
Yoga Yuniadi - Wide QRS Complex Tachycardia - Baru
Yoga Yuniadi - Wide QRS Complex Tachycardia - Baru
You might also like
- British-Airways e A4Document14 pagesBritish-Airways e A4Samuel Lim70% (10)
- ECG InterpretationDocument95 pagesECG InterpretationNur Rahmat Wibowo100% (10)
- Cardiology Ekg BoardDocument87 pagesCardiology Ekg BoardPutri WijayaNo ratings yet
- Wide QRS Complex TachyarrhythmiaDocument36 pagesWide QRS Complex TachyarrhythmiaMaruliNo ratings yet
- Approach To A Wide Complex Tachycardia: DR - Maksud D-CARD Student Dhaka Medical CollegeDocument51 pagesApproach To A Wide Complex Tachycardia: DR - Maksud D-CARD Student Dhaka Medical CollegerusmanshiddiqNo ratings yet
- Broad Complex TachycardiaDocument63 pagesBroad Complex Tachycardiadragon66No ratings yet
- All About EcgDocument92 pagesAll About Ecgezhilmathimbbs_21630No ratings yet
- Differential Diagnosis of Wide QRS TachycardiasDocument6 pagesDifferential Diagnosis of Wide QRS TachycardiasKev Jose Ruiz RojasNo ratings yet
- PG - Quick Look On Arrhythmia in ED - JCU 2021Document71 pagesPG - Quick Look On Arrhythmia in ED - JCU 2021Afied FitrahNo ratings yet
- Basics and Interpretation: Sif HansdottirDocument65 pagesBasics and Interpretation: Sif Hansdottirwenny1186100% (1)
- VT Vs SVT AberrantDocument41 pagesVT Vs SVT AberrantAl Hijjah FadhilahNo ratings yet
- VT Versus SVT (With Aberrancy) : Adapted From, 2019Document10 pagesVT Versus SVT (With Aberrancy) : Adapted From, 2019wddassdaNo ratings yet
- Paul Varosy - ECG Criteria For Distinguishing SVT From VTDocument9 pagesPaul Varosy - ECG Criteria For Distinguishing SVT From VTTriple-mNo ratings yet
- ArrhytmiaDocument70 pagesArrhytmiaAfied FitrahNo ratings yet
- Superimposed ECG PDFDocument93 pagesSuperimposed ECG PDFEdalyn CapiliNo ratings yet
- ElectrocardiogramDocument169 pagesElectrocardiogramjitendra magarNo ratings yet
- Advanced ECG Interpretation: Rebecca Sevigny BSN, RN, CCRNDocument76 pagesAdvanced ECG Interpretation: Rebecca Sevigny BSN, RN, CCRNI Putu SastrawanNo ratings yet
- EKG Taki-Bradi AritmiaDocument47 pagesEKG Taki-Bradi Aritmiamithaa octoviagnesNo ratings yet
- Acc Ecg ChallengeDocument91 pagesAcc Ecg ChallengeMiguel LizarragaNo ratings yet
- EKG Common Clinical ArrhythmiasDocument54 pagesEKG Common Clinical ArrhythmiasFaisal AlhasNo ratings yet
- Basic Ecg From FastlanDocument125 pagesBasic Ecg From Fastlanomarfaruque7807No ratings yet
- The Normal ElectrocardiogramDocument63 pagesThe Normal ElectrocardiogramPuravin Crishan VeerasamyNo ratings yet
- ECG Final Yrs ModifiedDocument69 pagesECG Final Yrs ModifiedSAVIO T ALPHONSENo ratings yet
- Ventricular Tachycardia in The Ischemic HeartDocument57 pagesVentricular Tachycardia in The Ischemic Heartusfcards100% (3)
- Ventricular Arrhythmia - VT: Braghmandaru A.BDocument113 pagesVentricular Arrhythmia - VT: Braghmandaru A.BFaisol SiddiqNo ratings yet
- Kuliah EKG II Unswagati 2016Document77 pagesKuliah EKG II Unswagati 2016iikNo ratings yet
- Widecomplex Tachycardia: Mithilesh Kumar Das,, Archana Rajdev,, Vikas KalraDocument13 pagesWidecomplex Tachycardia: Mithilesh Kumar Das,, Archana Rajdev,, Vikas KalraTor JaNo ratings yet
