
Kern Chapter 1
Kern Chapter 1
You might also like
- Short Answer Questions CHCCSM004Document14 pagesShort Answer Questions CHCCSM004Tmg Preity100% (2)
- Adams 2022.1 Installation GuideDocument138 pagesAdams 2022.1 Installation GuidedbNo ratings yet
- Obe PDFDocument6 pagesObe PDFjaycee_evangelistaNo ratings yet
- Date & Time Cues Need Nursing Diagnosis Objective/Goal Nursing Interventions Evaluation Novem Ber A Fatigue Related ToDocument4 pagesDate & Time Cues Need Nursing Diagnosis Objective/Goal Nursing Interventions Evaluation Novem Ber A Fatigue Related ToCarissa DenogaNo ratings yet
- Teen Pregnancy PresentationDocument12 pagesTeen Pregnancy Presentationapi-501254101100% (1)
- Template For Evaluation of Curriculum Week 4Document12 pagesTemplate For Evaluation of Curriculum Week 4api-598498344No ratings yet
- AMEE Guide No. 14: Outcome-Based Education: An Introduction To Outcome-Based EducationDocument36 pagesAMEE Guide No. 14: Outcome-Based Education: An Introduction To Outcome-Based EducationVaqar BariNo ratings yet
- Assessment of Learning NeedsDocument4 pagesAssessment of Learning NeedsRhonaJoyNo ratings yet
- Curriculum Alignment and EvaluationDocument11 pagesCurriculum Alignment and Evaluationapi-695177304No ratings yet
- UA OMSE Med/Ed Enews v3 No. 01 (AUG 2014)Document10 pagesUA OMSE Med/Ed Enews v3 No. 01 (AUG 2014)KC Spear Ellinwood, former Director Instructional DevelopmentNo ratings yet
- Jayson NovellesDocument38 pagesJayson Novellesaronara dalampasiganNo ratings yet
- Group-Based, Person-Centered Diabetes Self-Management Education: Healthcare Professionals ' Implementation of New ApproachesDocument11 pagesGroup-Based, Person-Centered Diabetes Self-Management Education: Healthcare Professionals ' Implementation of New ApproachesChristian MolimaNo ratings yet
- PentagiumonDocument38 pagesPentagiumonblain mathewNo ratings yet
- 1 s2.0 S1807593222001119 MainDocument6 pages1 s2.0 S1807593222001119 MainNadiraNo ratings yet
- 2012.10.23 HC Curriculum OverviewDocument23 pages2012.10.23 HC Curriculum Overviewjere muthamaNo ratings yet
- Declaración de Consenso Sobre El Contenido de Los Currículos de Razonamiento Clínico en La Educación Médica de Pregrado 2020 INGLESDocument9 pagesDeclaración de Consenso Sobre El Contenido de Los Currículos de Razonamiento Clínico en La Educación Médica de Pregrado 2020 INGLESjaldoquiNo ratings yet
- Development of Decision-Making in PharmacyDocument11 pagesDevelopment of Decision-Making in PharmacyRasheed AliNo ratings yet
- Medical Education in The United States. The Role of AndragogyDocument5 pagesMedical Education in The United States. The Role of AndragogydarkbyronsNo ratings yet
- Develop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenDocument8 pagesDevelop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenpsicoterapiavaldiviaNo ratings yet
- Osborne+et+al +the+health+education+impact+questionnaireDocument10 pagesOsborne+et+al +the+health+education+impact+questionnairesandrine.abellarNo ratings yet
- Med/Ed Enews v3 No. 06 (MAY 2015)Document13 pagesMed/Ed Enews v3 No. 06 (MAY 2015)KC Spear Ellinwood, former Director Instructional DevelopmentNo ratings yet
- 725 Research ProposalDocument13 pages725 Research Proposalapi-676510959No ratings yet
- Makoul, 2007Document10 pagesMakoul, 2007aminNo ratings yet
- Development and Evaluation of A Questionnaire To Measure The Perceived Implementation of The Mission Statement of A Competency Based CurriculumDocument13 pagesDevelopment and Evaluation of A Questionnaire To Measure The Perceived Implementation of The Mission Statement of A Competency Based CurriculumfidelbustamiNo ratings yet
