Download as docx, pdf, or txt
You might also like
- Trading From Levels of Energy & The Unconscious MindDocument4 pagesTrading From Levels of Energy & The Unconscious MindMandeep Gill100% (4)
- Harry Wong - OutlineDocument15 pagesHarry Wong - OutlineFem Fem100% (1)
- Day 1: The Ultimate Guide To Decoding A Child's Sensory SystemDocument45 pagesDay 1: The Ultimate Guide To Decoding A Child's Sensory SystemLuca ServentiNo ratings yet
- Occt 630 - Occupational Profile and Intervention Plan - PortfolioDocument21 pagesOcct 630 - Occupational Profile and Intervention Plan - Portfolioapi-279916752No ratings yet
- Allen Cogntive Disabilties ModelDocument29 pagesAllen Cogntive Disabilties ModelSarah Lyn White-Cantu100% (1)
- Eng201 Latest Solved Mcqs by Reference From Mid Term PapersDocument13 pagesEng201 Latest Solved Mcqs by Reference From Mid Term Papersbani100% (4)
- Dreams Are The Royal Road To The UnconsciousDocument22 pagesDreams Are The Royal Road To The Unconsciousahmadmedo100% (1)
- Court Ordered DBT ClearanceDocument4 pagesCourt Ordered DBT ClearanceLori HandrahanNo ratings yet
- Guidelines For Documentation of Occupational Therapy PDFDocument7 pagesGuidelines For Documentation of Occupational Therapy PDFMaria AiramNo ratings yet
- Therapy Outcome Measures for Rehabilitation Professionals: Speech and Language Therapy, Physiotherapy, Occupational TherapyFrom EverandTherapy Outcome Measures for Rehabilitation Professionals: Speech and Language Therapy, Physiotherapy, Occupational TherapyNo ratings yet
- The Efficacy of Sensory Integration Therapy On Children With Asperger's Syndrome and Pdd-NosDocument278 pagesThe Efficacy of Sensory Integration Therapy On Children With Asperger's Syndrome and Pdd-NosAbu FayyadhNo ratings yet
- Sensory Motor Skill DevelopmentDocument3 pagesSensory Motor Skill DevelopmentMagiting FmgNo ratings yet
- Sensory Room Presentation Due 12Document9 pagesSensory Room Presentation Due 12api-582889983No ratings yet
- Key Responsibilities:: Occupational Therapist Job Description V-Jan/2020Document4 pagesKey Responsibilities:: Occupational Therapist Job Description V-Jan/2020MD Luthfy LubisNo ratings yet
- Effectiveness of Sensory Integration Therapy (Vestibular & Proprioception Input) On Gross Motor Functioning in Developmental Delayed and Spastic Diplegic CP ChildrenDocument6 pagesEffectiveness of Sensory Integration Therapy (Vestibular & Proprioception Input) On Gross Motor Functioning in Developmental Delayed and Spastic Diplegic CP ChildrenYanuar Adi SanjayaNo ratings yet
- Wee FimDocument9 pagesWee FimdeffyNo ratings yet
- Objective TipsDocument3 pagesObjective TipsAzure GlyNo ratings yet
- FxwsensorychildDocument31 pagesFxwsensorychildapi-534627445No ratings yet
- Sensory Processing Presentation February 2014Document58 pagesSensory Processing Presentation February 2014Geovanny NuñezNo ratings yet
- Tactile Defensiveness PDFDocument7 pagesTactile Defensiveness PDFCristi BacuNo ratings yet
- OT Interventions For ASDDocument42 pagesOT Interventions For ASDTitus LeeNo ratings yet
- OT in Pediatrics Quick Reference GuideDocument2 pagesOT in Pediatrics Quick Reference GuideMaya JohnsonNo ratings yet
- Treatment PlanDocument6 pagesTreatment Planapi-382628487100% (1)
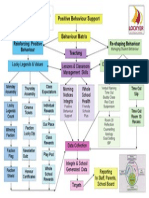
- Positive Behaviour SupportsDocument1 pagePositive Behaviour SupportsCandice BurchNo ratings yet
- Occt 526 - Child-Based PicoDocument14 pagesOcct 526 - Child-Based Picoapi-291380671No ratings yet
- Sensory DevelopmentDocument3 pagesSensory Developmentapi-660820048No ratings yet
- Bethany Case StudyDocument25 pagesBethany Case StudyMegan McCarthyNo ratings yet
- CARESOSA - Research Questions Set 1Document7 pagesCARESOSA - Research Questions Set 1Lucille CaresosaNo ratings yet
- Chapter 16: Application of Motor Control and Motor LearningDocument8 pagesChapter 16: Application of Motor Control and Motor LearningJireh Chambers100% (1)
- MOHO Intervention Implementation - GUADALQUIVERDocument3 pagesMOHO Intervention Implementation - GUADALQUIVERKoyceNo ratings yet