- Bradi Si Tahi Cu Risc Vital FinalDocument67 pagesBradi Si Tahi Cu Risc Vital FinalAndreeaNo ratings yet
- Tachycardia Which Fast Is Too FuriousDocument79 pagesTachycardia Which Fast Is Too FuriousEstiningtiyas RahayuNo ratings yet
- VT Versus SVTDocument12 pagesVT Versus SVTYuli AzwarNo ratings yet
- All EcgDocument143 pagesAll EcgYenza FaheraNo ratings yet
- QRS Interval - LITFL - ECG Library BasicsDocument10 pagesQRS Interval - LITFL - ECG Library Basicssilver silvaNo ratings yet
- ECG TutorialDocument40 pagesECG TutorialAnonymous HAbhRTs2TfNo ratings yet
- 2 Februari 2018 EKGDocument24 pages2 Februari 2018 EKGDarren WilliamNo ratings yet
- Basics of ECG Pre-Workshop: Dr. Nancy Selfridge Chair, Department of Clinical Medicine Semester 4 2019Document43 pagesBasics of ECG Pre-Workshop: Dr. Nancy Selfridge Chair, Department of Clinical Medicine Semester 4 2019Tom TsouNo ratings yet
- Arrhytmia: Tachyarrhythmia (Rate 100 X/min) Bradyarrhytmia (Rate 60 X/min)Document50 pagesArrhytmia: Tachyarrhythmia (Rate 100 X/min) Bradyarrhytmia (Rate 60 X/min)Rica HermanNo ratings yet
- Ecg Pathology 02Document95 pagesEcg Pathology 02Andi MP Manurung100% (1)
- Topnotch ECG Interpretation For MoonlightersDocument25 pagesTopnotch ECG Interpretation For Moonlightersmefav7778520100% (1)
- Wswecocekgdasar2018Document34 pagesWswecocekgdasar2018Hendra AbeitNo ratings yet
- ECG For InternsDocument31 pagesECG For InternsAgus SyaifudinNo ratings yet
- W-2-Sevigny-Basic ECG PDFDocument61 pagesW-2-Sevigny-Basic ECG PDFdheaNo ratings yet
- Arrythmia Recognition Lecture FinalDocument54 pagesArrythmia Recognition Lecture FinalFlorencio D. Santos IVNo ratings yet
- ECG HandoutsDocument12 pagesECG HandoutsJeffrey RamosNo ratings yet
- How To: Read ECG?Document63 pagesHow To: Read ECG?Let BNo ratings yet
- Electrocardiography: I. Leads A. Limb LeadsDocument11 pagesElectrocardiography: I. Leads A. Limb LeadsJoezelle0% (1)
- Aritmia Dan BradiaritmiaDocument29 pagesAritmia Dan BradiaritmiaNurlina Setiadi100% (1)
- Normal ECGDocument63 pagesNormal ECGMohd Johari Mohd ShafuwanNo ratings yet
- Cardio INTERPRETATION OF THE ELECTROCARDIOGRAMDocument74 pagesCardio INTERPRETATION OF THE ELECTROCARDIOGRAMkrisnoNo ratings yet
- Brugada CriteriaDocument1 pageBrugada CriteriaMarcus PaulNo ratings yet
- Suatu Alat LaboratorisDocument78 pagesSuatu Alat LaboratorisHematology 2016No ratings yet
- Cardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyDocument87 pagesCardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyummimalikihamidNo ratings yet
- EKG Curs Asistenti Medicali GeneralistriDocument18 pagesEKG Curs Asistenti Medicali GeneralistriDiana IoanaNo ratings yet
- 0 Arrhythmia Arwin PDFDocument53 pages0 Arrhythmia Arwin PDFEvans HansenNo ratings yet
- Ecg Interpretation:: The BasicsDocument40 pagesEcg Interpretation:: The BasicsRavi SharmaNo ratings yet
- Basics of ECG: By-Pallavi ChicholikarDocument115 pagesBasics of ECG: By-Pallavi ChicholikarBhakti WashilkarNo ratings yet
- Abnormal ECG L 3 chamber enlargement and blockDocument34 pagesAbnormal ECG L 3 chamber enlargement and blockعلي عليNo ratings yet