- Article - INFUSION - OF - AGE-FRIENDLY - PRINCIPLES - INTO - CURRICULADocument1 pageArticle - INFUSION - OF - AGE-FRIENDLY - PRINCIPLES - INTO - CURRICULAHarlene ArabiaNo ratings yet
- Running Head: Teaching Project Paper 1Document10 pagesRunning Head: Teaching Project Paper 1api-539369902No ratings yet
- Curriculum Development Half-Day WorkshopDocument103 pagesCurriculum Development Half-Day WorkshopSima SunNo ratings yet
- Clinical Objectives PDFDocument4 pagesClinical Objectives PDFYhuhan James TejadaNo ratings yet
- Written Assignment CPDDocument12 pagesWritten Assignment CPDLOGESWARRY K.VESUPATHYNo ratings yet
- G1 Clinic Chapter 1-3 Final 1ST SemDocument50 pagesG1 Clinic Chapter 1-3 Final 1ST SemBedecir, Schrister Hynes D.No ratings yet
- Method PrecedesDocument7 pagesMethod PrecedesScribdTranslationsNo ratings yet
- AMEE Guide No 56-The Research Compas An Introduction To Research in Medical EducationDocument15 pagesAMEE Guide No 56-The Research Compas An Introduction To Research in Medical EducationgladystubaradNo ratings yet
- The Use of Social Media As A Tool To Educate United Kingdom Undergraduate Pharmacy Students About Public HealthDocument32 pagesThe Use of Social Media As A Tool To Educate United Kingdom Undergraduate Pharmacy Students About Public HealthStella MarisNo ratings yet
- Assessment of Non-Cognitive Factors - CushingDocument43 pagesAssessment of Non-Cognitive Factors - Cushingapi-3764755No ratings yet
- Khyati 2Document8 pagesKhyati 2anisha08.islamNo ratings yet
- Clinical Teaching: Sixty Tips For Successful Implementation: Research ArticleDocument11 pagesClinical Teaching: Sixty Tips For Successful Implementation: Research ArticleChezka MendozaNo ratings yet
- Barriers and Solutions To Implementing The Staff Education On Depression Screening and Follow - EditedDocument4 pagesBarriers and Solutions To Implementing The Staff Education On Depression Screening and Follow - EditedViotry ChepkwonyNo ratings yet
- Using Field Notes To Evaluate Competencies in Family Medicine Training: A Study of Predictors of IntentionDocument10 pagesUsing Field Notes To Evaluate Competencies in Family Medicine Training: A Study of Predictors of IntentionMirna Liliana Carmona GarciaNo ratings yet
- Nurs3126 Co - 2021.01.06Document27 pagesNurs3126 Co - 2021.01.06nolifeNo ratings yet
- Obesity Medicine Rotation OMA HP Student Syllabus 4 WK Online RotationDocument9 pagesObesity Medicine Rotation OMA HP Student Syllabus 4 WK Online RotationWill HNo ratings yet
- The Development of A Questionnaire To Assess The Readiness (Nurse)Document6 pagesThe Development of A Questionnaire To Assess The Readiness (Nurse)neizhaNo ratings yet
- The State of Communication Education in Family Medicine ResidenciesDocument7 pagesThe State of Communication Education in Family Medicine ResidenciesSilih Pulihan MedrofaNo ratings yet
- New Paradigm For CME - JCEHP Sep 2011Document8 pagesNew Paradigm For CME - JCEHP Sep 2011Daniel GuineeNo ratings yet
- Perspective On Teaching and LearningDocument43 pagesPerspective On Teaching and LearningJonalyn Cielito Francisco100% (2)
- Health Case Studies 1512494009Document258 pagesHealth Case Studies 1512494009lisa weareNo ratings yet
- Innovations in Medical Education - Arpit RevisedDocument10 pagesInnovations in Medical Education - Arpit RevisedArjumand FaruqiNo ratings yet
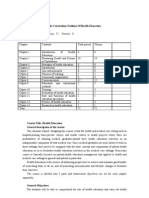
- The Curriculum Outlines of Health EducationDocument6 pagesThe Curriculum Outlines of Health Educationapi-3728690No ratings yet
- Critically Appraised Articles 3Document15 pagesCritically Appraised Articles 3api-638750949No ratings yet
- Writing Objectives WebDocument27 pagesWriting Objectives WebBeenish ShahNo ratings yet
