
Adult Antibiotic Prophylaxis For Urological Surgery
Adult Antibiotic Prophylaxis For Urological Surgery
You might also like
- Miscellaneous For FinalsDocument30 pagesMiscellaneous For Finalsjames.a.blairNo ratings yet
- Essentials of Internal MedicineDocument832 pagesEssentials of Internal MedicineEmanuelMC100% (79)
- AHS антибиотики рекомендацDocument42 pagesAHS антибиотики рекомендацMaksym DemianchukNo ratings yet
- Guideline 133FM PDFDocument13 pagesGuideline 133FM PDFPangestu DhikaNo ratings yet
- Icu Antibiotic GuidelinesDocument4 pagesIcu Antibiotic GuidelinesTia MonitaNo ratings yet
- Empiric Antimicrobial Agent Selection For Acute Complicated UTI - UpToDate 2Document1 pageEmpiric Antimicrobial Agent Selection For Acute Complicated UTI - UpToDate 2Wong Lee CheeNo ratings yet
- Pocket Guide June2013 PDFDocument2 pagesPocket Guide June2013 PDFSergeyGruntov100% (1)
- Antibiotic PolicyDocument10 pagesAntibiotic Policykrutarth shahNo ratings yet
- Peptic Ulcer Disease DrugsDocument6 pagesPeptic Ulcer Disease DrugsApple MaeNo ratings yet
- Antimicrobial Dosage Adjustments in Renal Impairment For FormularyDocument20 pagesAntimicrobial Dosage Adjustments in Renal Impairment For Formularyangkatanjuli2019No ratings yet
- RBCH - PHT Aminophylline Loading Dose GuidelinesDocument2 pagesRBCH - PHT Aminophylline Loading Dose GuidelinesAdrian PrasetioNo ratings yet
- Wound Infections: Common PathogensDocument1 pageWound Infections: Common PathogensAnonymous KGxzow5zxhNo ratings yet
- Postpartum Preeclampsia Checklist: SafemotherhoodinitiativeDocument1 pagePostpartum Preeclampsia Checklist: SafemotherhoodinitiativeazimaNo ratings yet
- Perioperative Antimicrobial Prophylaxis Guidelines For Adult and Pediatric PatientsDocument2 pagesPerioperative Antimicrobial Prophylaxis Guidelines For Adult and Pediatric Patientsihtisham1No ratings yet
- SQC ABx Guidelines 2-21-2011 PDFDocument2 pagesSQC ABx Guidelines 2-21-2011 PDFMinh SteveNo ratings yet
- Acute Pyelonephritis Treatment & Management: Approach ConsiderationsDocument4 pagesAcute Pyelonephritis Treatment & Management: Approach ConsiderationsPeter InocandoNo ratings yet
- Management of Convulsions in Pregnancy 3Document29 pagesManagement of Convulsions in Pregnancy 3Monisha ArulalanNo ratings yet
- Antibiotic Policy 2014Document32 pagesAntibiotic Policy 2014shah007zaad100% (1)
- SHC Antimicrobial Prophylaxis in Surgery RecommendationsDocument3 pagesSHC Antimicrobial Prophylaxis in Surgery RecommendationsCatherine MorrisNo ratings yet
- Antibiotic RegimetotreatpneumoniaDocument1 pageAntibiotic RegimetotreatpneumoniaNousheen ThakurNo ratings yet
- Treatment of MalariaDocument49 pagesTreatment of MalariaShanza AmaanNo ratings yet
- 03 SMI Eclampsia Checklist July 2017Document1 page03 SMI Eclampsia Checklist July 2017piano543100% (1)
- Acs 2023 Part 4 Presentation VersionDocument38 pagesAcs 2023 Part 4 Presentation Versionapi-668470097No ratings yet
- Pneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Document2 pagesPneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Irsalina TriastutikNo ratings yet
- Antibiotic ProphylaxisDocument2 pagesAntibiotic Prophylaxisabdelhamed aliNo ratings yet
