
Theatre Ventilation
Theatre Ventilation
You might also like
- Guidelines Based On VDI 6022 PDFDocument7 pagesGuidelines Based On VDI 6022 PDFbauer_mendoza3510100% (2)
- Detailed Lesson Plan in Getaway DrugsDocument9 pagesDetailed Lesson Plan in Getaway DrugsJovelyn Takilid75% (4)
- 100 Modelos B2 EOI Inglés.Document150 pages100 Modelos B2 EOI Inglés.Hannah Gray100% (2)
- MOSAIC HP - Operation Manual - 4100110311 - Rev1.1Document137 pagesMOSAIC HP - Operation Manual - 4100110311 - Rev1.1Alexandre Berthon100% (1)
- DNP Essentials EportfolioDocument3 pagesDNP Essentials Eportfolioapi-246869268100% (1)
- Anae 15542Document8 pagesAnae 15542Ervin SeborgaNo ratings yet
- Environmental Controls in Operating Theatres: S. Dharan and D. PittetDocument6 pagesEnvironmental Controls in Operating Theatres: S. Dharan and D. PittetDinda FSNo ratings yet
- Jurnal Deskriptif IngDocument6 pagesJurnal Deskriptif IngAulin putri damayantiNo ratings yet
- Ventilation Performance in The Operating Theatre Against Airborne Infection Numerical Study On An Ultra-Clean SystemDocument10 pagesVentilation Performance in The Operating Theatre Against Airborne Infection Numerical Study On An Ultra-Clean SystemVL KohNo ratings yet
- Tay 2020Document2 pagesTay 2020Corin Boice TelloNo ratings yet
- Environmental Controls in Operating Theatres: S. Dharan and D. PittetDocument6 pagesEnvironmental Controls in Operating Theatres: S. Dharan and D. PittetDinda FSNo ratings yet
- Microbiological Commissioning and MonitoringDocument28 pagesMicrobiological Commissioning and MonitoringSungkakNo ratings yet
- Spotlight: Lancet Respir Med 2020Document2 pagesSpotlight: Lancet Respir Med 2020kayegi8666No ratings yet
- COVID-19 Management in HongKongDocument1 pageCOVID-19 Management in HongKongShahzad KamranNo ratings yet
- A Review of Intraoperative Protective Ventilation: Review Article Open AccessDocument9 pagesA Review of Intraoperative Protective Ventilation: Review Article Open AccessLeiniker NavarroNo ratings yet
- Hospital Diffusers EngineeringDocument26 pagesHospital Diffusers Engineeringamechmar5935100% (1)
- Revista Española de Anestesiología y Reanimación: Is Direct Laryngoscopy Dead? Long Live The Video LaryngosDocument4 pagesRevista Española de Anestesiología y Reanimación: Is Direct Laryngoscopy Dead? Long Live The Video LaryngosNati PadillaNo ratings yet
- Operating Room Ventilation With Laminar Airflow ShowsDocument6 pagesOperating Room Ventilation With Laminar Airflow Showsitho23No ratings yet
- Medical Hypotheses: SciencedirectDocument5 pagesMedical Hypotheses: SciencedirectRizka DaengNo ratings yet
- Experimental Investigation of Indoor Aerosol Dispersion and Accumulation in The Context of COVID-19: Effects of Masks and VentilationDocument14 pagesExperimental Investigation of Indoor Aerosol Dispersion and Accumulation in The Context of COVID-19: Effects of Masks and VentilationDaniel CarvajalNo ratings yet
- Safe Surgery 2Document5 pagesSafe Surgery 2Masrun FatanahNo ratings yet
- Airflow Dynamics in An Emergency Department: A CFD Simulation Study To Analyse COVID-19 DispersionDocument11 pagesAirflow Dynamics in An Emergency Department: A CFD Simulation Study To Analyse COVID-19 DispersionNoufal JamousNo ratings yet