- Teaching The Medical Interview: Methods and Key Learning Issues in A Faculty Development CourseDocument8 pagesTeaching The Medical Interview: Methods and Key Learning Issues in A Faculty Development CourseMaw BerryNo ratings yet
- Submit Due 9.12Document11 pagesSubmit Due 9.12Are HidayuNo ratings yet
- Final Research PaperDocument15 pagesFinal Research Paperapi-647278206No ratings yet
- Nur 602 Week 4 NarrativeDocument10 pagesNur 602 Week 4 Narrativeapi-429205355No ratings yet
- Slick J. - Project ProfessionalismDocument2 pagesSlick J. - Project ProfessionalismStachen SharpenerNo ratings yet
- Evaluation Methods For Prevention EducationDocument7 pagesEvaluation Methods For Prevention EducationtimtimNo ratings yet
- Nursing Arts LO Module 4Document7 pagesNursing Arts LO Module 4AmberpersonNo ratings yet
- Cadorin 2017 Instruments Evaluating The Self DirDocument13 pagesCadorin 2017 Instruments Evaluating The Self DirAndrada Marko PoloNo ratings yet
- Aet2 10354Document8 pagesAet2 10354Edris ZamroniNo ratings yet
- UA OMSE Med/Ed Enews v3 No. 02 (SEP 2014)Document10 pagesUA OMSE Med/Ed Enews v3 No. 02 (SEP 2014)KC Spear Ellinwood, former Director Instructional DevelopmentNo ratings yet
- The Core Curriculum and Integration in Medical Education: Nikoo Yamani, Masoumeh RahimiDocument5 pagesThe Core Curriculum and Integration in Medical Education: Nikoo Yamani, Masoumeh RahimiDoctorRonZ7No ratings yet
- Course Design for Public Health: A Competency Based ApproachFrom EverandCourse Design for Public Health: A Competency Based ApproachNo ratings yet
- Relationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationFrom EverandRelationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationNo ratings yet
- Quality Assurance in Medical Education: A Practical GuideFrom EverandQuality Assurance in Medical Education: A Practical GuideNo ratings yet
- P.V.C Pump Private Limited Plot No. 1c Industrial Area, Lokikere Road Davanagere-577005 Off.: 08192-260014Document1 pageP.V.C Pump Private Limited Plot No. 1c Industrial Area, Lokikere Road Davanagere-577005 Off.: 08192-260014Darshan DarshuNo ratings yet
- Shading Answer SheetDocument2 pagesShading Answer SheetSir D. LPT VlogNo ratings yet
- Slabon - CV - 05Document11 pagesSlabon - CV - 05api-655567758No ratings yet
- Semester - I: R.T.M.Nagpur University, Nagpur Syllabus For Bachelor of Science Part - I Supplementary English CourseDocument4 pagesSemester - I: R.T.M.Nagpur University, Nagpur Syllabus For Bachelor of Science Part - I Supplementary English CourseAkash DNo ratings yet
- En Paris Campus Other ProgramsDocument14 pagesEn Paris Campus Other ProgramsPinakpani DasNo ratings yet
- Afghanistan ResearchCenterProposalDocument8 pagesAfghanistan ResearchCenterProposalBarba GulatNo ratings yet
- Botswana Research PaperDocument7 pagesBotswana Research Paperfvj8675e100% (1)
- CUET UG ScoreCardDocument1 pageCUET UG ScoreCardraw991998No ratings yet
- Business Analytics Report: "The Factors Affect To Customers' Satisfaction of Techcombank Banking Services"Document8 pagesBusiness Analytics Report: "The Factors Affect To Customers' Satisfaction of Techcombank Banking Services"SơnNo ratings yet
- TESOL Methodology: Unit - 3 Teaching MethodsDocument26 pagesTESOL Methodology: Unit - 3 Teaching MethodsYhoel CalleNo ratings yet
- Department of Education: A Conversation - 3. A Speech or Presentation - 4. Having A Phone Call With SomeoneDocument2 pagesDepartment of Education: A Conversation - 3. A Speech or Presentation - 4. Having A Phone Call With SomeoneJan Alleana FernandezNo ratings yet
- IELTS Speaking Study Plan - 2 Months PDFDocument12 pagesIELTS Speaking Study Plan - 2 Months PDFAli AsgerovNo ratings yet
