Download as docx, pdf, or txt
You might also like
- Break-Out Machines Level 1Document34 pagesBreak-Out Machines Level 1llereador100% (3)
- Laboratory Evaluation of Wood and Other Cellulosic Materials For Resistance To TermitesDocument3 pagesLaboratory Evaluation of Wood and Other Cellulosic Materials For Resistance To TermitesAnvit GadkarNo ratings yet
- How To Measure The PHPZC Using The PH Drift MethodDocument2 pagesHow To Measure The PHPZC Using The PH Drift Methodpaola aldana100% (1)
- Nola PenderDocument3 pagesNola PenderAlriam Twinkle MartinNo ratings yet
- Health Education RevDocument13 pagesHealth Education RevChelsea Taguiam GuillermoNo ratings yet
- Health Education Theories in Health Education: Sub Concepts of The Health Promotion ModelDocument6 pagesHealth Education Theories in Health Education: Sub Concepts of The Health Promotion ModelLexi LoreNo ratings yet
- Nola J. Pender's Health Promotion ModelDocument34 pagesNola J. Pender's Health Promotion Modeljay5ar5jamorabon5torNo ratings yet
- Nola PenderDocument9 pagesNola PenderAndrea YangNo ratings yet
- Pender ReportDocument16 pagesPender Reportfypbz6dncsNo ratings yet
- Ob CHAPTER 20Document5 pagesOb CHAPTER 20Magandia, Janizah R.No ratings yet
- Nola Pender (WEEK 8)Document11 pagesNola Pender (WEEK 8)Erica VelascoNo ratings yet
- Introduction To Health EducationDocument110 pagesIntroduction To Health EducationRaRe TV100% (1)
- Remodelling of Nola PenderDocument5 pagesRemodelling of Nola PenderDon Chiaw ManongdoNo ratings yet
- Nola PenderDocument4 pagesNola PenderMarian M.BaloNo ratings yet
- CHN 1 - Unfinished TransDocument3 pagesCHN 1 - Unfinished TransShiela PerdigonNo ratings yet
- Health Promotion ModelDocument5 pagesHealth Promotion Modelhanieyah29No ratings yet
- Peran & Perilaku KesehatanDocument49 pagesPeran & Perilaku Kesehatanhafid nugroho100% (1)
- Theories of Health PsychologyDocument38 pagesTheories of Health PsychologyTushar BansalNo ratings yet
- Module 4.5 - Nola PenderDocument2 pagesModule 4.5 - Nola Penderidk lolNo ratings yet
- 2lec wk2Document10 pages2lec wk2claire yowsNo ratings yet
- Reviewer 18 NOLA PENDERDocument2 pagesReviewer 18 NOLA PENDERClaireNo ratings yet
- Health Promotion ModelDocument22 pagesHealth Promotion ModelMonika shankarNo ratings yet
- TFN (Week 8)Document25 pagesTFN (Week 8)Erica VelascoNo ratings yet
- LgreenDocument3 pagesLgreenRadita MahendraNo ratings yet
- Phpe 210Document2 pagesPhpe 210Reg LagartejaNo ratings yet
- NCM Purposive TaskDocument3 pagesNCM Purposive TaskSandy ReyesNo ratings yet
- Edgar F. Borgatta, Rhonda J. V. Montgomery - Encyclopedia of Sociology - Volume 2-Macmillan Reference USA (2000) - 407-419Document13 pagesEdgar F. Borgatta, Rhonda J. V. Montgomery - Encyclopedia of Sociology - Volume 2-Macmillan Reference USA (2000) - 407-419Mohamed MassoudiNo ratings yet
- Health Promotion Model - Nola JDocument35 pagesHealth Promotion Model - Nola JmajoodhNo ratings yet
- Week 8 (Theories)Document8 pagesWeek 8 (Theories)Erica VelascoNo ratings yet
- Nola J. Pender's Health Promotion ModelDocument11 pagesNola J. Pender's Health Promotion ModelCINDY� BELMESNo ratings yet
- Nola Pender's Health Promotion Model - VICERA-NATIVIDADDocument27 pagesNola Pender's Health Promotion Model - VICERA-NATIVIDADMonica ViceraNo ratings yet
- Iii. Nola PenderDocument3 pagesIii. Nola PenderBSN-2F Neutral Axis SiazonNo ratings yet
- Funda Lesson1 Health and WellnessDocument5 pagesFunda Lesson1 Health and WellnessAzTech 233No ratings yet
- HPM and H and B - Daryl E. CandoDocument41 pagesHPM and H and B - Daryl E. CandoDaryl CandoNo ratings yet
- CHN Reviewer PrelimDocument19 pagesCHN Reviewer PrelimCher Ann RuilesNo ratings yet
- Penders Health Promotion ModelDocument7 pagesPenders Health Promotion ModelANIME SOLONo ratings yet
- The Health Promotion Model (Nola J. Pender) : SupratmanDocument11 pagesThe Health Promotion Model (Nola J. Pender) : SupratmanNugraha PratamaNo ratings yet