- Convulsive Status Epilepticus 1003Document9 pagesConvulsive Status Epilepticus 1003aamir6312No ratings yet
- 19sm02a170703EclampsiaCheck1 PDFDocument1 page19sm02a170703EclampsiaCheck1 PDFazimaNo ratings yet
- Postpartum Preeclampsia Checklist: Emergency Department ExampleDocument1 pagePostpartum Preeclampsia Checklist: Emergency Department ExamplewijeNo ratings yet
- Antibiotic Surgical Prophylaxis Protocol SMH October 2018 UpdateDocument7 pagesAntibiotic Surgical Prophylaxis Protocol SMH October 2018 Updatessrnew2023No ratings yet
- Antibiotic Prophylaxis in Gustilo Grade I To III Open Fractures of The Lower LimbV5 - April18th2012Document1 pageAntibiotic Prophylaxis in Gustilo Grade I To III Open Fractures of The Lower LimbV5 - April18th2012Yopi ArdhiaswariNo ratings yet
- Clinically Significant Drug InteractionsDocument18 pagesClinically Significant Drug Interactionsmagus davilaNo ratings yet
- G HDPDocument32 pagesG HDPkunkkonkNo ratings yet
- Nursing Orientation Program Intravenous TherapyDocument45 pagesNursing Orientation Program Intravenous TherapyMarianne LayloNo ratings yet
- Sucralfate Monograph For ProfessionalsDocument7 pagesSucralfate Monograph For ProfessionalsKP MukherjeeNo ratings yet
- Piperacillin TazobactamDocument1 pagePiperacillin TazobactamRakesh DudiNo ratings yet
- Hypoglycemia Grid Draft 2-17-2016Document1 pageHypoglycemia Grid Draft 2-17-2016Ahmed AbdalfattahNo ratings yet
- Carboplatin PaclitaxelDocument6 pagesCarboplatin PaclitaxelNida Auliya RahmahNo ratings yet
- 8 Convulsions ETAT - 2010Document22 pages8 Convulsions ETAT - 2010nasibdinNo ratings yet
- SHC SurgProphylaxisGuidelinesDocument6 pagesSHC SurgProphylaxisGuidelinesDr shehwar100% (1)
- Bacterial Meningitis HSV Encephalitis: Therapeutic Guidelines AntibioticDocument2 pagesBacterial Meningitis HSV Encephalitis: Therapeutic Guidelines AntibioticBetari DhiraNo ratings yet
- Final Haad (DOH) ExamDocument9 pagesFinal Haad (DOH) ExamsenthamizhselvanNo ratings yet
- Abx Dosing PedsDocument15 pagesAbx Dosing PedsfazalwadoodNo ratings yet
- LifeBridge Health Empiric Antibiotic Guide 2018Document15 pagesLifeBridge Health Empiric Antibiotic Guide 2018passwordNo ratings yet
- Surgical Antibiotic Prophylaxis Guideline 220719Document7 pagesSurgical Antibiotic Prophylaxis Guideline 220719MuathNo ratings yet
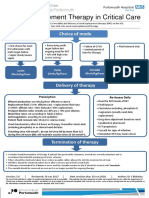
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Commonly Used Premedication Regimens: TaxanesDocument2 pagesCommonly Used Premedication Regimens: TaxanesnurulNo ratings yet
- Protocolo Covid 19 Ihss HRN PDFDocument5 pagesProtocolo Covid 19 Ihss HRN PDFJennifer CarcamoNo ratings yet
- Febrile NeutropeniaDocument3 pagesFebrile Neutropeniatheseus5No ratings yet
- Ciprofloxacin 3Document12 pagesCiprofloxacin 3Odiit StephenNo ratings yet
- Antivirale Covid en No HospitalizadosDocument1 pageAntivirale Covid en No HospitalizadosJORGENo ratings yet
- Adult Sepsis Order SetDocument3 pagesAdult Sepsis Order SetYoussef MokdadNo ratings yet
- 5 Pre Op CS & Major Surgery 22.06.2015Document5 pages5 Pre Op CS & Major Surgery 22.06.2015Mahesh RathnayakeNo ratings yet
- Exp 1 InsertDocument1 pageExp 1 InsertChristianNo ratings yet