- EKG Interpretation Lecture 1 - Identifying The Squiggles, Developing A System For ReadingDocument6 pagesEKG Interpretation Lecture 1 - Identifying The Squiggles, Developing A System For Readingkcargen100% (1)
- KULIAH ECG Dinkes PurworejoDocument69 pagesKULIAH ECG Dinkes PurworejoVella NurfatimahNo ratings yet
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachFrom EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachNo ratings yet
- Raharjo SB - 2018 - Conventional AblationDocument37 pagesRaharjo SB - 2018 - Conventional AblationZulhelmiNo ratings yet
- Dicky A. Hanafy - Indication and Choice of Remote Monitoring EPDocument31 pagesDicky A. Hanafy - Indication and Choice of Remote Monitoring EPZulhelmiNo ratings yet
- Dony Yugo - Ablation HOCMDocument21 pagesDony Yugo - Ablation HOCMZulhelmiNo ratings yet
- Dony Yugo - Drug Provocative TestDocument21 pagesDony Yugo - Drug Provocative TestZulhelmiNo ratings yet
- HRV Twa EpDocument54 pagesHRV Twa EpZulhelmiNo ratings yet
- Raharjo SB - Opening EP BootcampDocument16 pagesRaharjo SB - Opening EP BootcampZulhelmiNo ratings yet
- Yoga Yuniadi - Ladder DiagramDocument32 pagesYoga Yuniadi - Ladder DiagramZulhelmiNo ratings yet
- Aleka EpDocument67 pagesAleka EpZulhelmiNo ratings yet
- Raharjo SB - 2018 - LAA ClosureDocument26 pagesRaharjo SB - 2018 - LAA ClosureZulhelmiNo ratings yet
- TB-HIV Private PhysiciansDocument66 pagesTB-HIV Private PhysiciansZulhelmiNo ratings yet
- Surface & Coatings Technology: J. VetterDocument28 pagesSurface & Coatings Technology: J. VetterAlireza BagherpourNo ratings yet
- Induced OmanDocument295 pagesInduced OmanWaleed EjazNo ratings yet
- Application of Capital Structure Theories. A Systematic ReviewDocument27 pagesApplication of Capital Structure Theories. A Systematic ReviewAhmed BakhtNo ratings yet
- Comptia A+ 220-601 Practice Test QuestionsDocument32 pagesComptia A+ 220-601 Practice Test Questionsmidnight sun fanNo ratings yet
- Using An Online Auction System in Open Source PDFDocument8 pagesUsing An Online Auction System in Open Source PDFRachmat Aulia0% (1)
- Fundamentals of Computer GraphicsDocument58 pagesFundamentals of Computer GraphicsISHAAN TAKKARNo ratings yet
- INSTOCK IPAS EDI InstructionDocument27 pagesINSTOCK IPAS EDI InstructionFei XueNo ratings yet
- Basic Dimensions For NPT American National Taper Pipe ThreadsDocument2 pagesBasic Dimensions For NPT American National Taper Pipe ThreadsAndi DumayNo ratings yet
- 4 Stoichiometry PDFDocument8 pages4 Stoichiometry PDFHakim Abbas Ali PhalasiyaNo ratings yet
- Pneumatic Logic ComponentsDocument17 pagesPneumatic Logic ComponentskammoNo ratings yet
- Ce 023 Module 5 and 6Document9 pagesCe 023 Module 5 and 6George YanelaNo ratings yet
- Generic - MCQ - Answer - Sheet (1) IB ExamDocument2 pagesGeneric - MCQ - Answer - Sheet (1) IB ExamKB CochraneNo ratings yet
- TADANO Gr300ex3Document157 pagesTADANO Gr300ex3Abi Jith100% (1)
- TheProfessionalNurseSelf AssessmentScaleDocument14 pagesTheProfessionalNurseSelf AssessmentScaleNabeeha Fazeel100% (1)