- A.Nola Pender Nola Pender Health Promotion ModelDocument12 pagesA.Nola Pender Nola Pender Health Promotion ModelNathaniel PulidoNo ratings yet
- Nola J. Pender: The Health Adaptation ModelDocument35 pagesNola J. Pender: The Health Adaptation ModelCharmaine Gem Aganon PeregrinoNo ratings yet
- TFN Reviewer Third ExaminationDocument31 pagesTFN Reviewer Third ExaminationJoel CastilloNo ratings yet
- Health Promotion Model: Group 3 Justine Nikki Calumpit Cherry Lou Diaz Michelle Clariss Go Erica ManejaDocument16 pagesHealth Promotion Model: Group 3 Justine Nikki Calumpit Cherry Lou Diaz Michelle Clariss Go Erica ManejaKing Aldus ConstantinoNo ratings yet
- Health Promotion ModelDocument9 pagesHealth Promotion ModelSneha100% (1)
- Health Behavioral Theories Ling Yen Pan 2013Document27 pagesHealth Behavioral Theories Ling Yen Pan 2013abbasbelkoaishaNo ratings yet
- Pender's Health Promotion Model: Presented by Jessica Konopka, Nicky Reed, Nacole Shafer, Cheryl Shapiro, & Sara WaltersDocument21 pagesPender's Health Promotion Model: Presented by Jessica Konopka, Nicky Reed, Nacole Shafer, Cheryl Shapiro, & Sara Waltersjona phie MonteroNo ratings yet
- C1 NCM 102Document20 pagesC1 NCM 102Khecia Freanne TorresNo ratings yet
- Penders Health Promotion ModelDocument2 pagesPenders Health Promotion ModelRIK HAROLD GATPANDANNo ratings yet
- Theories Related To Health PromotionDocument12 pagesTheories Related To Health PromotionJamie Rose FontanillaNo ratings yet
- Community Health Nursing IiDocument17 pagesCommunity Health Nursing IiSheila Mae TubacNo ratings yet
- Major Concepts of The Health Promotion ModelDocument2 pagesMajor Concepts of The Health Promotion Modelrhycelayon304No ratings yet
- Untitled Design - 072224Document16 pagesUntitled Design - 072224muzammilsutar8No ratings yet
- Theories in Health EducationDocument30 pagesTheories in Health EducationshaneNo ratings yet
- TFN The NotesDocument24 pagesTFN The Notesdaniela bareteNo ratings yet
- Chnmidterm 2 NDDocument9 pagesChnmidterm 2 NDMharlynne Nezlou L. PoliranNo ratings yet
- TFNDocument6 pagesTFNHannah IsraelNo ratings yet
- Health Promotion ModelDocument3 pagesHealth Promotion ModelJehannah Dayanara Berdan HayudiniNo ratings yet
- TFN Oral Rev ReviewerDocument6 pagesTFN Oral Rev ReviewerDela Cruz Clarizza BiancaNo ratings yet
- Nola J. PenderDocument5 pagesNola J. PenderSofia Marie GalendezNo ratings yet
- Marife Reyes (Report)Document8 pagesMarife Reyes (Report)Francis AjeroNo ratings yet
- CHN 2 Midterms PDFDocument9 pagesCHN 2 Midterms PDFStephanie Mhae TabasaNo ratings yet
- CHNDocument119 pagesCHNCanny CańasNo ratings yet
- Health and BehaviorDocument5 pagesHealth and BehaviorJewell M. LicupNo ratings yet
- Historical Development and Concepts of Health EducationDocument5 pagesHistorical Development and Concepts of Health EducationNil GyiNo ratings yet
- Anika Jade Alican COMPUTER Grd5 ST - AgathaDocument3 pagesAnika Jade Alican COMPUTER Grd5 ST - AgathaChelsea Taguiam GuillermoNo ratings yet
- Ethical ConsiderationsDocument4 pagesEthical ConsiderationsChelsea Taguiam GuillermoNo ratings yet
- Project PhilosophyDocument9 pagesProject PhilosophyChelsea Taguiam GuillermoNo ratings yet
- ResearchDocument16 pagesResearchChelsea Taguiam GuillermoNo ratings yet
- Health Education RevDocument13 pagesHealth Education RevChelsea Taguiam GuillermoNo ratings yet
- ARFA Nov122022 COLLADODocument2 pagesARFA Nov122022 COLLADOChelsea Taguiam GuillermoNo ratings yet
- SCRIPT FatsssDocument6 pagesSCRIPT FatsssChelsea Taguiam GuillermoNo ratings yet
- GUILLERMO - CHELSEA - ST - CHRISTINA OF TYRE - P.EDocument2 pagesGUILLERMO - CHELSEA - ST - CHRISTINA OF TYRE - P.EChelsea Taguiam GuillermoNo ratings yet
- Ass RelssDocument1 pageAss RelssChelsea Taguiam GuillermoNo ratings yet
- Guillermo, Chelsea Reinne - ST - Christina of Tyre - Learning Task 5Document2 pagesGuillermo, Chelsea Reinne - ST - Christina of Tyre - Learning Task 5Chelsea Taguiam GuillermoNo ratings yet
