Download as pdf or txt
You might also like
- BLS TimetableDocument1 pageBLS TimetablemariamNo ratings yet
- Approach 4 Standard Precautions Icon PDF 672KBDocument1 pageApproach 4 Standard Precautions Icon PDF 672KBElaine MacalandaNo ratings yet
- Case Study of The Change Management of British Airways After The Economic Crisis of 2008Document5 pagesCase Study of The Change Management of British Airways After The Economic Crisis of 2008Mirela-Elena Popa0% (1)
- Pre - de - Coding NabhDocument43 pagesPre - de - Coding NabhDr Ananta Kumari ChaurasiaNo ratings yet
- Paraformaldehyde MSDS: Section 1: Chemical Product and Company IdentificationDocument6 pagesParaformaldehyde MSDS: Section 1: Chemical Product and Company Identificationjuanme0489No ratings yet
- 11 01 Physical Restraint Time Out FormDocument3 pages11 01 Physical Restraint Time Out FormNewsTeam20100% (1)
- Daily Equipment Cleaning RecordsDocument3 pagesDaily Equipment Cleaning RecordsmathanbhuNo ratings yet
- (Mark With An X The Appropriate Box) : Dole-Bqf-WairDocument1 page(Mark With An X The Appropriate Box) : Dole-Bqf-Wairroland magoNo ratings yet
- Daily Work Schedule TemplateDocument2 pagesDaily Work Schedule Templatemichael collinsNo ratings yet
- Wair DoleDocument5 pagesWair Dolewizmaster computer sales & servicesNo ratings yet
- Assessment of Patient Safety ChallengesDocument9 pagesAssessment of Patient Safety Challengesmuhammad ismailNo ratings yet
- ERT MeetingDocument7 pagesERT MeetingMUNA100% (1)
- Occupational HealthDocument16 pagesOccupational HealthfaarehaNo ratings yet
- Hospital Safety IndexDocument5 pagesHospital Safety IndexEdward D. SarcoNo ratings yet
- (Facility Name) : Emergency Operations PlanDocument26 pages(Facility Name) : Emergency Operations PlanIbsen CampoverdeNo ratings yet
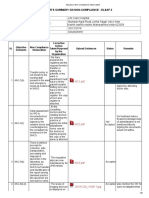
- Assessor Non Compliance ObservationDocument9 pagesAssessor Non Compliance ObservationSwati BajpaiNo ratings yet
- AEDRDocument1 pageAEDRPrestone100% (1)
- Annual Work Accident and Illness Exposure Data ReportDocument1 pageAnnual Work Accident and Illness Exposure Data ReportDarryl RoblesNo ratings yet
- Sop Occupational Safety and Health Complaints Mechanism UnitDocument12 pagesSop Occupational Safety and Health Complaints Mechanism UnitEmdad YusufNo ratings yet
- Solid Waste ChecklistDocument6 pagesSolid Waste ChecklistGIRBERT ADLAWONNo ratings yet
- Clinical Face Sheet: Category of PatientDocument14 pagesClinical Face Sheet: Category of PatientMarjorie UmipigNo ratings yet
- Annual Accident or Illness Exposure Data ReportDocument1 pageAnnual Accident or Illness Exposure Data ReportMi Primero MerchandiseNo ratings yet
- 3 Employer's Work Accident Illness ReportDocument2 pages3 Employer's Work Accident Illness ReportAlmario Sagun100% (2)
- Meeting With SKMDocument4 pagesMeeting With SKMAnwarNo ratings yet
- Safety ManualDocument17 pagesSafety ManualDr. Sachendra Raj100% (1)
- CHA Hospital Activation of The Emergency Operations Plan ChecklistDocument5 pagesCHA Hospital Activation of The Emergency Operations Plan Checklistraysub159No ratings yet
- Code Red Training Nayati Raju DagarDocument30 pagesCode Red Training Nayati Raju DagarRaju DagarNo ratings yet
- Incident Report Form: Personal DetailsDocument3 pagesIncident Report Form: Personal Detailsjhon suarezNo ratings yet
- Mega Mock DrillDocument22 pagesMega Mock DrillSharvari BurdeNo ratings yet
- 11.2 Baseline Medical Surveillance ProcedureDocument18 pages11.2 Baseline Medical Surveillance ProcedureaceNo ratings yet
- Commiittees Nabh 2015 SafetyDocument7 pagesCommiittees Nabh 2015 SafetypratimazNo ratings yet