- Linde C-Matic AutobonicsDocument6 pagesLinde C-Matic AutobonicsJONHHY NGUYEN DANGNo ratings yet
- Read MeDocument1 pageRead MeDileep MishraNo ratings yet
- Syed Ahsan Ali Bokhari (11-MS-TE-15) Muhammad Usman Ghani (11-MS-CP-07) Shariq Rafiq Khan (11-MS-TE-13) Rao Taimoor Ali (10-IEMS-EM-29)Document19 pagesSyed Ahsan Ali Bokhari (11-MS-TE-15) Muhammad Usman Ghani (11-MS-CP-07) Shariq Rafiq Khan (11-MS-TE-13) Rao Taimoor Ali (10-IEMS-EM-29)Syed Ahsan Ali BokhariNo ratings yet
- Image Enhancement-Spatial Domain - UpdatedDocument112 pagesImage Enhancement-Spatial Domain - Updatedzain javaidNo ratings yet
- Weight of CalculationDocument5 pagesWeight of Calculationlitaanggita fordesignNo ratings yet
- O o o o o o o o o o oDocument17 pagesO o o o o o o o o o oshukkurNo ratings yet
- Campbell Dudek Smith 1970Document10 pagesCampbell Dudek Smith 1970richardvas12No ratings yet
- 02 ExplorationDocument50 pages02 ExplorationYernar TiyntayevNo ratings yet
- Fall 2010-11 Course OfferingsDocument3 pagesFall 2010-11 Course OfferingsrezadigitNo ratings yet
- Lesson Plan in Science 7Document6 pagesLesson Plan in Science 7gemima galvezNo ratings yet
- FDocument4 pagesFYoniwo Edward TsemiNo ratings yet
- Capitulos GuiaDocument100 pagesCapitulos GuiaRicardo ValverdeNo ratings yet
- FRWTMCver413eng PDFDocument168 pagesFRWTMCver413eng PDFdrakula85100% (1)
- Midland Brick Coursing ChartDocument2 pagesMidland Brick Coursing ChartMichael Slater100% (1)
- Business Applications - FractionsDocument1 pageBusiness Applications - FractionsShiny NatividadNo ratings yet


































































































Download as pdf or txt
You might also like
- British-Airways e A4Document14 pagesBritish-Airways e A4Samuel Lim70% (10)
- ECG InterpretationDocument95 pagesECG InterpretationNur Rahmat Wibowo100% (10)
- Cardiology Ekg BoardDocument87 pagesCardiology Ekg BoardPutri WijayaNo ratings yet
- Wide QRS Complex TachyarrhythmiaDocument36 pagesWide QRS Complex TachyarrhythmiaMaruliNo ratings yet
- Approach To A Wide Complex Tachycardia: DR - Maksud D-CARD Student Dhaka Medical CollegeDocument51 pagesApproach To A Wide Complex Tachycardia: DR - Maksud D-CARD Student Dhaka Medical CollegerusmanshiddiqNo ratings yet
- Broad Complex TachycardiaDocument63 pagesBroad Complex Tachycardiadragon66No ratings yet
- All About EcgDocument92 pagesAll About Ecgezhilmathimbbs_21630No ratings yet
- Differential Diagnosis of Wide QRS TachycardiasDocument6 pagesDifferential Diagnosis of Wide QRS TachycardiasKev Jose Ruiz RojasNo ratings yet
- PG - Quick Look On Arrhythmia in ED - JCU 2021Document71 pagesPG - Quick Look On Arrhythmia in ED - JCU 2021Afied FitrahNo ratings yet
- Basics and Interpretation: Sif HansdottirDocument65 pagesBasics and Interpretation: Sif Hansdottirwenny1186100% (1)
- VT Vs SVT AberrantDocument41 pagesVT Vs SVT AberrantAl Hijjah FadhilahNo ratings yet
- VT Versus SVT (With Aberrancy) : Adapted From, 2019Document10 pagesVT Versus SVT (With Aberrancy) : Adapted From, 2019wddassdaNo ratings yet
- Paul Varosy - ECG Criteria For Distinguishing SVT From VTDocument9 pagesPaul Varosy - ECG Criteria For Distinguishing SVT From VTTriple-mNo ratings yet