- g12 Module Week 6 - GuillermoDocument2 pagesg12 Module Week 6 - GuillermoChelsea Taguiam GuillermoNo ratings yet
- Faith-Experience December - Guillermo - BSNDocument4 pagesFaith-Experience December - Guillermo - BSNChelsea Taguiam GuillermoNo ratings yet
- G12 HG MODULE FINAL TERM WEEK 7 - GuillermoDocument4 pagesG12 HG MODULE FINAL TERM WEEK 7 - GuillermoChelsea Taguiam GuillermoNo ratings yet
- The Impact of Globalization On Communication - SABUG JOHN DENVERDocument1 pageThe Impact of Globalization On Communication - SABUG JOHN DENVERChelsea Taguiam GuillermoNo ratings yet
- Guillermo, Chelsea Reinne T. March 17 2022Document2 pagesGuillermo, Chelsea Reinne T. March 17 2022Chelsea Taguiam GuillermoNo ratings yet
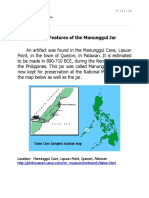
- Activity 2 The Features of The Manunggul Jar 2Document7 pagesActivity 2 The Features of The Manunggul Jar 2Chelsea Taguiam GuillermoNo ratings yet
- December - Faith Experience - GuillermoDocument4 pagesDecember - Faith Experience - GuillermoChelsea Taguiam GuillermoNo ratings yet
- Fire Pump Set Technical InformationDocument3 pagesFire Pump Set Technical InformationLEONEL SOTTONo ratings yet
- NEMA-WC 74 - ICEA S-93-639 5-46kV Shielded Power CableDocument97 pagesNEMA-WC 74 - ICEA S-93-639 5-46kV Shielded Power CableTrầnHữuHòaNo ratings yet
- A Presentation On: Presented byDocument67 pagesA Presentation On: Presented byOlufemi KolawoleNo ratings yet
- Project Materials Handling and Preservation ProcedureDocument2 pagesProject Materials Handling and Preservation ProcedureGbenga Mobolade100% (3)
- Plot PlanDocument5 pagesPlot PlandasubhaiNo ratings yet
- Black Vulture MGMT PlanDocument24 pagesBlack Vulture MGMT Planapi-662406940No ratings yet
- Anaesthesia Workstation 4Document120 pagesAnaesthesia Workstation 4john georgeNo ratings yet
- OSP FO WorkDocument50 pagesOSP FO WorkARCC2030No ratings yet
- Vocabulary BuildingDocument5 pagesVocabulary BuildingSaima AbediNo ratings yet
- ADD2407217Document2 pagesADD2407217SUMIT PATELNo ratings yet
- Especificaciones de Valvulas Normas APIDocument2 pagesEspecificaciones de Valvulas Normas APIÀngel Rodriguez0% (1)
- The One Minute ManagerDocument20 pagesThe One Minute ManagerYashwant J100% (2)
- Labour Law Thailand English VersionDocument24 pagesLabour Law Thailand English VersionDavid LeoNo ratings yet
- Sampling Procedure and Tables For InspectionDocument43 pagesSampling Procedure and Tables For InspectionAnonymous AoTZuNvxNo ratings yet
- University of Cagayan Valley School of Criminology 32Document6 pagesUniversity of Cagayan Valley School of Criminology 32janna danNo ratings yet
- Service Manual: Codemaster XL+ (M1722B) Defibrillator/MonitorDocument260 pagesService Manual: Codemaster XL+ (M1722B) Defibrillator/Monitorm.torresNo ratings yet
- MGMT 591-Final Project Duewk7Document13 pagesMGMT 591-Final Project Duewk7jmquint00100% (1)
- Student Exploration: Polarity and Intermolecular ForcesDocument7 pagesStudent Exploration: Polarity and Intermolecular ForcesZhaoxiaotang EstherNo ratings yet
- Oral Iron ProductsDocument2 pagesOral Iron ProductsOlga BabiiNo ratings yet
- Catalogo SiouxDocument13 pagesCatalogo Siouxdef2009100% (1)
- De Jong 2013 ACS Catalysis Catalysts For Production of Lower Olefins From Synthesis Gas - A Review PDFDocument20 pagesDe Jong 2013 ACS Catalysis Catalysts For Production of Lower Olefins From Synthesis Gas - A Review PDFSohail FarooqNo ratings yet
- Honda Vision 110 2012 ManualDocument99 pagesHonda Vision 110 2012 ManualLupu HarambeNo ratings yet
- Ce208 Lab ReportDocument3 pagesCe208 Lab ReportHarsh SharmaNo ratings yet
- PPS Steam Boiler Operation and AuxiliariesDocument9 pagesPPS Steam Boiler Operation and AuxiliariesAraNo ratings yet
- AstronomyDocument20 pagesAstronomyAjay Kumar DasNo ratings yet
- Solid Waste Management: By: Dr. Mohd Ariffin Abu HassanDocument47 pagesSolid Waste Management: By: Dr. Mohd Ariffin Abu HassanFaiqa Abd Aziz100% (1)
- Human Genome ProjectDocument57 pagesHuman Genome ProjectIsma Velasco100% (1)