- Use of Helmet Cpap in COVID-19 - A Practical ReviewDocument10 pagesUse of Helmet Cpap in COVID-19 - A Practical ReviewDoménica SánchezNo ratings yet
- Air Quality - OR - TaiwanDocument6 pagesAir Quality - OR - TaiwanKanokwan BorwornphiphattanachaiNo ratings yet
- Numerical Simulation On A Horizontal Airflow For Airborne Particles ControlDocument6 pagesNumerical Simulation On A Horizontal Airflow For Airborne Particles ControlMarioNo ratings yet
- Effective of Ventilation System in Healthcare Facilities During Handling With Pandemic COVID-19 in Egypt Effective of Ventilation System in Healthcare Facilities During Handling Wi..Document7 pagesEffective of Ventilation System in Healthcare Facilities During Handling With Pandemic COVID-19 in Egypt Effective of Ventilation System in Healthcare Facilities During Handling Wi..Widarma Atmaja, I KomangNo ratings yet
- Jurnal OK-CovidDocument8 pagesJurnal OK-CovidAchmad FauzyNo ratings yet
- Videolaryngoscopy Increases Mouth-To-Mouth' Distance Compared With Direct LaryngosDocument2 pagesVideolaryngoscopy Increases Mouth-To-Mouth' Distance Compared With Direct LaryngosHugo Robles GómezNo ratings yet
- Vacuum Aerosol 4Document10 pagesVacuum Aerosol 4khamilatusyNo ratings yet
- Journal Appraisal 2Document14 pagesJournal Appraisal 2Norjetalexis Maningo CabreraNo ratings yet
- Impact of Gas Humidification and Nebulizer PositioDocument12 pagesImpact of Gas Humidification and Nebulizer PositioRamya DivyaNo ratings yet
- Transmission of Infectious Diseases Air TravelDocument8 pagesTransmission of Infectious Diseases Air Travelbenjamin.arfi06No ratings yet
- 1 s2.0 S1479666X20301888 MainDocument5 pages1 s2.0 S1479666X20301888 MainTécnicos CredineNo ratings yet
- Applications of Ultraviolet Germicidal Irradiation Disinfection in Health Care Facilities: Effective Adjunct, But Not Stand-Alone TechnologyDocument12 pagesApplications of Ultraviolet Germicidal Irradiation Disinfection in Health Care Facilities: Effective Adjunct, But Not Stand-Alone TechnologyDavid Adolfo Paez MolinaNo ratings yet
- JHI Laminar Airflow Versus Turbulent Airflow in Simulated Total Hip Arthroplasty PIIS0195670121002425Document7 pagesJHI Laminar Airflow Versus Turbulent Airflow in Simulated Total Hip Arthroplasty PIIS0195670121002425Anders ENo ratings yet
- Bronchoscopic Management of Prolonged Air Leak: Sevak Keshishyan, Alberto E. Revelo, Oleg EpelbaumDocument13 pagesBronchoscopic Management of Prolonged Air Leak: Sevak Keshishyan, Alberto E. Revelo, Oleg EpelbaumFranco Xabier Milos RuizNo ratings yet
- Laminar Flow in Orthopaedic Operations - Essential If You CanDocument15 pagesLaminar Flow in Orthopaedic Operations - Essential If You CanSamiYousifNo ratings yet
- Oral Oncology: CORONA-steps For Tracheotomy in COVID-19 Patients: A Staff-Safe Method For Airway ManagementDocument3 pagesOral Oncology: CORONA-steps For Tracheotomy in COVID-19 Patients: A Staff-Safe Method For Airway ManagementCorin Boice TelloNo ratings yet
- Hospital Air Curtain Systems: Dan Int-Hout, Chief Engineer Gerry Cook, Sr. Project EngineerDocument14 pagesHospital Air Curtain Systems: Dan Int-Hout, Chief Engineer Gerry Cook, Sr. Project EngineerSolymanElsayedSolymanNo ratings yet
- It Wasn't Raining When Noah Built The ArkDocument4 pagesIt Wasn't Raining When Noah Built The ArkocramusNo ratings yet