- ArrhytmiaDocument70 pagesArrhytmiaAfied FitrahNo ratings yet
- Superimposed ECG PDFDocument93 pagesSuperimposed ECG PDFEdalyn CapiliNo ratings yet
- ElectrocardiogramDocument169 pagesElectrocardiogramjitendra magarNo ratings yet
- Advanced ECG Interpretation: Rebecca Sevigny BSN, RN, CCRNDocument76 pagesAdvanced ECG Interpretation: Rebecca Sevigny BSN, RN, CCRNI Putu SastrawanNo ratings yet
- EKG Taki-Bradi AritmiaDocument47 pagesEKG Taki-Bradi Aritmiamithaa octoviagnesNo ratings yet
- Acc Ecg ChallengeDocument91 pagesAcc Ecg ChallengeMiguel LizarragaNo ratings yet
- EKG Common Clinical ArrhythmiasDocument54 pagesEKG Common Clinical ArrhythmiasFaisal AlhasNo ratings yet
- Basic Ecg From FastlanDocument125 pagesBasic Ecg From Fastlanomarfaruque7807No ratings yet
- The Normal ElectrocardiogramDocument63 pagesThe Normal ElectrocardiogramPuravin Crishan VeerasamyNo ratings yet
- ECG Final Yrs ModifiedDocument69 pagesECG Final Yrs ModifiedSAVIO T ALPHONSENo ratings yet
- Ventricular Tachycardia in The Ischemic HeartDocument57 pagesVentricular Tachycardia in The Ischemic Heartusfcards100% (3)
- Ventricular Arrhythmia - VT: Braghmandaru A.BDocument113 pagesVentricular Arrhythmia - VT: Braghmandaru A.BFaisol SiddiqNo ratings yet
- Kuliah EKG II Unswagati 2016Document77 pagesKuliah EKG II Unswagati 2016iikNo ratings yet
- Widecomplex Tachycardia: Mithilesh Kumar Das,, Archana Rajdev,, Vikas KalraDocument13 pagesWidecomplex Tachycardia: Mithilesh Kumar Das,, Archana Rajdev,, Vikas KalraTor JaNo ratings yet
- Bradi Si Tahi Cu Risc Vital FinalDocument67 pagesBradi Si Tahi Cu Risc Vital FinalAndreeaNo ratings yet
- Tachycardia Which Fast Is Too FuriousDocument79 pagesTachycardia Which Fast Is Too FuriousEstiningtiyas RahayuNo ratings yet
- VT Versus SVTDocument12 pagesVT Versus SVTYuli AzwarNo ratings yet
- All EcgDocument143 pagesAll EcgYenza FaheraNo ratings yet
- QRS Interval - LITFL - ECG Library BasicsDocument10 pagesQRS Interval - LITFL - ECG Library Basicssilver silvaNo ratings yet
- ECG TutorialDocument40 pagesECG TutorialAnonymous HAbhRTs2TfNo ratings yet
- 2 Februari 2018 EKGDocument24 pages2 Februari 2018 EKGDarren WilliamNo ratings yet
- Basics of ECG Pre-Workshop: Dr. Nancy Selfridge Chair, Department of Clinical Medicine Semester 4 2019Document43 pagesBasics of ECG Pre-Workshop: Dr. Nancy Selfridge Chair, Department of Clinical Medicine Semester 4 2019Tom TsouNo ratings yet
- Arrhytmia: Tachyarrhythmia (Rate 100 X/min) Bradyarrhytmia (Rate 60 X/min)Document50 pagesArrhytmia: Tachyarrhythmia (Rate 100 X/min) Bradyarrhytmia (Rate 60 X/min)Rica HermanNo ratings yet
- Ecg Pathology 02Document95 pagesEcg Pathology 02Andi MP Manurung100% (1)
- Topnotch ECG Interpretation For MoonlightersDocument25 pagesTopnotch ECG Interpretation For Moonlightersmefav7778520100% (1)
- Wswecocekgdasar2018Document34 pagesWswecocekgdasar2018Hendra AbeitNo ratings yet
- ECG For InternsDocument31 pagesECG For InternsAgus SyaifudinNo ratings yet
- W-2-Sevigny-Basic ECG PDFDocument61 pagesW-2-Sevigny-Basic ECG PDFdheaNo ratings yet