- IV To PO Poster VersionDocument1 pageIV To PO Poster VersionJohn Benedict Sta AnaNo ratings yet
- IDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in WomenDocument7 pagesIDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Womenamalia puspita dewiNo ratings yet
- Folfiri Beva Gi Col PDocument12 pagesFolfiri Beva Gi Col Pvera docNo ratings yet
- Flip Chart-Converted 2Document10 pagesFlip Chart-Converted 2anisah mahmudah0% (1)
- Drug StuDyDocument11 pagesDrug StuDyMel SevillaNo ratings yet
- Empiric Antibiotic ListDocument2 pagesEmpiric Antibiotic ListpasswordNo ratings yet
- IDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in WomenDocument6 pagesIDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in WomenIcewizard EugeoNo ratings yet
- The Essential Guide to Ciprofloxacin: Usage, Precautions, Interactions and Side Effects.From EverandThe Essential Guide to Ciprofloxacin: Usage, Precautions, Interactions and Side Effects.No ratings yet
- 44-45 Tetracyclines and Chloramphenicols-2023Document30 pages44-45 Tetracyclines and Chloramphenicols-2023deo okiaNo ratings yet
- Antibiotika PDFDocument101 pagesAntibiotika PDFDaniel SitungkirNo ratings yet
- IMCI Technical Update - Including ZNDocument45 pagesIMCI Technical Update - Including ZNTinnie :)No ratings yet
- Antibiotics and Antibacterial Drugs SDocument67 pagesAntibiotics and Antibacterial Drugs Somar hameed100% (1)
- A Study On The Bacteriological Profile of Urinary PDFDocument4 pagesA Study On The Bacteriological Profile of Urinary PDFcendy oktariNo ratings yet
- Rekap Laporan Lab 2021Document1,925 pagesRekap Laporan Lab 2021fennyrahmaNo ratings yet
- API Experiences Growth: Prime For Perfect MakeupDocument2 pagesAPI Experiences Growth: Prime For Perfect Makeupapi-139438053No ratings yet
- Drug Dosage Mechanism of Action Indications & Contraindications Side Effects & Adverse Effects Nursing ResponsibilityDocument1 pageDrug Dosage Mechanism of Action Indications & Contraindications Side Effects & Adverse Effects Nursing ResponsibilityAthena SaturdayNo ratings yet
- Antibiotics and The Burn Patient: ReviewDocument11 pagesAntibiotics and The Burn Patient: Reviewcirugiaplastica puceNo ratings yet
- The Role of Prebiotics in Pangasius ProductionDocument7 pagesThe Role of Prebiotics in Pangasius ProductionInternational Aquafeed magazine100% (1)
- AntibioticsDocument122 pagesAntibioticsPiyush Verma100% (2)
- Herbs in DentistryDocument6 pagesHerbs in Dentistryinventionjournals100% (1)
- MIDTERM 1 GRAMMAR VOCAB REVISION KeyDocument38 pagesMIDTERM 1 GRAMMAR VOCAB REVISION KeyNicol ManuelaNo ratings yet
- Kenyan HerbsDocument12 pagesKenyan HerbsJoden2005No ratings yet
- FinalDocument39 pagesFinalHazel Trabajo100% (1)
- Antimicrobial Stewardship Program in Hospital - Muchlis AU SofroDocument44 pagesAntimicrobial Stewardship Program in Hospital - Muchlis AU SofroPPI RSPKUMuhCepuNo ratings yet
- Stanford Health Care Antimicrobial Dosing Reference GuideDocument7 pagesStanford Health Care Antimicrobial Dosing Reference GuideKarl Martin PinedaNo ratings yet
- Antibacterial Drug Used in Tretment of Infection of Skin and Soft TissueDocument18 pagesAntibacterial Drug Used in Tretment of Infection of Skin and Soft Tissuerajkumar871992No ratings yet
