Download as docx, pdf, or txt
You might also like
- Percutaneous Renal Surgery A Practical Clinical HandbookDocument273 pagesPercutaneous Renal Surgery A Practical Clinical HandbookAlfredo Balcázar100% (1)
- Sexual Wisdom 4 Catholics Rev.15Document254 pagesSexual Wisdom 4 Catholics Rev.15vixtrNo ratings yet
- Surgery Insight: Natural Orifice Transluminal Endoscopic Surgery - An Analysis of Work To DateDocument12 pagesSurgery Insight: Natural Orifice Transluminal Endoscopic Surgery - An Analysis of Work To Datedocramanujam@rediffmailNo ratings yet
- Laparoscopic Surgery FinalDocument6 pagesLaparoscopic Surgery FinalIuli CojiNo ratings yet
- Laparoscopic SurgeryDocument7 pagesLaparoscopic Surgeryاحمد زغارىNo ratings yet
- MIS Part 1Document22 pagesMIS Part 1Abigail PaasaNo ratings yet
- Principles of Laparoscopic SurgeryDocument31 pagesPrinciples of Laparoscopic SurgeryKhalid Javeed Khan71% (7)
- Gaskin 1991Document13 pagesGaskin 1991mauricio ricardoNo ratings yet
- Gastrointestinal Interventional Endoscopy: Advanced TechniquesFrom EverandGastrointestinal Interventional Endoscopy: Advanced TechniquesMihir S. WaghNo ratings yet
- Artikel Tatalaksana APPDocument18 pagesArtikel Tatalaksana APPaulia agustinaNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument17 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistssafwanNo ratings yet
- SintesisDocument2 pagesSintesishipogloso74No ratings yet
- Laparoscopic Entry TechniquesDocument9 pagesLaparoscopic Entry TechniquesDougNo ratings yet
- Laparoscopic Surgery in Gynaecologic OncologyDocument7 pagesLaparoscopic Surgery in Gynaecologic OncologyManan BoobNo ratings yet
- 01 Introduction To Gynecology EndosDocument22 pages01 Introduction To Gynecology Endosrake sardevaNo ratings yet
- Laparoscopic Hysterectomy: Center of Minimally Invasive Gynecological Surgery Amper Kliniken AG, 85221 Dachau GermanyDocument25 pagesLaparoscopic Hysterectomy: Center of Minimally Invasive Gynecological Surgery Amper Kliniken AG, 85221 Dachau GermanyJunaida Afifa0% (1)
- Natural Orifice Transluminal Endoscopic SurgeryDocument11 pagesNatural Orifice Transluminal Endoscopic SurgeryMishel Rodriguez GuzmanNo ratings yet
- Colonoscopy Techniques (RA 2005)Document227 pagesColonoscopy Techniques (RA 2005)William Ricardo Effio Galvez100% (3)
- Thoracosopy VS VatsDocument13 pagesThoracosopy VS Vatshamm hammmoudNo ratings yet
- The Early History of Interventional EUDocument4 pagesThe Early History of Interventional EUDaniel MuñozNo ratings yet
- Endoscopy Is The InsertionDocument9 pagesEndoscopy Is The Insertionshuraj k.c.No ratings yet
- Exploratory LaparotomyDocument24 pagesExploratory Laparotomyyynu_sia48475No ratings yet
- Jurnal AppendicitisDocument10 pagesJurnal AppendicitisEwoJatmikoNo ratings yet
- Laparoscopic Hysterectomy and Decision When and WH PDFDocument5 pagesLaparoscopic Hysterectomy and Decision When and WH PDFDian SiregarNo ratings yet
- Principles of Minimal Invasive SurgeryDocument39 pagesPrinciples of Minimal Invasive SurgeryAvinash KannanNo ratings yet
- 2014 172 0 Retroperitoneal and Retrograde Total Laparoscopic Hysterectomy As A Standard Treatment in A Community Hospital 97 101 1Document5 pages2014 172 0 Retroperitoneal and Retrograde Total Laparoscopic Hysterectomy As A Standard Treatment in A Community Hospital 97 101 1Sarah MuharomahNo ratings yet
- LAPAROSCOPIC SURGERyDocument37 pagesLAPAROSCOPIC SURGERyabraham winartoNo ratings yet