- Zones Student PrequestionnaireDocument1 pageZones Student PrequestionnaireRachelNo ratings yet
- The Performance Quality Rating Scale (PQRS) : Reliability, Convergent Validity, and Internal Responsiveness For Two Scoring SystemsDocument8 pagesThe Performance Quality Rating Scale (PQRS) : Reliability, Convergent Validity, and Internal Responsiveness For Two Scoring SystemsCarol AlvaradoNo ratings yet
- Activity Analysis OutlineDocument3 pagesActivity Analysis OutlineNaomi Apuhin100% (1)
- Pre-Post OT InterventionDocument16 pagesPre-Post OT InterventionIdanerlisNo ratings yet
- Activity Analysis, Creativity and Playfulness in Pediatric Occupational TherapyDocument16 pagesActivity Analysis, Creativity and Playfulness in Pediatric Occupational TherapySofia VieiraNo ratings yet
- Pressure, Temperature, Pain, and Movement of The Hairs On The SkinDocument18 pagesPressure, Temperature, Pain, and Movement of The Hairs On The SkinAnup PednekarNo ratings yet
- Intervention & Goal Update For Annalise (SP Lab) Taylor StamperDocument3 pagesIntervention & Goal Update For Annalise (SP Lab) Taylor Stamperapi-547889945No ratings yet
- Specific Learning DisabilitiesDocument61 pagesSpecific Learning DisabilitiesShallu JoonNo ratings yet
- Cognitive Development For StudentsDocument94 pagesCognitive Development For StudentsaplesgjskNo ratings yet
- Behavior-Checklist StudentReferralLetterDocument4 pagesBehavior-Checklist StudentReferralLetterAna MallariNo ratings yet
- OT For AutismDocument2 pagesOT For AutismArianna Apreutesei3152eri8oawiNo ratings yet
- Developmental ForDocument16 pagesDevelopmental ForAarthi ArumugamNo ratings yet
- COMPANION SP2 TEMPLATE Summary & Interpretation FormDocument5 pagesCOMPANION SP2 TEMPLATE Summary & Interpretation FormjcNo ratings yet
- Occupational Therapy and Life Course Development: A Work Book for Professional PracticeFrom EverandOccupational Therapy and Life Course Development: A Work Book for Professional PracticeNo ratings yet
- WeeFIM Clinical ReviewDocument10 pagesWeeFIM Clinical Reviewsss_sarzzzNo ratings yet
- 11 17 17 Treatment PlanDocument7 pages11 17 17 Treatment Planapi-435469413No ratings yet
- Spinal Cord Assesment Form PTDocument8 pagesSpinal Cord Assesment Form PTSureaka PonnusamyNo ratings yet
- Kaleidoscope Therapy & Learning Center: Occupational Therapy Initial EvaluationDocument7 pagesKaleidoscope Therapy & Learning Center: Occupational Therapy Initial EvaluationJhudith De Julio BuhayNo ratings yet
- The Use of Occupational and Physical Therapies For Individuals With Autism Spectrum DisorderDocument45 pagesThe Use of Occupational and Physical Therapies For Individuals With Autism Spectrum DisorderAkhileshNo ratings yet
- Smart Goals Template 05Document2 pagesSmart Goals Template 05Shruti Sharma100% (1)
- PlayDocument3 pagesPlaybhawnatulsian0% (1)
- Basic Sensory Terms DefinitionsDocument2 pagesBasic Sensory Terms Definitionsapi-660820048No ratings yet
- Case Study For BipolarDocument7 pagesCase Study For Bipolarapi-285705203No ratings yet
- International Physical Activity Questionnaire - Short Form: Evaluation MeasuresDocument8 pagesInternational Physical Activity Questionnaire - Short Form: Evaluation MeasuresAyyNo ratings yet
- Intro To OT Evaluation and Intervention Part 1Document33 pagesIntro To OT Evaluation and Intervention Part 1Jica GulaNo ratings yet
- Marcus Evaluation - StruthersDocument8 pagesMarcus Evaluation - Struthersapi-355500890No ratings yet
- Depression Children PDFDocument2 pagesDepression Children PDFConstanzaNo ratings yet
- Quick DASHDocument4 pagesQuick DASHKennedy Hindley100% (1)
- IDEAL List of Tools and AssessmentsDocument10 pagesIDEAL List of Tools and AssessmentsAbeliz Durant MunizNo ratings yet
- Soap NoteDocument2 pagesSoap Noteapi-382628487No ratings yet
- The Children's Eating Behavior InventoryDocument14 pagesThe Children's Eating Behavior Inventoryguilherme augusto paroNo ratings yet
- VinelandDocument35 pagesVinelandHajra KhanNo ratings yet