- Nama Antibiotik Regimen Dosis Dosis Per-Hari Rute No Kode PasienDocument10 pagesNama Antibiotik Regimen Dosis Dosis Per-Hari Rute No Kode PasienAri AnggaraNo ratings yet
- IDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in WomenDocument7 pagesIDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Womenamalia puspita dewiNo ratings yet
- Formulation and Evaluation of Cefuroxime Axetil Orodispensible TabletsDocument10 pagesFormulation and Evaluation of Cefuroxime Axetil Orodispensible TabletsBaru Chandrasekhar RaoNo ratings yet
- Ai AssignmentDocument24 pagesAi AssignmentskmitunNo ratings yet
- Penicillin ReportDocument9 pagesPenicillin ReportJean CabigaoNo ratings yet
- Bioorganic & Medicinal Chemistry Letters XXX (2011) XXX-XXXDocument5 pagesBioorganic & Medicinal Chemistry Letters XXX (2011) XXX-XXXCr PrakashNo ratings yet
- Historical Overview of The Cephalosporin Spectrum: Four Generations of Structural EvolutionDocument8 pagesHistorical Overview of The Cephalosporin Spectrum: Four Generations of Structural EvolutionBagus FitraNo ratings yet
- 5 Psae Egypt 2014Document9 pages5 Psae Egypt 2014Khoa Vi Sinh BVCRNo ratings yet
- Fluoroquinolones PDFDocument1 pageFluoroquinolones PDFmariam ibrahimNo ratings yet
- Presentation FileDocument25 pagesPresentation FileInnoVentureCommunityNo ratings yet
- QR ANTIBIOTIC GUIDELINE A3 Size - 210628 - 082213 - 210628 - 082342 - 210628 - 082357-1Document1 pageQR ANTIBIOTIC GUIDELINE A3 Size - 210628 - 082213 - 210628 - 082342 - 210628 - 082357-1Munirah YusoffNo ratings yet






















































































Download as pdf or txt
You might also like
- Miscellaneous For FinalsDocument30 pagesMiscellaneous For Finalsjames.a.blairNo ratings yet
- Essentials of Internal MedicineDocument832 pagesEssentials of Internal MedicineEmanuelMC100% (79)
- AHS антибиотики рекомендацDocument42 pagesAHS антибиотики рекомендацMaksym DemianchukNo ratings yet
- Guideline 133FM PDFDocument13 pagesGuideline 133FM PDFPangestu DhikaNo ratings yet
- Icu Antibiotic GuidelinesDocument4 pagesIcu Antibiotic GuidelinesTia MonitaNo ratings yet
- Empiric Antimicrobial Agent Selection For Acute Complicated UTI - UpToDate 2Document1 pageEmpiric Antimicrobial Agent Selection For Acute Complicated UTI - UpToDate 2Wong Lee CheeNo ratings yet
- Pocket Guide June2013 PDFDocument2 pagesPocket Guide June2013 PDFSergeyGruntov100% (1)
- Antibiotic PolicyDocument10 pagesAntibiotic Policykrutarth shahNo ratings yet
- Peptic Ulcer Disease DrugsDocument6 pagesPeptic Ulcer Disease DrugsApple MaeNo ratings yet
- Antimicrobial Dosage Adjustments in Renal Impairment For FormularyDocument20 pagesAntimicrobial Dosage Adjustments in Renal Impairment For Formularyangkatanjuli2019No ratings yet
- RBCH - PHT Aminophylline Loading Dose GuidelinesDocument2 pagesRBCH - PHT Aminophylline Loading Dose GuidelinesAdrian PrasetioNo ratings yet
- Wound Infections: Common PathogensDocument1 pageWound Infections: Common PathogensAnonymous KGxzow5zxhNo ratings yet