- High-Flow, Noninvasive Ventilation and Awake (Nonintubation) Proning in Patients With Coronavirus Disease 2019 With Respiratory FailureDocument11 pagesHigh-Flow, Noninvasive Ventilation and Awake (Nonintubation) Proning in Patients With Coronavirus Disease 2019 With Respiratory FailureCamila Fernanda Rivera ArayaNo ratings yet
- A 1180 8527 PDFDocument5 pagesA 1180 8527 PDFPaulHerreraNo ratings yet
- What Is New in Airway ManagementDocument4 pagesWhat Is New in Airway Managementkarely EspinozaNo ratings yet
- Effect of Ventilation Strategies On Infection Control Inside Operating Theatres PDFDocument17 pagesEffect of Ventilation Strategies On Infection Control Inside Operating Theatres PDFValerika GurschiNo ratings yet
- UVGI ApplicationDocument12 pagesUVGI Applicationsakchai2012No ratings yet
- Coronavirus Disease 2019: Epidemiological Factors During Aerosol-Generating Medical ProceduresDocument4 pagesCoronavirus Disease 2019: Epidemiological Factors During Aerosol-Generating Medical ProceduresAbrar Hendri PutraNo ratings yet
- The Laboratory Characterization of Fugitive AerosoDocument7 pagesThe Laboratory Characterization of Fugitive AerosoRamya DivyaNo ratings yet
- Jamda: Richard M. Lynch PHD, Reginald Goring BsDocument2 pagesJamda: Richard M. Lynch PHD, Reginald Goring BsWidarma Atmaja, I KomangNo ratings yet
- Divino, Quiroz Case Study No. 2 - Covid-19Document9 pagesDivino, Quiroz Case Study No. 2 - Covid-19AngelikaNo ratings yet
- Weiser 2018Document10 pagesWeiser 2018Syahrul MuhammadiyahNo ratings yet
- CRISIS Ventilator A 3D Printed Option For Ventilator Surge in Mass Respiratory PandemicsDocument8 pagesCRISIS Ventilator A 3D Printed Option For Ventilator Surge in Mass Respiratory PandemicsdjaroslavskyNo ratings yet
- Airway StentDocument5 pagesAirway StentYanuar AbdulhayNo ratings yet
- Technological Advancements in The Care of The Trauma PatientDocument11 pagesTechnological Advancements in The Care of The Trauma PatientmeillonchazaroNo ratings yet
- Public Health Ontario - Covid 19 Hvac Systems in BuildingsDocument15 pagesPublic Health Ontario - Covid 19 Hvac Systems in BuildingsBerk KÖTEŞLİNo ratings yet
- Cruces Et Al-2020-Critical CareDocument10 pagesCruces Et Al-2020-Critical CareminiypuntoNo ratings yet
- 14 2 206Document5 pages14 2 206Abdullah ZahidNo ratings yet
- Micro Commissioning of Theatres HIS PaperDocument44 pagesMicro Commissioning of Theatres HIS PaperAbderrezak Merzak AbdouNo ratings yet
- Critical Incidents of The Respiratory SystemDocument6 pagesCritical Incidents of The Respiratory SystemLia Whulan11No ratings yet
- Tracheostomy Management During The COVID-19 PandemicDocument3 pagesTracheostomy Management During The COVID-19 Pandemicika lestariNo ratings yet
- Supraglotic DivicesDocument5 pagesSupraglotic DivicesDavid OrtizNo ratings yet
- 1 s2.0 S0195670106002866 MainDocument15 pages1 s2.0 S0195670106002866 MainAfraNo ratings yet
- Cánula Asimétrica en Paciente HipoxémicoDocument12 pagesCánula Asimétrica en Paciente HipoxémicoEdgar PandoNo ratings yet
- Burden of Surgical Site Infections in The NetherlandsDocument10 pagesBurden of Surgical Site Infections in The NetherlandsKanokwan BorwornphiphattanachaiNo ratings yet