- Arrythmia Recognition Lecture FinalDocument54 pagesArrythmia Recognition Lecture FinalFlorencio D. Santos IVNo ratings yet
- ECG HandoutsDocument12 pagesECG HandoutsJeffrey RamosNo ratings yet
- How To: Read ECG?Document63 pagesHow To: Read ECG?Let BNo ratings yet
- Electrocardiography: I. Leads A. Limb LeadsDocument11 pagesElectrocardiography: I. Leads A. Limb LeadsJoezelle0% (1)
- Aritmia Dan BradiaritmiaDocument29 pagesAritmia Dan BradiaritmiaNurlina Setiadi100% (1)
- Normal ECGDocument63 pagesNormal ECGMohd Johari Mohd ShafuwanNo ratings yet
- Cardio INTERPRETATION OF THE ELECTROCARDIOGRAMDocument74 pagesCardio INTERPRETATION OF THE ELECTROCARDIOGRAMkrisnoNo ratings yet
- Brugada CriteriaDocument1 pageBrugada CriteriaMarcus PaulNo ratings yet
- Suatu Alat LaboratorisDocument78 pagesSuatu Alat LaboratorisHematology 2016No ratings yet
- Cardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyDocument87 pagesCardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyummimalikihamidNo ratings yet
- EKG Curs Asistenti Medicali GeneralistriDocument18 pagesEKG Curs Asistenti Medicali GeneralistriDiana IoanaNo ratings yet
- 0 Arrhythmia Arwin PDFDocument53 pages0 Arrhythmia Arwin PDFEvans HansenNo ratings yet
- Ecg Interpretation:: The BasicsDocument40 pagesEcg Interpretation:: The BasicsRavi SharmaNo ratings yet
- Basics of ECG: By-Pallavi ChicholikarDocument115 pagesBasics of ECG: By-Pallavi ChicholikarBhakti WashilkarNo ratings yet
- Abnormal ECG L 3 chamber enlargement and blockDocument34 pagesAbnormal ECG L 3 chamber enlargement and blockعلي عليNo ratings yet
- EKG Interpretation Lecture 1 - Identifying The Squiggles, Developing A System For ReadingDocument6 pagesEKG Interpretation Lecture 1 - Identifying The Squiggles, Developing A System For Readingkcargen100% (1)
- KULIAH ECG Dinkes PurworejoDocument69 pagesKULIAH ECG Dinkes PurworejoVella NurfatimahNo ratings yet
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachFrom EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachNo ratings yet
- Raharjo SB - 2018 - Conventional AblationDocument37 pagesRaharjo SB - 2018 - Conventional AblationZulhelmiNo ratings yet
- Dicky A. Hanafy - Indication and Choice of Remote Monitoring EPDocument31 pagesDicky A. Hanafy - Indication and Choice of Remote Monitoring EPZulhelmiNo ratings yet
- Dony Yugo - Ablation HOCMDocument21 pagesDony Yugo - Ablation HOCMZulhelmiNo ratings yet
- Dony Yugo - Drug Provocative TestDocument21 pagesDony Yugo - Drug Provocative TestZulhelmiNo ratings yet
- HRV Twa EpDocument54 pagesHRV Twa EpZulhelmiNo ratings yet
- Raharjo SB - Opening EP BootcampDocument16 pagesRaharjo SB - Opening EP BootcampZulhelmiNo ratings yet
- Yoga Yuniadi - Ladder DiagramDocument32 pagesYoga Yuniadi - Ladder DiagramZulhelmiNo ratings yet
- Aleka EpDocument67 pagesAleka EpZulhelmiNo ratings yet
- Raharjo SB - 2018 - LAA ClosureDocument26 pagesRaharjo SB - 2018 - LAA ClosureZulhelmiNo ratings yet
- TB-HIV Private PhysiciansDocument66 pagesTB-HIV Private PhysiciansZulhelmiNo ratings yet
- Surface & Coatings Technology: J. VetterDocument28 pagesSurface & Coatings Technology: J. VetterAlireza BagherpourNo ratings yet