- Postpartum Preeclampsia Checklist: SafemotherhoodinitiativeDocument1 pagePostpartum Preeclampsia Checklist: SafemotherhoodinitiativeazimaNo ratings yet
- Perioperative Antimicrobial Prophylaxis Guidelines For Adult and Pediatric PatientsDocument2 pagesPerioperative Antimicrobial Prophylaxis Guidelines For Adult and Pediatric Patientsihtisham1No ratings yet
- SQC ABx Guidelines 2-21-2011 PDFDocument2 pagesSQC ABx Guidelines 2-21-2011 PDFMinh SteveNo ratings yet
- Acute Pyelonephritis Treatment & Management: Approach ConsiderationsDocument4 pagesAcute Pyelonephritis Treatment & Management: Approach ConsiderationsPeter InocandoNo ratings yet
- Management of Convulsions in Pregnancy 3Document29 pagesManagement of Convulsions in Pregnancy 3Monisha ArulalanNo ratings yet
- Antibiotic Policy 2014Document32 pagesAntibiotic Policy 2014shah007zaad100% (1)
- SHC Antimicrobial Prophylaxis in Surgery RecommendationsDocument3 pagesSHC Antimicrobial Prophylaxis in Surgery RecommendationsCatherine MorrisNo ratings yet
- Antibiotic RegimetotreatpneumoniaDocument1 pageAntibiotic RegimetotreatpneumoniaNousheen ThakurNo ratings yet
- Treatment of MalariaDocument49 pagesTreatment of MalariaShanza AmaanNo ratings yet
- 03 SMI Eclampsia Checklist July 2017Document1 page03 SMI Eclampsia Checklist July 2017piano543100% (1)
- Acs 2023 Part 4 Presentation VersionDocument38 pagesAcs 2023 Part 4 Presentation Versionapi-668470097No ratings yet
- Pneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Document2 pagesPneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Irsalina TriastutikNo ratings yet
- Antibiotic ProphylaxisDocument2 pagesAntibiotic Prophylaxisabdelhamed aliNo ratings yet
- Convulsive Status Epilepticus 1003Document9 pagesConvulsive Status Epilepticus 1003aamir6312No ratings yet
- 19sm02a170703EclampsiaCheck1 PDFDocument1 page19sm02a170703EclampsiaCheck1 PDFazimaNo ratings yet
- Postpartum Preeclampsia Checklist: Emergency Department ExampleDocument1 pagePostpartum Preeclampsia Checklist: Emergency Department ExamplewijeNo ratings yet
- Antibiotic Surgical Prophylaxis Protocol SMH October 2018 UpdateDocument7 pagesAntibiotic Surgical Prophylaxis Protocol SMH October 2018 Updatessrnew2023No ratings yet
- Antibiotic Prophylaxis in Gustilo Grade I To III Open Fractures of The Lower LimbV5 - April18th2012Document1 pageAntibiotic Prophylaxis in Gustilo Grade I To III Open Fractures of The Lower LimbV5 - April18th2012Yopi ArdhiaswariNo ratings yet
- Clinically Significant Drug InteractionsDocument18 pagesClinically Significant Drug Interactionsmagus davilaNo ratings yet
- G HDPDocument32 pagesG HDPkunkkonkNo ratings yet
- Nursing Orientation Program Intravenous TherapyDocument45 pagesNursing Orientation Program Intravenous TherapyMarianne LayloNo ratings yet
- Sucralfate Monograph For ProfessionalsDocument7 pagesSucralfate Monograph For ProfessionalsKP MukherjeeNo ratings yet
- Piperacillin TazobactamDocument1 pagePiperacillin TazobactamRakesh DudiNo ratings yet
- Hypoglycemia Grid Draft 2-17-2016Document1 pageHypoglycemia Grid Draft 2-17-2016Ahmed AbdalfattahNo ratings yet
- Carboplatin PaclitaxelDocument6 pagesCarboplatin PaclitaxelNida Auliya RahmahNo ratings yet
- 8 Convulsions ETAT - 2010Document22 pages8 Convulsions ETAT - 2010nasibdinNo ratings yet