- Control and Management of Hospital Indoor Air QualityDocument8 pagesControl and Management of Hospital Indoor Air QualityKanokwan BorwornphiphattanachaiNo ratings yet
- Air Quality - OR - TaiwanDocument6 pagesAir Quality - OR - TaiwanKanokwan BorwornphiphattanachaiNo ratings yet
- Air Sampling SOPDocument4 pagesAir Sampling SOPKanokwan BorwornphiphattanachaiNo ratings yet
- Recorderis Ingles - Corte 1Document12 pagesRecorderis Ingles - Corte 1Harold MarriagaNo ratings yet
- Silver Iodide MSDS: Section 1: Chemical Product and Company IdentificationDocument5 pagesSilver Iodide MSDS: Section 1: Chemical Product and Company IdentificationelsadwihermiatiNo ratings yet
- Pharmacoeconomics: Presented By: M. Krishna Aishwarya M. Pharmacy Ii/Ii Year Drug Regulatory AffairsDocument16 pagesPharmacoeconomics: Presented By: M. Krishna Aishwarya M. Pharmacy Ii/Ii Year Drug Regulatory AffairsaishuNo ratings yet
- Cold Laser BookDocument26 pagesCold Laser BookJorge Segui100% (1)
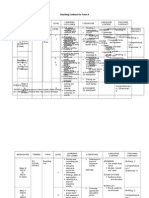
- Teaching Contract F4Document16 pagesTeaching Contract F4Wardah BajraiNo ratings yet
- SoftenerDocument2 pagesSoftenerUniversal ExpoNo ratings yet
- Proposed SP Ordinance 15-002-2019Document5 pagesProposed SP Ordinance 15-002-2019JudeRamosNo ratings yet
- TOS 2nd Quarter ExamDocument3 pagesTOS 2nd Quarter Examxandra joy abadezaNo ratings yet
- MudrasDocument3 pagesMudrasPraveen Alinkeel100% (1)
- Kalaburagi Vol - 1 PDFDocument650 pagesKalaburagi Vol - 1 PDFMadhusudan ChilukotiNo ratings yet
- Certificate of AbsenceDocument1 pageCertificate of AbsenceFrancisco RamirezNo ratings yet
- Jack Martin CV Sept-16Document2 pagesJack Martin CV Sept-16Anonymous fhs6rxNo ratings yet
- Plaintiff'S Class Action Complaint Case SummaryDocument24 pagesPlaintiff'S Class Action Complaint Case SummaryCBS 11 News100% (1)
- Chpater-9 XI NotesDocument7 pagesChpater-9 XI NotesAarsh AgarwalNo ratings yet
- 31 - Past Perfect Tense (İleri) - Okuma ParçasıDocument10 pages31 - Past Perfect Tense (İleri) - Okuma Parçası28 eylülNo ratings yet
- LEED Green Associate Practice QnsDocument194 pagesLEED Green Associate Practice Qnsmitri100% (1)
- Healthcare Waste ManagementDocument53 pagesHealthcare Waste ManagementErilyn MarinduqueNo ratings yet
- DR Barry SearsDocument37 pagesDR Barry SearskarllozaraujoNo ratings yet
- HIRARC Report Best ContactDocument5 pagesHIRARC Report Best ContactDon McleanNo ratings yet
- ErgonomicsDocument15 pagesErgonomicsdtmNo ratings yet
- Gracella Irwana - G - Pert 05-06 - Sia - 1Document51 pagesGracella Irwana - G - Pert 05-06 - Sia - 1Gracella IrwanaNo ratings yet
- CHN Bullets PDFDocument55 pagesCHN Bullets PDFVinu PoojapranavamNo ratings yet
- Laser in Fixed ProsthodonticsDocument6 pagesLaser in Fixed Prosthodontics2oclock0% (1)
- Keep Safe Everyone. God Bless 2C.: 3. Deadline For This Activity Will Be On Sunday March 29, 2020 11:59PMDocument10 pagesKeep Safe Everyone. God Bless 2C.: 3. Deadline For This Activity Will Be On Sunday March 29, 2020 11:59PMJœnríčk AzueloNo ratings yet
- 12 in Series III SweepDocument60 pages12 in Series III SweepEric ConNNo ratings yet
- 1 s2.0 S0169409X21002830 MainDocument31 pages1 s2.0 S0169409X21002830 MainRocio Angie Navarro SeguraNo ratings yet



























































