- Induced OmanDocument295 pagesInduced OmanWaleed EjazNo ratings yet
- Application of Capital Structure Theories. A Systematic ReviewDocument27 pagesApplication of Capital Structure Theories. A Systematic ReviewAhmed BakhtNo ratings yet
- Comptia A+ 220-601 Practice Test QuestionsDocument32 pagesComptia A+ 220-601 Practice Test Questionsmidnight sun fanNo ratings yet
- Using An Online Auction System in Open Source PDFDocument8 pagesUsing An Online Auction System in Open Source PDFRachmat Aulia0% (1)
- Fundamentals of Computer GraphicsDocument58 pagesFundamentals of Computer GraphicsISHAAN TAKKARNo ratings yet
- INSTOCK IPAS EDI InstructionDocument27 pagesINSTOCK IPAS EDI InstructionFei XueNo ratings yet
- Basic Dimensions For NPT American National Taper Pipe ThreadsDocument2 pagesBasic Dimensions For NPT American National Taper Pipe ThreadsAndi DumayNo ratings yet
- 4 Stoichiometry PDFDocument8 pages4 Stoichiometry PDFHakim Abbas Ali PhalasiyaNo ratings yet
- Pneumatic Logic ComponentsDocument17 pagesPneumatic Logic ComponentskammoNo ratings yet
- Ce 023 Module 5 and 6Document9 pagesCe 023 Module 5 and 6George YanelaNo ratings yet
- Generic - MCQ - Answer - Sheet (1) IB ExamDocument2 pagesGeneric - MCQ - Answer - Sheet (1) IB ExamKB CochraneNo ratings yet
- TADANO Gr300ex3Document157 pagesTADANO Gr300ex3Abi Jith100% (1)
- TheProfessionalNurseSelf AssessmentScaleDocument14 pagesTheProfessionalNurseSelf AssessmentScaleNabeeha Fazeel100% (1)
- Linde C-Matic AutobonicsDocument6 pagesLinde C-Matic AutobonicsJONHHY NGUYEN DANGNo ratings yet
- Read MeDocument1 pageRead MeDileep MishraNo ratings yet
- Syed Ahsan Ali Bokhari (11-MS-TE-15) Muhammad Usman Ghani (11-MS-CP-07) Shariq Rafiq Khan (11-MS-TE-13) Rao Taimoor Ali (10-IEMS-EM-29)Document19 pagesSyed Ahsan Ali Bokhari (11-MS-TE-15) Muhammad Usman Ghani (11-MS-CP-07) Shariq Rafiq Khan (11-MS-TE-13) Rao Taimoor Ali (10-IEMS-EM-29)Syed Ahsan Ali BokhariNo ratings yet
- Image Enhancement-Spatial Domain - UpdatedDocument112 pagesImage Enhancement-Spatial Domain - Updatedzain javaidNo ratings yet
- Weight of CalculationDocument5 pagesWeight of Calculationlitaanggita fordesignNo ratings yet
- O o o o o o o o o o oDocument17 pagesO o o o o o o o o o oshukkurNo ratings yet
- Campbell Dudek Smith 1970Document10 pagesCampbell Dudek Smith 1970richardvas12No ratings yet
- 02 ExplorationDocument50 pages02 ExplorationYernar TiyntayevNo ratings yet
- Fall 2010-11 Course OfferingsDocument3 pagesFall 2010-11 Course OfferingsrezadigitNo ratings yet
- Lesson Plan in Science 7Document6 pagesLesson Plan in Science 7gemima galvezNo ratings yet
- FDocument4 pagesFYoniwo Edward TsemiNo ratings yet
- Capitulos GuiaDocument100 pagesCapitulos GuiaRicardo ValverdeNo ratings yet
- FRWTMCver413eng PDFDocument168 pagesFRWTMCver413eng PDFdrakula85100% (1)
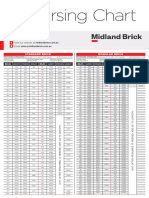
- Midland Brick Coursing ChartDocument2 pagesMidland Brick Coursing ChartMichael Slater100% (1)
- Business Applications - FractionsDocument1 pageBusiness Applications - FractionsShiny NatividadNo ratings yet