- Job Description: Iii. Key Performance IndicatorsDocument2 pagesJob Description: Iii. Key Performance IndicatorsBidisha BasuNo ratings yet
- No Smoking Policy 2022Document5 pagesNo Smoking Policy 2022nlvmmc.laboratoryNo ratings yet
- Ape FormsDocument7 pagesApe FormsReynaldo Gacus YantoNo ratings yet
- HIV AIDS Workplace Policy & ProgramDocument4 pagesHIV AIDS Workplace Policy & ProgramJLA Construction ServicesNo ratings yet
- Accident Investigation ReportDocument2 pagesAccident Investigation ReportMichael MiotkNo ratings yet
- Employees Accedent ReportDocument1 pageEmployees Accedent ReportKomal TiwariNo ratings yet
- VCT ManualDocument70 pagesVCT ManualNay Lin HtikeNo ratings yet
- Assisted Delivery In: University of Iloilo Rizal Street, Iloilo City Tel No. (033) 338-1071 Loc. 146Document3 pagesAssisted Delivery In: University of Iloilo Rizal Street, Iloilo City Tel No. (033) 338-1071 Loc. 146Khyara Marie Estante DemiarNo ratings yet
- Safety Record Book PDFDocument11 pagesSafety Record Book PDFibrahimNo ratings yet
- HIRA ToolDocument26 pagesHIRA Toolsreekala2007No ratings yet
- 2.1. Organising For SafetyDocument29 pages2.1. Organising For SafetyPERATCHI SELVANNo ratings yet
- The Management and Control of Hospital Acquired InfectionDocument21 pagesThe Management and Control of Hospital Acquired InfectionHarrison TravisNo ratings yet
- 63 MdroDocument3 pages63 MdroerwindaNo ratings yet
- Fire Safety NABHDocument3 pagesFire Safety NABHTejinderNo ratings yet
- Crowd and Crisis Management Learning ActivitiesDocument6 pagesCrowd and Crisis Management Learning ActivitiesJamaica PicoNo ratings yet
- Purpose: Title: Code Pink-Abduction PlanDocument5 pagesPurpose: Title: Code Pink-Abduction Planarie susantoNo ratings yet
- HAND HYGIENE MONITORING SHEET (Revised)Document3 pagesHAND HYGIENE MONITORING SHEET (Revised)lance tabinasNo ratings yet
- Employee Medical Incident ReportDocument1 pageEmployee Medical Incident ReportAiswarya SukumarNo ratings yet
- State Hazcom TestDocument2 pagesState Hazcom TesteastNo ratings yet
- Time Taken For Initial AssessmentDocument1 pageTime Taken For Initial AssessmentNidhi VijanNo ratings yet
- Safety Observation ReportDocument3 pagesSafety Observation Reportraja ahmedNo ratings yet
- Identifying and Controlling Hazards: We Lco MeDocument45 pagesIdentifying and Controlling Hazards: We Lco MeAijaz Ahmed Shaikh100% (1)
- SOP For Preparation of Commonly Used Disinfectants and Fumigants Against Coronavirus (SARS-CoV-2)Document27 pagesSOP For Preparation of Commonly Used Disinfectants and Fumigants Against Coronavirus (SARS-CoV-2)andualemNo ratings yet
- Register of InjuriesDocument3 pagesRegister of InjuriesMani VannanNo ratings yet
- "No Smoking" Policy GuidelineDocument2 pages"No Smoking" Policy GuidelineMarti GregorioNo ratings yet
- Medicine Inventory 2010-2011Document2 pagesMedicine Inventory 2010-2011Michelle Domingo PalmaNo ratings yet
- Bosh Course OutlineDocument3 pagesBosh Course OutlineNinyasumergidoNo ratings yet
- 6 Hazard AvoidanceDocument22 pages6 Hazard AvoidancefirahliyanaNo ratings yet
- BOSH First Exam ReviewerDocument16 pagesBOSH First Exam ReviewerEDRICK PARASNo ratings yet
- DOLE - BQF - WAIR - COVID - 19excelver1 - 02 - REVISED (1) .XLSX - REVISED WAIR COVID 19Document1 pageDOLE - BQF - WAIR - COVID - 19excelver1 - 02 - REVISED (1) .XLSX - REVISED WAIR COVID 19Steve LopenaNo ratings yet
- Federation of Senior Citizens (New)Document3 pagesFederation of Senior Citizens (New)darwin18No ratings yet
- Coa SampleDocument2 pagesCoa Sampledarwin18No ratings yet