Download as pdf or txt
You might also like
- Guidelines Based On VDI 6022 PDFDocument7 pagesGuidelines Based On VDI 6022 PDFbauer_mendoza3510100% (2)
- Detailed Lesson Plan in Getaway DrugsDocument9 pagesDetailed Lesson Plan in Getaway DrugsJovelyn Takilid75% (4)
- 100 Modelos B2 EOI Inglés.Document150 pages100 Modelos B2 EOI Inglés.Hannah Gray100% (2)
- MOSAIC HP - Operation Manual - 4100110311 - Rev1.1Document137 pagesMOSAIC HP - Operation Manual - 4100110311 - Rev1.1Alexandre Berthon100% (1)
- DNP Essentials EportfolioDocument3 pagesDNP Essentials Eportfolioapi-246869268100% (1)
- Anae 15542Document8 pagesAnae 15542Ervin SeborgaNo ratings yet
- Environmental Controls in Operating Theatres: S. Dharan and D. PittetDocument6 pagesEnvironmental Controls in Operating Theatres: S. Dharan and D. PittetDinda FSNo ratings yet
- Jurnal Deskriptif IngDocument6 pagesJurnal Deskriptif IngAulin putri damayantiNo ratings yet
- Ventilation Performance in The Operating Theatre Against Airborne Infection Numerical Study On An Ultra-Clean SystemDocument10 pagesVentilation Performance in The Operating Theatre Against Airborne Infection Numerical Study On An Ultra-Clean SystemVL KohNo ratings yet
- Tay 2020Document2 pagesTay 2020Corin Boice TelloNo ratings yet
- Environmental Controls in Operating Theatres: S. Dharan and D. PittetDocument6 pagesEnvironmental Controls in Operating Theatres: S. Dharan and D. PittetDinda FSNo ratings yet
- Microbiological Commissioning and MonitoringDocument28 pagesMicrobiological Commissioning and MonitoringSungkakNo ratings yet
- Spotlight: Lancet Respir Med 2020Document2 pagesSpotlight: Lancet Respir Med 2020kayegi8666No ratings yet
- COVID-19 Management in HongKongDocument1 pageCOVID-19 Management in HongKongShahzad KamranNo ratings yet
- A Review of Intraoperative Protective Ventilation: Review Article Open AccessDocument9 pagesA Review of Intraoperative Protective Ventilation: Review Article Open AccessLeiniker NavarroNo ratings yet
- Hospital Diffusers EngineeringDocument26 pagesHospital Diffusers Engineeringamechmar5935100% (1)
- Revista Española de Anestesiología y Reanimación: Is Direct Laryngoscopy Dead? Long Live The Video LaryngosDocument4 pagesRevista Española de Anestesiología y Reanimación: Is Direct Laryngoscopy Dead? Long Live The Video LaryngosNati PadillaNo ratings yet
- Operating Room Ventilation With Laminar Airflow ShowsDocument6 pagesOperating Room Ventilation With Laminar Airflow Showsitho23No ratings yet
- Medical Hypotheses: SciencedirectDocument5 pagesMedical Hypotheses: SciencedirectRizka DaengNo ratings yet
- Experimental Investigation of Indoor Aerosol Dispersion and Accumulation in The Context of COVID-19: Effects of Masks and VentilationDocument14 pagesExperimental Investigation of Indoor Aerosol Dispersion and Accumulation in The Context of COVID-19: Effects of Masks and VentilationDaniel CarvajalNo ratings yet
- Safe Surgery 2Document5 pagesSafe Surgery 2Masrun FatanahNo ratings yet
- Airflow Dynamics in An Emergency Department: A CFD Simulation Study To Analyse COVID-19 DispersionDocument11 pagesAirflow Dynamics in An Emergency Department: A CFD Simulation Study To Analyse COVID-19 DispersionNoufal JamousNo ratings yet