- SHC SurgProphylaxisGuidelinesDocument6 pagesSHC SurgProphylaxisGuidelinesDr shehwar100% (1)
- Bacterial Meningitis HSV Encephalitis: Therapeutic Guidelines AntibioticDocument2 pagesBacterial Meningitis HSV Encephalitis: Therapeutic Guidelines AntibioticBetari DhiraNo ratings yet
- Final Haad (DOH) ExamDocument9 pagesFinal Haad (DOH) ExamsenthamizhselvanNo ratings yet
- Abx Dosing PedsDocument15 pagesAbx Dosing PedsfazalwadoodNo ratings yet
- LifeBridge Health Empiric Antibiotic Guide 2018Document15 pagesLifeBridge Health Empiric Antibiotic Guide 2018passwordNo ratings yet
- Surgical Antibiotic Prophylaxis Guideline 220719Document7 pagesSurgical Antibiotic Prophylaxis Guideline 220719MuathNo ratings yet
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Commonly Used Premedication Regimens: TaxanesDocument2 pagesCommonly Used Premedication Regimens: TaxanesnurulNo ratings yet
- Protocolo Covid 19 Ihss HRN PDFDocument5 pagesProtocolo Covid 19 Ihss HRN PDFJennifer CarcamoNo ratings yet
- Febrile NeutropeniaDocument3 pagesFebrile Neutropeniatheseus5No ratings yet
- Ciprofloxacin 3Document12 pagesCiprofloxacin 3Odiit StephenNo ratings yet
- Antivirale Covid en No HospitalizadosDocument1 pageAntivirale Covid en No HospitalizadosJORGENo ratings yet
- Adult Sepsis Order SetDocument3 pagesAdult Sepsis Order SetYoussef MokdadNo ratings yet
- 5 Pre Op CS & Major Surgery 22.06.2015Document5 pages5 Pre Op CS & Major Surgery 22.06.2015Mahesh RathnayakeNo ratings yet
- Exp 1 InsertDocument1 pageExp 1 InsertChristianNo ratings yet
- IV To PO Poster VersionDocument1 pageIV To PO Poster VersionJohn Benedict Sta AnaNo ratings yet
- IDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in WomenDocument7 pagesIDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Womenamalia puspita dewiNo ratings yet
- Folfiri Beva Gi Col PDocument12 pagesFolfiri Beva Gi Col Pvera docNo ratings yet
- Flip Chart-Converted 2Document10 pagesFlip Chart-Converted 2anisah mahmudah0% (1)
- Drug StuDyDocument11 pagesDrug StuDyMel SevillaNo ratings yet
- Empiric Antibiotic ListDocument2 pagesEmpiric Antibiotic ListpasswordNo ratings yet
- IDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in WomenDocument6 pagesIDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in WomenIcewizard EugeoNo ratings yet
- The Essential Guide to Ciprofloxacin: Usage, Precautions, Interactions and Side Effects.From EverandThe Essential Guide to Ciprofloxacin: Usage, Precautions, Interactions and Side Effects.No ratings yet
- 44-45 Tetracyclines and Chloramphenicols-2023Document30 pages44-45 Tetracyclines and Chloramphenicols-2023deo okiaNo ratings yet
- Antibiotika PDFDocument101 pagesAntibiotika PDFDaniel SitungkirNo ratings yet
- IMCI Technical Update - Including ZNDocument45 pagesIMCI Technical Update - Including ZNTinnie :)No ratings yet
- Antibiotics and Antibacterial Drugs SDocument67 pagesAntibiotics and Antibacterial Drugs Somar hameed100% (1)
- A Study On The Bacteriological Profile of Urinary PDFDocument4 pagesA Study On The Bacteriological Profile of Urinary PDFcendy oktariNo ratings yet
- Rekap Laporan Lab 2021Document1,925 pagesRekap Laporan Lab 2021fennyrahmaNo ratings yet