- Guidelines Down Syndrome Assessment and Intervention PDFDocument292 pagesGuidelines Down Syndrome Assessment and Intervention PDFZenithaMeidaNo ratings yet
- By 3 Months of Age Does Your Child:: Motor SkillsDocument8 pagesBy 3 Months of Age Does Your Child:: Motor Skillso2andhemoglobinNo ratings yet
- Perkins Activity and Resource Guide Chapter 2 - Foundations of Learning Language, Cognition, and Social Relationships: Second Edition: Revised and UpdatedFrom EverandPerkins Activity and Resource Guide Chapter 2 - Foundations of Learning Language, Cognition, and Social Relationships: Second Edition: Revised and UpdatedNo ratings yet
- Ot102 Finals NotesDocument24 pagesOt102 Finals NotesFrancesNo ratings yet
- Ot Process NotesDocument2 pagesOt Process NotesFrancesNo ratings yet
- Long Quiz NotesDocument25 pagesLong Quiz NotesFrancesNo ratings yet
- Ot101 - Answer Key (Long Exams)Document6 pagesOt101 - Answer Key (Long Exams)FrancesNo ratings yet
- Healthcare in The PhilippinesDocument45 pagesHealthcare in The PhilippinesFrancesNo ratings yet
- Student Affairs Project AssignmentDocument9 pagesStudent Affairs Project Assignmentapi-428799429No ratings yet
- Cognitive NeuroscienceDocument4 pagesCognitive NeuroscienceAkhwand SaulatNo ratings yet
- Unit 2 Association and CommunityDocument14 pagesUnit 2 Association and CommunityVaibhav Kumar DevNo ratings yet
- Reading Faces To Understand People: Naomi TickleDocument5 pagesReading Faces To Understand People: Naomi TickleAnnaNo ratings yet
- Technical Theatre Design SyllabusDocument5 pagesTechnical Theatre Design Syllabusanon-579447No ratings yet
- The Status of Linguistics As A ScienceDocument6 pagesThe Status of Linguistics As A SciencePriscila HernandezNo ratings yet
- MGMT5007 Assessment 3Document7 pagesMGMT5007 Assessment 3rayNo ratings yet
- R VaughanDocument25 pagesR VaughanbmNo ratings yet
- 2.SociologyChild AbuseDocument7 pages2.SociologyChild Abusedew23No ratings yet
- CAARS Patient EnglishDocument2 pagesCAARS Patient Englishramav99759No ratings yet
- 4 1 Hs Sample LessonDocument3 pages4 1 Hs Sample Lessonapi-176967138No ratings yet
- Chapter 3: Learning From Others and Reviewing The LITERATURE (Answer Sheet)Document2 pagesChapter 3: Learning From Others and Reviewing The LITERATURE (Answer Sheet)Soriano AnjelynNo ratings yet
- Banagudos - Pe Assignment 2Document2 pagesBanagudos - Pe Assignment 2Angela BanagudosNo ratings yet
- Lesson 1 - Introduction To MILDocument44 pagesLesson 1 - Introduction To MILKim Raven Cayao AsahanNo ratings yet
- TRP Cards Freeman and Freeman Chapter 1Document3 pagesTRP Cards Freeman and Freeman Chapter 1api-285814614No ratings yet
- Test T23: C. Unemployment D. EnjoyedDocument5 pagesTest T23: C. Unemployment D. EnjoyedYến MaiNo ratings yet
- Political Thought and Political Thinkers (Judith N. Shklar (Auth.) Etc.) (Z-Library)Document214 pagesPolitical Thought and Political Thinkers (Judith N. Shklar (Auth.) Etc.) (Z-Library)Mike Alegrete CrespoNo ratings yet
- 16 Powerful Positive Affirmations For CalmnessDocument12 pages16 Powerful Positive Affirmations For CalmnessJamie BrownNo ratings yet
- Essay On Learning To Be A Better StudentDocument2 pagesEssay On Learning To Be A Better StudentJUSTINRAM GARCIANo ratings yet
- Student Motivation, School Culture, and Academic Achievement, What School Leaders Can DoDocument28 pagesStudent Motivation, School Culture, and Academic Achievement, What School Leaders Can DoTeo Eyu LiNo ratings yet
- Features of Individualism ColectivismDocument3 pagesFeatures of Individualism Colectivismgabystar101No ratings yet
- MODULE III Correctional AdministrationDocument5 pagesMODULE III Correctional AdministrationMarco Paolo PasnoNo ratings yet
- Gr. 4-READING INTERVENTION 2022-2023Document3 pagesGr. 4-READING INTERVENTION 2022-2023romina maningasNo ratings yet
- Gag Reflex: Prepared By: Final Year K.M.S. DentalDocument26 pagesGag Reflex: Prepared By: Final Year K.M.S. DentalMuaiyed Buzayan AkremyNo ratings yet