- Use of Helmet Cpap in COVID-19 - A Practical ReviewDocument10 pagesUse of Helmet Cpap in COVID-19 - A Practical ReviewDoménica SánchezNo ratings yet
- Air Quality - OR - TaiwanDocument6 pagesAir Quality - OR - TaiwanKanokwan BorwornphiphattanachaiNo ratings yet
- Numerical Simulation On A Horizontal Airflow For Airborne Particles ControlDocument6 pagesNumerical Simulation On A Horizontal Airflow For Airborne Particles ControlMarioNo ratings yet
- Effective of Ventilation System in Healthcare Facilities During Handling With Pandemic COVID-19 in Egypt Effective of Ventilation System in Healthcare Facilities During Handling Wi..Document7 pagesEffective of Ventilation System in Healthcare Facilities During Handling With Pandemic COVID-19 in Egypt Effective of Ventilation System in Healthcare Facilities During Handling Wi..Widarma Atmaja, I KomangNo ratings yet
- Jurnal OK-CovidDocument8 pagesJurnal OK-CovidAchmad FauzyNo ratings yet
- Videolaryngoscopy Increases Mouth-To-Mouth' Distance Compared With Direct LaryngosDocument2 pagesVideolaryngoscopy Increases Mouth-To-Mouth' Distance Compared With Direct LaryngosHugo Robles GómezNo ratings yet
- Vacuum Aerosol 4Document10 pagesVacuum Aerosol 4khamilatusyNo ratings yet
- Journal Appraisal 2Document14 pagesJournal Appraisal 2Norjetalexis Maningo CabreraNo ratings yet
- Impact of Gas Humidification and Nebulizer PositioDocument12 pagesImpact of Gas Humidification and Nebulizer PositioRamya DivyaNo ratings yet
- Transmission of Infectious Diseases Air TravelDocument8 pagesTransmission of Infectious Diseases Air Travelbenjamin.arfi06No ratings yet
- 1 s2.0 S1479666X20301888 MainDocument5 pages1 s2.0 S1479666X20301888 MainTécnicos CredineNo ratings yet
- Applications of Ultraviolet Germicidal Irradiation Disinfection in Health Care Facilities: Effective Adjunct, But Not Stand-Alone TechnologyDocument12 pagesApplications of Ultraviolet Germicidal Irradiation Disinfection in Health Care Facilities: Effective Adjunct, But Not Stand-Alone TechnologyDavid Adolfo Paez MolinaNo ratings yet
- JHI Laminar Airflow Versus Turbulent Airflow in Simulated Total Hip Arthroplasty PIIS0195670121002425Document7 pagesJHI Laminar Airflow Versus Turbulent Airflow in Simulated Total Hip Arthroplasty PIIS0195670121002425Anders ENo ratings yet
- Bronchoscopic Management of Prolonged Air Leak: Sevak Keshishyan, Alberto E. Revelo, Oleg EpelbaumDocument13 pagesBronchoscopic Management of Prolonged Air Leak: Sevak Keshishyan, Alberto E. Revelo, Oleg EpelbaumFranco Xabier Milos RuizNo ratings yet
- Laminar Flow in Orthopaedic Operations - Essential If You CanDocument15 pagesLaminar Flow in Orthopaedic Operations - Essential If You CanSamiYousifNo ratings yet
- Oral Oncology: CORONA-steps For Tracheotomy in COVID-19 Patients: A Staff-Safe Method For Airway ManagementDocument3 pagesOral Oncology: CORONA-steps For Tracheotomy in COVID-19 Patients: A Staff-Safe Method For Airway ManagementCorin Boice TelloNo ratings yet
- Hospital Air Curtain Systems: Dan Int-Hout, Chief Engineer Gerry Cook, Sr. Project EngineerDocument14 pagesHospital Air Curtain Systems: Dan Int-Hout, Chief Engineer Gerry Cook, Sr. Project EngineerSolymanElsayedSolymanNo ratings yet