- 10 Razones para Usar Eco en CriticosDocument13 pages10 Razones para Usar Eco en CriticosCurro MirallesNo ratings yet
- Laparoscopic Appendectomy As An AltDocument6 pagesLaparoscopic Appendectomy As An Altmarcela.orellanatNo ratings yet
- Collard J. Dis Esophagus 1994 7-66Document16 pagesCollard J. Dis Esophagus 1994 7-66vinicius.alvarez3No ratings yet
- Laparoscopic Ovariectomy in Small AnimalsDocument9 pagesLaparoscopic Ovariectomy in Small AnimalsIván A. P-BetancurtNo ratings yet
- Intraoperative Complications After Total Laparoscopic Hysterectomy: A Retrospective Study in Training Institute Richa Patel, Arun MorayDocument5 pagesIntraoperative Complications After Total Laparoscopic Hysterectomy: A Retrospective Study in Training Institute Richa Patel, Arun MorayArun MorayNo ratings yet
- Topic 1 Technologies in SurgeryDocument29 pagesTopic 1 Technologies in Surgeryzynna.abadiNo ratings yet
- Thora CosDocument20 pagesThora CosDani VélezNo ratings yet
- EndosDocument45 pagesEndosDr VirenNo ratings yet
- Review StrikturDocument13 pagesReview StrikturFryda 'buona' YantiNo ratings yet
- Magine Methods: Matta M.DDocument28 pagesMagine Methods: Matta M.Dmichal ben meronNo ratings yet
- Abdominal Access TechniquesDocument7 pagesAbdominal Access TechniquesdrmarcsNo ratings yet
- Exploratory LaparotomyDocument25 pagesExploratory Laparotomywinai13No ratings yet
- Hysterosalpingography 2009Document7 pagesHysterosalpingography 2009Niko MontgomeryNo ratings yet
- Laparoscopic Abdominal SurgeriesDocument45 pagesLaparoscopic Abdominal Surgeriesarnoldedwin50% (2)
- Laparoscopic Appendicectomy in Appendicular LumpDocument2 pagesLaparoscopic Appendicectomy in Appendicular LumpinventionjournalsNo ratings yet
- Coursebook-Echoscopy ch30Document23 pagesCoursebook-Echoscopy ch30Сергей СадовниковNo ratings yet
- Identification of Acute Appendicitis Using Euclidean Distance On Sonographic ImageDocument7 pagesIdentification of Acute Appendicitis Using Euclidean Distance On Sonographic ImageDr. R. BALUNo ratings yet
- 6 Laparoscopy Risks, Benefits and Complications REVIEWDocument11 pages6 Laparoscopy Risks, Benefits and Complications REVIEWnakaldNo ratings yet
- Endoscopy in Obstetric & GynaecologyDocument19 pagesEndoscopy in Obstetric & GynaecologyChrist PhanerooNo ratings yet
- Cutaneous Needle Aspirations in Liver DiseaseDocument6 pagesCutaneous Needle Aspirations in Liver DiseaseRhian BrimbleNo ratings yet
- Endoscopic Procedures on the SpineFrom EverandEndoscopic Procedures on the SpineJin-Sung KimNo ratings yet
- New Techniques in Genital Prolapse Surgery by Carl W. Zimmerman (Auth.), Peter VDocument325 pagesNew Techniques in Genital Prolapse Surgery by Carl W. Zimmerman (Auth.), Peter VMmmNo ratings yet
- Interventional Endoscopic UltrasoundDocument203 pagesInterventional Endoscopic UltrasoundAdhi SetiawanNo ratings yet
- Video-Assisted Thoracic Surgery For Esophagectomy: Evolution and ProsperityDocument8 pagesVideo-Assisted Thoracic Surgery For Esophagectomy: Evolution and ProsperityANSHUNo ratings yet
- Laparoscopic Appendicectomy in All Trimesters of PregnancyDocument7 pagesLaparoscopic Appendicectomy in All Trimesters of PregnancyJason CalvinNo ratings yet
- Teitelbaum 2018Document7 pagesTeitelbaum 2018victor ibarra romeroNo ratings yet
- Atlas of Minimally Invasive Surgery in Esophageal Carcinoma (Puntambekar)Document203 pagesAtlas of Minimally Invasive Surgery in Esophageal Carcinoma (Puntambekar)Ciprian-Nicolae MunteanNo ratings yet