- Cengr 4140-Eq ReviewerDocument19 pagesCengr 4140-Eq Reviewerdarwin18No ratings yet
- AuthorizationDocument1 pageAuthorizationdarwin18No ratings yet
- Travis Oakes Fatality Inquiry ReportDocument10 pagesTravis Oakes Fatality Inquiry ReportcalcitydeskNo ratings yet
- 中文打字机一个世纪的汉字突围史 美墨磊宁Thomas S Mullaney Z-LibraryDocument490 pages中文打字机一个世纪的汉字突围史 美墨磊宁Thomas S Mullaney Z-Libraryxxx caoNo ratings yet
- FINA3010 Assignment1Document5 pagesFINA3010 Assignment1Hei RayNo ratings yet
- TED Taiye SelasiDocument4 pagesTED Taiye SelasiMinh ThuNo ratings yet
- STUDENT 2021-2022 Academic Calendar (FINAL)Document1 pageSTUDENT 2021-2022 Academic Calendar (FINAL)Babar ImtiazNo ratings yet
- Alex. Hamilton Vs Thomas JeffersonDocument4 pagesAlex. Hamilton Vs Thomas JeffersonRhett Hunt100% (1)
- Negara Hukum-5-1-Juni-2014Document99 pagesNegara Hukum-5-1-Juni-2014haekalnashvilleNo ratings yet
- 31-07-2020 - The Hindu Handwritten NotesDocument16 pages31-07-2020 - The Hindu Handwritten NotesnishuNo ratings yet
- Pre-Test - Pediatric NursingDocument6 pagesPre-Test - Pediatric NursingogiskuadzNo ratings yet
- GeffonDocument6 pagesGeffonDaniel HopsickerNo ratings yet
- 9-23-2020-Motion To Post Bail - Voltaire Gebulaguin - Atty. Blancia - Docx (Edited)Document7 pages9-23-2020-Motion To Post Bail - Voltaire Gebulaguin - Atty. Blancia - Docx (Edited)Andrei BlanciaNo ratings yet
- S R S M: Arah Owell and Cott AckenzieDocument7 pagesS R S M: Arah Owell and Cott AckenzieEduardo MBNo ratings yet
- M607 L01 SolutionDocument7 pagesM607 L01 SolutionRonak PatelNo ratings yet
- Nta (Ugc-Net) : Ask, Learn & LeadDocument18 pagesNta (Ugc-Net) : Ask, Learn & LeadprajwalbhatNo ratings yet
- Babu Jagjeevana Ram Uttarandhra Sujala SravanthiDocument5 pagesBabu Jagjeevana Ram Uttarandhra Sujala SravanthiYuvaraju CherukuriNo ratings yet
- Kenneth Alvis Pierce v. Ray H. Page, Warden, and The State of Oklahoma, 362 F.2d 534, 10th Cir. (1966)Document2 pagesKenneth Alvis Pierce v. Ray H. Page, Warden, and The State of Oklahoma, 362 F.2d 534, 10th Cir. (1966)Scribd Government DocsNo ratings yet
- CH 3Document41 pagesCH 3Diana BaRobNo ratings yet
- Ronquillo - Et Al. vs. Roco - Et Al.Document11 pagesRonquillo - Et Al. vs. Roco - Et Al.Court JorsNo ratings yet
- Economic Survey 2017-18Document350 pagesEconomic Survey 2017-18Subhransu Sekhar SwainNo ratings yet
- Gulf Times: HMC Providing State-Of-The-Art Treatment To All Covid-19 PatientsDocument20 pagesGulf Times: HMC Providing State-Of-The-Art Treatment To All Covid-19 PatientsmurphygtNo ratings yet
- Brown 2003Document12 pagesBrown 2003sziágyi zsófiaNo ratings yet
- Oisd STD 235Document110 pagesOisd STD 235naved ahmed100% (5)
- Fouts Def 2nd Production of DocumentsDocument88 pagesFouts Def 2nd Production of Documentswolf woodNo ratings yet
- Equatorial Realty Vs Mayfair TheaterDocument2 pagesEquatorial Realty Vs Mayfair TheaterSaji Jimeno100% (1)
- Chennai Dr. Ambedkar Government Law College, Pudupakkam Clinical Paper IV - Final Year List of StudentsDocument7 pagesChennai Dr. Ambedkar Government Law College, Pudupakkam Clinical Paper IV - Final Year List of StudentsSELMA G.SNo ratings yet
- Comparative Relationship Between Traditional Architecture and Modern ArchitectureDocument24 pagesComparative Relationship Between Traditional Architecture and Modern ArchitectureGem nuladaNo ratings yet
- Mayank Mehta EYDocument10 pagesMayank Mehta EYyasmeenfatimak52No ratings yet
- Teaching The SchwaDocument5 pagesTeaching The SchwaStarr BlueNo ratings yet
- PP 18 The Missa LectaDocument13 pagesPP 18 The Missa LectaRicardo TerrabuzziNo ratings yet