- It Wasn't Raining When Noah Built The ArkDocument4 pagesIt Wasn't Raining When Noah Built The ArkocramusNo ratings yet
- High-Flow, Noninvasive Ventilation and Awake (Nonintubation) Proning in Patients With Coronavirus Disease 2019 With Respiratory FailureDocument11 pagesHigh-Flow, Noninvasive Ventilation and Awake (Nonintubation) Proning in Patients With Coronavirus Disease 2019 With Respiratory FailureCamila Fernanda Rivera ArayaNo ratings yet
- A 1180 8527 PDFDocument5 pagesA 1180 8527 PDFPaulHerreraNo ratings yet
- What Is New in Airway ManagementDocument4 pagesWhat Is New in Airway Managementkarely EspinozaNo ratings yet
- Effect of Ventilation Strategies On Infection Control Inside Operating Theatres PDFDocument17 pagesEffect of Ventilation Strategies On Infection Control Inside Operating Theatres PDFValerika GurschiNo ratings yet
- UVGI ApplicationDocument12 pagesUVGI Applicationsakchai2012No ratings yet
- Coronavirus Disease 2019: Epidemiological Factors During Aerosol-Generating Medical ProceduresDocument4 pagesCoronavirus Disease 2019: Epidemiological Factors During Aerosol-Generating Medical ProceduresAbrar Hendri PutraNo ratings yet
- The Laboratory Characterization of Fugitive AerosoDocument7 pagesThe Laboratory Characterization of Fugitive AerosoRamya DivyaNo ratings yet
- Jamda: Richard M. Lynch PHD, Reginald Goring BsDocument2 pagesJamda: Richard M. Lynch PHD, Reginald Goring BsWidarma Atmaja, I KomangNo ratings yet
- Divino, Quiroz Case Study No. 2 - Covid-19Document9 pagesDivino, Quiroz Case Study No. 2 - Covid-19AngelikaNo ratings yet
- Weiser 2018Document10 pagesWeiser 2018Syahrul MuhammadiyahNo ratings yet
- CRISIS Ventilator A 3D Printed Option For Ventilator Surge in Mass Respiratory PandemicsDocument8 pagesCRISIS Ventilator A 3D Printed Option For Ventilator Surge in Mass Respiratory PandemicsdjaroslavskyNo ratings yet
- Airway StentDocument5 pagesAirway StentYanuar AbdulhayNo ratings yet
- Technological Advancements in The Care of The Trauma PatientDocument11 pagesTechnological Advancements in The Care of The Trauma PatientmeillonchazaroNo ratings yet
- Public Health Ontario - Covid 19 Hvac Systems in BuildingsDocument15 pagesPublic Health Ontario - Covid 19 Hvac Systems in BuildingsBerk KÖTEŞLİNo ratings yet
- Cruces Et Al-2020-Critical CareDocument10 pagesCruces Et Al-2020-Critical CareminiypuntoNo ratings yet
- 14 2 206Document5 pages14 2 206Abdullah ZahidNo ratings yet
- Micro Commissioning of Theatres HIS PaperDocument44 pagesMicro Commissioning of Theatres HIS PaperAbderrezak Merzak AbdouNo ratings yet
- Critical Incidents of The Respiratory SystemDocument6 pagesCritical Incidents of The Respiratory SystemLia Whulan11No ratings yet
- Tracheostomy Management During The COVID-19 PandemicDocument3 pagesTracheostomy Management During The COVID-19 Pandemicika lestariNo ratings yet
- Supraglotic DivicesDocument5 pagesSupraglotic DivicesDavid OrtizNo ratings yet
- 1 s2.0 S0195670106002866 MainDocument15 pages1 s2.0 S0195670106002866 MainAfraNo ratings yet
- Cánula Asimétrica en Paciente HipoxémicoDocument12 pagesCánula Asimétrica en Paciente HipoxémicoEdgar PandoNo ratings yet
- Burden of Surgical Site Infections in The NetherlandsDocument10 pagesBurden of Surgical Site Infections in The NetherlandsKanokwan BorwornphiphattanachaiNo ratings yet