- What Happens If You Fail To Defend Your ThesisDocument5 pagesWhat Happens If You Fail To Defend Your Thesissprxzfugg100% (2)
- Math11 SP Q3 M8 PDFDocument12 pagesMath11 SP Q3 M8 PDFJessa Banawan EdulanNo ratings yet
- Lane - NIT-1Document11 pagesLane - NIT-1narendra29000No ratings yet
- (16-028) Final Essay - ELEVAZODocument2 pages(16-028) Final Essay - ELEVAZOMAEVEL HYACINTH ELEVAZONo ratings yet
- Middle School Interview QuestionsDocument3 pagesMiddle School Interview QuestionsJP ENGLISH100% (1)
- Assignment - Questionnaire Development - Chapter 15Document6 pagesAssignment - Questionnaire Development - Chapter 15akashNo ratings yet
- Indian Tra QUANTDocument148 pagesIndian Tra QUANTDevendra Yadav ME 23100% (1)
- Clinical Decision Making in Mental Health PracticeDocument339 pagesClinical Decision Making in Mental Health PracticeLeidy Paola Mendez Roncancio100% (3)
- Red Hat Enterprise Linux-6Document809 pagesRed Hat Enterprise Linux-6lamsal123No ratings yet
- Course Hero Application KitDocument17 pagesCourse Hero Application KitRONALYN GONZALESNo ratings yet
- Project RubricDocument2 pagesProject Rubricapi-246410580100% (1)
- ERP BibliographyDocument56 pagesERP BibliographySmriti MishraNo ratings yet
- Color WheelDocument3 pagesColor Wheelapi-300965210No ratings yet
- GCAC Fall 2023 Course DescriptionsDocument6 pagesGCAC Fall 2023 Course DescriptionspranavshreniNo ratings yet
- Guidance On Teaching, Learning and Assessment at Key Stage 4Document115 pagesGuidance On Teaching, Learning and Assessment at Key Stage 4Lisa TalNo ratings yet
























































































Download as pdf or txt
You might also like
- Short Answer Questions CHCCSM004Document14 pagesShort Answer Questions CHCCSM004Tmg Preity100% (2)
- Adams 2022.1 Installation GuideDocument138 pagesAdams 2022.1 Installation GuidedbNo ratings yet
- Obe PDFDocument6 pagesObe PDFjaycee_evangelistaNo ratings yet
- Date & Time Cues Need Nursing Diagnosis Objective/Goal Nursing Interventions Evaluation Novem Ber A Fatigue Related ToDocument4 pagesDate & Time Cues Need Nursing Diagnosis Objective/Goal Nursing Interventions Evaluation Novem Ber A Fatigue Related ToCarissa DenogaNo ratings yet
- Teen Pregnancy PresentationDocument12 pagesTeen Pregnancy Presentationapi-501254101100% (1)
- Template For Evaluation of Curriculum Week 4Document12 pagesTemplate For Evaluation of Curriculum Week 4api-598498344No ratings yet
- AMEE Guide No. 14: Outcome-Based Education: An Introduction To Outcome-Based EducationDocument36 pagesAMEE Guide No. 14: Outcome-Based Education: An Introduction To Outcome-Based EducationVaqar BariNo ratings yet
- Assessment of Learning NeedsDocument4 pagesAssessment of Learning NeedsRhonaJoyNo ratings yet
- Curriculum Alignment and EvaluationDocument11 pagesCurriculum Alignment and Evaluationapi-695177304No ratings yet
- UA OMSE Med/Ed Enews v3 No. 01 (AUG 2014)Document10 pagesUA OMSE Med/Ed Enews v3 No. 01 (AUG 2014)KC Spear Ellinwood, former Director Instructional DevelopmentNo ratings yet
- Jayson NovellesDocument38 pagesJayson Novellesaronara dalampasiganNo ratings yet
- Group-Based, Person-Centered Diabetes Self-Management Education: Healthcare Professionals ' Implementation of New ApproachesDocument11 pagesGroup-Based, Person-Centered Diabetes Self-Management Education: Healthcare Professionals ' Implementation of New ApproachesChristian MolimaNo ratings yet
- PentagiumonDocument38 pagesPentagiumonblain mathewNo ratings yet
- 1 s2.0 S1807593222001119 MainDocument6 pages1 s2.0 S1807593222001119 MainNadiraNo ratings yet
- 2012.10.23 HC Curriculum OverviewDocument23 pages2012.10.23 HC Curriculum Overviewjere muthamaNo ratings yet
