600Document393 pagesNabl 600TRH RECRUITMENTNo ratings yet
- RamzanDocument2 pagesRamzanAli HassanNo ratings yet
- TestReport 209200137Document3 pagesTestReport 209200137Hitesh GolakiyaNo ratings yet
- Adobe Scan Nov 10, 2021Document2 pagesAdobe Scan Nov 10, 2021CESTER OPNo ratings yet
- FINAL A Project Report OnDocument24 pagesFINAL A Project Report OnramanNo ratings yet
- 001000000000088305Document2 pages001000000000088305FGEIs Ro WahNo ratings yet
- PGIMER Chandigarh Recruitment Oct 2022 Notification PDFDocument31 pagesPGIMER Chandigarh Recruitment Oct 2022 Notification PDFHemantNo ratings yet
- Urinalysis Presentation1Document25 pagesUrinalysis Presentation1OliviaLaneNo ratings yet
- Proper Maintenance of InstrumentsDocument92 pagesProper Maintenance of InstrumentsDimi DimoNo ratings yet
- 3-c TEa Tabel ExtinsDocument36 pages3-c TEa Tabel ExtinsJimboreanu György PaulaNo ratings yet
- Sub - PG Dissertation Title Registration With KNR UHS, WarangalDocument7 pagesSub - PG Dissertation Title Registration With KNR UHS, WarangalPradeep VunnamNo ratings yet
- AIIMS Current - Faculty - List PDFDocument17 pagesAIIMS Current - Faculty - List PDFA Man TANo ratings yet
- NAFLD WhitepaperDocument12 pagesNAFLD Whitepaperhalagur75No ratings yet
- 5 - Must To Know Clinical MicrosDocument44 pages5 - Must To Know Clinical MicrosRudolph Jr. TaubNo ratings yet
- DR Waseem Hammoudeh - Jordan and Hepatitis B Virus - Medics Index MemberDocument1 pageDR Waseem Hammoudeh - Jordan and Hepatitis B Virus - Medics Index MemberMedicsindex Telepin SlidecaseNo ratings yet
- Laboratorial Diagnostics Keypoints RevisionDocument6 pagesLaboratorial Diagnostics Keypoints RevisionFathimathNo ratings yet
- Leukemia Glossary of WordsDocument7 pagesLeukemia Glossary of WordsMuli MJNo ratings yet
- MCQs For LaboratoryDocument42 pagesMCQs For Laboratorynarendrakumar94100% (2)
- Complete Blood CountDocument18 pagesComplete Blood CountNazih MominNo ratings yet
- Regional Anatomy Question - MidtermDocument6 pagesRegional Anatomy Question - MidtermManju ShreeNo ratings yet
- Folk Theatre Andhra Yakshaganam Its TradDocument9 pagesFolk Theatre Andhra Yakshaganam Its TradManju Shree100% (1)
- Regional Anatomy Question - FinalDocument8 pagesRegional Anatomy Question - FinalManju ShreeNo ratings yet
- 2 - Regional Anatomy (MidTerm) MCQsDocument18 pages2 - Regional Anatomy (MidTerm) MCQsManju ShreeNo ratings yet
- Human Values and Culture Through LiteratDocument20 pagesHuman Values and Culture Through LiteratManju ShreeNo ratings yet
- The Tree Method - FinalDocument77 pagesThe Tree Method - FinalManju Shree100% (1)
- Anita Nair WorkbookDocument101 pagesAnita Nair WorkbookManju ShreeNo ratings yet
- UGTM-Top Manifestation MistakesDocument27 pagesUGTM-Top Manifestation MistakesManju Shree100% (2)
- Chartered Engineer Royal Aeronautical Society Ceng Chartered Engineer MraesDocument42 pagesChartered Engineer Royal Aeronautical Society Ceng Chartered Engineer MraesManju ShreeNo ratings yet
- Concept, Assessment, Goals, Objectives of High Risk NewbornDocument76 pagesConcept, Assessment, Goals, Objectives of High Risk NewbornEsha KuttiNo ratings yet
- Liver Function Test InterpretationDocument48 pagesLiver Function Test InterpretationKiattipoom Sukkulcharoen100% (1)
- Git & Hepatobiliary-I Module Study Guide - Mbbs Year-2, 2023Document16 pagesGit & Hepatobiliary-I Module Study Guide - Mbbs Year-2, 2023zeeshanmusic23No ratings yet
- AbdomenDocument10 pagesAbdomenironNo ratings yet
- Feses IntroductionDocument88 pagesFeses IntroductionAnisaPratiwiArumningsih100% (1)
- #19 GASMEN, Cyrille F. MED-1C Biochemical - Genetic Case 14Document2 pages#19 GASMEN, Cyrille F. MED-1C Biochemical - Genetic Case 14Cyrille GasmenNo ratings yet
- Biography of Hazrat Khwaja Khanoon SahibDocument13 pagesBiography of Hazrat Khwaja Khanoon SahibMohammed Abdul Hafeez, B.Com., Hyderabad, IndiaNo ratings yet
- Approach To The Child With AnemiaDocument9 pagesApproach To The Child With Anemiasack26_11_93No ratings yet
- 11-Immediate Care of NewbornDocument112 pages11-Immediate Care of NewbornJiela CarbonillaNo ratings yet
- 120 FreeDocument44 pages120 FreeAlon GoldfainerNo ratings yet
- Dog and Cat Health SecretsDocument70 pagesDog and Cat Health SecretsIvana Dasović100% (1)
- (PAEDS) PSS 3 - Neonatal JaundiceDocument41 pages(PAEDS) PSS 3 - Neonatal JaundiceRoshandiep GillNo ratings yet
- Clinical Chemistry at The Extremes of Age 2024Document24 pagesClinical Chemistry at The Extremes of Age 2024Thelmah S KenalemangNo ratings yet
- 54.the Gallbladder and Bile DuctsDocument19 pages54.the Gallbladder and Bile DuctsAdenegan Adesola RaymondNo ratings yet
- Pediatrics RemarksDocument62 pagesPediatrics RemarksGÖKSU SAYGILINo ratings yet
- Neonataljaundice 140128015601 Phpapp02Document39 pagesNeonataljaundice 140128015601 Phpapp02Tina TalmadgeNo ratings yet
- Emergency Pediatric AidsDocument29 pagesEmergency Pediatric AidsRana SalemNo ratings yet
- Kr2med 2006engDocument62 pagesKr2med 2006engHind YousifNo ratings yet
- Bilirubin Crystals in Neutrophils: A Rare Occurance: January 2018Document5 pagesBilirubin Crystals in Neutrophils: A Rare Occurance: January 2018Djdjjd SiisusNo ratings yet
- 7th March 2020 Plab 1 MockDocument32 pages7th March 2020 Plab 1 MockZoha QureshiNo ratings yet
- Lecture Notes: Clinical Chemistry of LiverDocument38 pagesLecture Notes: Clinical Chemistry of LivershehnilaNo ratings yet
- Management of Neonatal JaundiceDocument22 pagesManagement of Neonatal JaundiceSuhazeli Abdullah100% (1)
- Mtap 2 CC1 FinalsDocument9 pagesMtap 2 CC1 FinalsI love dem Coffee (Migz)No ratings yet
- BilirubinDocument40 pagesBilirubinAnisetiyowatiNo ratings yet
- Vasaguloochyadi Kashayam - YogamruthamDocument5 pagesVasaguloochyadi Kashayam - YogamruthamRahul KirkNo ratings yet
- Liver Function Reviewer Cc2Document7 pagesLiver Function Reviewer Cc2Leo NoquilNo ratings yet