- ROLE OF DIAGNOSTIC LAPROSCOPY IN MANAGEMENT OF ACUTE Abdomen FinalDocument80 pagesROLE OF DIAGNOSTIC LAPROSCOPY IN MANAGEMENT OF ACUTE Abdomen Finalnaveena reddyNo ratings yet
- Endoscopy: DR Rubeena Ali SR Radiology Deptt Amth/RlmcDocument58 pagesEndoscopy: DR Rubeena Ali SR Radiology Deptt Amth/RlmcMuhammad WasifNo ratings yet
- Endoscopy, Is A Way To Record Images of The Digestive Track ForDocument28 pagesEndoscopy, Is A Way To Record Images of The Digestive Track ForSunil Pandey100% (1)
- ErniaDocument37 pagesErniaOskar MaNo ratings yet
- DysmenorrheaDocument24 pagesDysmenorrheaChristopher MhagamaNo ratings yet
- Chapter 7: Pelvis and PerineumDocument22 pagesChapter 7: Pelvis and PerineumAlaz NellyNo ratings yet
- Hypotonic and Atonic Postpartum HemorrhageDocument10 pagesHypotonic and Atonic Postpartum HemorrhageAnonymous Tzn8RGBZ4No ratings yet
- The Sexual SelfDocument83 pagesThe Sexual Self-------No ratings yet
- Group 2B Case Study On Ectopic PregnancyDocument36 pagesGroup 2B Case Study On Ectopic PregnancyANGEL GADONo ratings yet
- Untitled28 PDFDocument14 pagesUntitled28 PDFElizabeth Leon100% (1)
- 36 - Acute Inversion of The UterusDocument10 pages36 - Acute Inversion of The Uterusdr_asaleh100% (1)
- Abdominal ExaminationDocument5 pagesAbdominal ExaminationAnuradha MauryaNo ratings yet
- SCRT NTSDocument11 pagesSCRT NTSBella CamposNo ratings yet
- Labor and Birth NotesDocument36 pagesLabor and Birth NotesJodi BairNo ratings yet
- Problems With The 4ps of LaborDocument10 pagesProblems With The 4ps of LaborhoohooNo ratings yet
- Explanation 2020 1Document315 pagesExplanation 2020 1Reshma Shaji PnsNo ratings yet
- Final Exam NCM 109. NotesDocument18 pagesFinal Exam NCM 109. Noteskenken the Explorer0% (1)
- Nursing Questions& AnswersDocument37 pagesNursing Questions& AnswersSanjeev KumarNo ratings yet
- The White BirdDocument4 pagesThe White BirdMoh Arimao100% (1)
- Instrumental Vaginal Delivery: Professor Roshan Ara QaziDocument27 pagesInstrumental Vaginal Delivery: Professor Roshan Ara Qazikaram008No ratings yet
- Case Report Jai 3Document8 pagesCase Report Jai 3EACMed Nursing Station 5th FloorNo ratings yet
- Overview: Intrapartum Care:: Oxytocin TheoryDocument5 pagesOverview: Intrapartum Care:: Oxytocin TheoryZach BuenavistaNo ratings yet
- Total Abdominal Hysterectomy: September 2016Document8 pagesTotal Abdominal Hysterectomy: September 2016nidoNo ratings yet
- Module 13 Reproductive System 2015-16 - FINAL VERSIONDocument28 pagesModule 13 Reproductive System 2015-16 - FINAL VERSIONidzniNo ratings yet
- Sample Case StudyDocument31 pagesSample Case StudyMary Grace Mas50% (2)
- Obstetrics Outline (MCHN) Chapter 1Document8 pagesObstetrics Outline (MCHN) Chapter 1Marinill Soliman100% (1)
- Uterine Prolaps1Document6 pagesUterine Prolaps1Ginsha GeorgeNo ratings yet
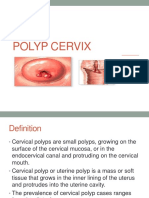
- Polyp CervixDocument14 pagesPolyp CervixT Horan100% (1)
- Pre-Prof Final Question PaperDocument56 pagesPre-Prof Final Question PaperRajaNo ratings yet
- Nle Pre Board June 2008 Npt2-Questions and RationaleDocument22 pagesNle Pre Board June 2008 Npt2-Questions and RationaleJacey Racho100% (1)
- Cot First QuarterDocument15 pagesCot First QuarterRowena Torres DahiligNo ratings yet
- Chordata and Vertebrata: Chapter - 8 Characters of Class Pisces (Fishes)Document7 pagesChordata and Vertebrata: Chapter - 8 Characters of Class Pisces (Fishes)Farrukh SaleemNo ratings yet
- Obstetrics OBDocument65 pagesObstetrics OBVicviclookTheking100% (1)