- Control and Management of Hospital Indoor Air QualityDocument8 pagesControl and Management of Hospital Indoor Air QualityKanokwan BorwornphiphattanachaiNo ratings yet
- Air Quality - OR - TaiwanDocument6 pagesAir Quality - OR - TaiwanKanokwan BorwornphiphattanachaiNo ratings yet
- Air Sampling SOPDocument4 pagesAir Sampling SOPKanokwan BorwornphiphattanachaiNo ratings yet
- Recorderis Ingles - Corte 1Document12 pagesRecorderis Ingles - Corte 1Harold MarriagaNo ratings yet
- Silver Iodide MSDS: Section 1: Chemical Product and Company IdentificationDocument5 pagesSilver Iodide MSDS: Section 1: Chemical Product and Company IdentificationelsadwihermiatiNo ratings yet
- Pharmacoeconomics: Presented By: M. Krishna Aishwarya M. Pharmacy Ii/Ii Year Drug Regulatory AffairsDocument16 pagesPharmacoeconomics: Presented By: M. Krishna Aishwarya M. Pharmacy Ii/Ii Year Drug Regulatory AffairsaishuNo ratings yet
- Cold Laser BookDocument26 pagesCold Laser BookJorge Segui100% (1)
- Teaching Contract F4Document16 pagesTeaching Contract F4Wardah BajraiNo ratings yet
- SoftenerDocument2 pagesSoftenerUniversal ExpoNo ratings yet
- Proposed SP Ordinance 15-002-2019Document5 pagesProposed SP Ordinance 15-002-2019JudeRamosNo ratings yet
- TOS 2nd Quarter ExamDocument3 pagesTOS 2nd Quarter Examxandra joy abadezaNo ratings yet
- MudrasDocument3 pagesMudrasPraveen Alinkeel100% (1)
- Kalaburagi Vol - 1 PDFDocument650 pagesKalaburagi Vol - 1 PDFMadhusudan ChilukotiNo ratings yet
- Certificate of AbsenceDocument1 pageCertificate of AbsenceFrancisco RamirezNo ratings yet
- Jack Martin CV Sept-16Document2 pagesJack Martin CV Sept-16Anonymous fhs6rxNo ratings yet
- Plaintiff'S Class Action Complaint Case SummaryDocument24 pagesPlaintiff'S Class Action Complaint Case SummaryCBS 11 News100% (1)
- Chpater-9 XI NotesDocument7 pagesChpater-9 XI NotesAarsh AgarwalNo ratings yet
- 31 - Past Perfect Tense (İleri) - Okuma ParçasıDocument10 pages31 - Past Perfect Tense (İleri) - Okuma Parçası28 eylülNo ratings yet
- LEED Green Associate Practice QnsDocument194 pagesLEED Green Associate Practice Qnsmitri100% (1)
- Healthcare Waste ManagementDocument53 pagesHealthcare Waste ManagementErilyn MarinduqueNo ratings yet
- DR Barry SearsDocument37 pagesDR Barry SearskarllozaraujoNo ratings yet
- HIRARC Report Best ContactDocument5 pagesHIRARC Report Best ContactDon McleanNo ratings yet
- ErgonomicsDocument15 pagesErgonomicsdtmNo ratings yet
- Gracella Irwana - G - Pert 05-06 - Sia - 1Document51 pagesGracella Irwana - G - Pert 05-06 - Sia - 1Gracella IrwanaNo ratings yet
- CHN Bullets PDFDocument55 pagesCHN Bullets PDFVinu PoojapranavamNo ratings yet
- Laser in Fixed ProsthodonticsDocument6 pagesLaser in Fixed Prosthodontics2oclock0% (1)
- Keep Safe Everyone. God Bless 2C.: 3. Deadline For This Activity Will Be On Sunday March 29, 2020 11:59PMDocument10 pagesKeep Safe Everyone. God Bless 2C.: 3. Deadline For This Activity Will Be On Sunday March 29, 2020 11:59PMJœnríčk AzueloNo ratings yet
- 12 in Series III SweepDocument60 pages12 in Series III SweepEric ConNNo ratings yet
- 1 s2.0 S0169409X21002830 MainDocument31 pages1 s2.0 S0169409X21002830 MainRocio Angie Navarro SeguraNo ratings yet