- API Experiences Growth: Prime For Perfect MakeupDocument2 pagesAPI Experiences Growth: Prime For Perfect Makeupapi-139438053No ratings yet
- Drug Dosage Mechanism of Action Indications & Contraindications Side Effects & Adverse Effects Nursing ResponsibilityDocument1 pageDrug Dosage Mechanism of Action Indications & Contraindications Side Effects & Adverse Effects Nursing ResponsibilityAthena SaturdayNo ratings yet
- Antibiotics and The Burn Patient: ReviewDocument11 pagesAntibiotics and The Burn Patient: Reviewcirugiaplastica puceNo ratings yet
- The Role of Prebiotics in Pangasius ProductionDocument7 pagesThe Role of Prebiotics in Pangasius ProductionInternational Aquafeed magazine100% (1)
- AntibioticsDocument122 pagesAntibioticsPiyush Verma100% (2)
- Herbs in DentistryDocument6 pagesHerbs in Dentistryinventionjournals100% (1)
- MIDTERM 1 GRAMMAR VOCAB REVISION KeyDocument38 pagesMIDTERM 1 GRAMMAR VOCAB REVISION KeyNicol ManuelaNo ratings yet
- Kenyan HerbsDocument12 pagesKenyan HerbsJoden2005No ratings yet
- FinalDocument39 pagesFinalHazel Trabajo100% (1)
- Antimicrobial Stewardship Program in Hospital - Muchlis AU SofroDocument44 pagesAntimicrobial Stewardship Program in Hospital - Muchlis AU SofroPPI RSPKUMuhCepuNo ratings yet
- Stanford Health Care Antimicrobial Dosing Reference GuideDocument7 pagesStanford Health Care Antimicrobial Dosing Reference GuideKarl Martin PinedaNo ratings yet
- Antibacterial Drug Used in Tretment of Infection of Skin and Soft TissueDocument18 pagesAntibacterial Drug Used in Tretment of Infection of Skin and Soft Tissuerajkumar871992No ratings yet
- Nama Antibiotik Regimen Dosis Dosis Per-Hari Rute No Kode PasienDocument10 pagesNama Antibiotik Regimen Dosis Dosis Per-Hari Rute No Kode PasienAri AnggaraNo ratings yet
- IDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in WomenDocument7 pagesIDSA - Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Womenamalia puspita dewiNo ratings yet
- Formulation and Evaluation of Cefuroxime Axetil Orodispensible TabletsDocument10 pagesFormulation and Evaluation of Cefuroxime Axetil Orodispensible TabletsBaru Chandrasekhar RaoNo ratings yet
- Ai AssignmentDocument24 pagesAi AssignmentskmitunNo ratings yet
- Penicillin ReportDocument9 pagesPenicillin ReportJean CabigaoNo ratings yet
- Bioorganic & Medicinal Chemistry Letters XXX (2011) XXX-XXXDocument5 pagesBioorganic & Medicinal Chemistry Letters XXX (2011) XXX-XXXCr PrakashNo ratings yet
- Historical Overview of The Cephalosporin Spectrum: Four Generations of Structural EvolutionDocument8 pagesHistorical Overview of The Cephalosporin Spectrum: Four Generations of Structural EvolutionBagus FitraNo ratings yet
- 5 Psae Egypt 2014Document9 pages5 Psae Egypt 2014Khoa Vi Sinh BVCRNo ratings yet
- Fluoroquinolones PDFDocument1 pageFluoroquinolones PDFmariam ibrahimNo ratings yet
- Presentation FileDocument25 pagesPresentation FileInnoVentureCommunityNo ratings yet
- QR ANTIBIOTIC GUIDELINE A3 Size - 210628 - 082213 - 210628 - 082342 - 210628 - 082357-1Document1 pageQR ANTIBIOTIC GUIDELINE A3 Size - 210628 - 082213 - 210628 - 082342 - 210628 - 082357-1Munirah YusoffNo ratings yet