- Declaración de Consenso Sobre El Contenido de Los Currículos de Razonamiento Clínico en La Educación Médica de Pregrado 2020 INGLESDocument9 pagesDeclaración de Consenso Sobre El Contenido de Los Currículos de Razonamiento Clínico en La Educación Médica de Pregrado 2020 INGLESjaldoquiNo ratings yet
- Development of Decision-Making in PharmacyDocument11 pagesDevelopment of Decision-Making in PharmacyRasheed AliNo ratings yet
- Medical Education in The United States. The Role of AndragogyDocument5 pagesMedical Education in The United States. The Role of AndragogydarkbyronsNo ratings yet
- Develop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenDocument8 pagesDevelop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenpsicoterapiavaldiviaNo ratings yet
- Osborne+et+al +the+health+education+impact+questionnaireDocument10 pagesOsborne+et+al +the+health+education+impact+questionnairesandrine.abellarNo ratings yet
- Med/Ed Enews v3 No. 06 (MAY 2015)Document13 pagesMed/Ed Enews v3 No. 06 (MAY 2015)KC Spear Ellinwood, former Director Instructional DevelopmentNo ratings yet
- 725 Research ProposalDocument13 pages725 Research Proposalapi-676510959No ratings yet
- Makoul, 2007Document10 pagesMakoul, 2007aminNo ratings yet
- Development and Evaluation of A Questionnaire To Measure The Perceived Implementation of The Mission Statement of A Competency Based CurriculumDocument13 pagesDevelopment and Evaluation of A Questionnaire To Measure The Perceived Implementation of The Mission Statement of A Competency Based CurriculumfidelbustamiNo ratings yet
- Article - INFUSION - OF - AGE-FRIENDLY - PRINCIPLES - INTO - CURRICULADocument1 pageArticle - INFUSION - OF - AGE-FRIENDLY - PRINCIPLES - INTO - CURRICULAHarlene ArabiaNo ratings yet
- Running Head: Teaching Project Paper 1Document10 pagesRunning Head: Teaching Project Paper 1api-539369902No ratings yet
- Curriculum Development Half-Day WorkshopDocument103 pagesCurriculum Development Half-Day WorkshopSima SunNo ratings yet
- Clinical Objectives PDFDocument4 pagesClinical Objectives PDFYhuhan James TejadaNo ratings yet
- Written Assignment CPDDocument12 pagesWritten Assignment CPDLOGESWARRY K.VESUPATHYNo ratings yet
- G1 Clinic Chapter 1-3 Final 1ST SemDocument50 pagesG1 Clinic Chapter 1-3 Final 1ST SemBedecir, Schrister Hynes D.No ratings yet
- Method PrecedesDocument7 pagesMethod PrecedesScribdTranslationsNo ratings yet
- AMEE Guide No 56-The Research Compas An Introduction To Research in Medical EducationDocument15 pagesAMEE Guide No 56-The Research Compas An Introduction To Research in Medical EducationgladystubaradNo ratings yet
- The Use of Social Media As A Tool To Educate United Kingdom Undergraduate Pharmacy Students About Public HealthDocument32 pagesThe Use of Social Media As A Tool To Educate United Kingdom Undergraduate Pharmacy Students About Public HealthStella MarisNo ratings yet
- Assessment of Non-Cognitive Factors - CushingDocument43 pagesAssessment of Non-Cognitive Factors - Cushingapi-3764755No ratings yet
- Khyati 2Document8 pagesKhyati 2anisha08.islamNo ratings yet
- Clinical Teaching: Sixty Tips For Successful Implementation: Research ArticleDocument11 pagesClinical Teaching: Sixty Tips For Successful Implementation: Research ArticleChezka MendozaNo ratings yet
- Barriers and Solutions To Implementing The Staff Education On Depression Screening and Follow - EditedDocument4 pagesBarriers and Solutions To Implementing The Staff Education On Depression Screening and Follow - EditedViotry ChepkwonyNo ratings yet
- Using Field Notes To Evaluate Competencies in Family Medicine Training: A Study of Predictors of IntentionDocument10 pagesUsing Field Notes To Evaluate Competencies in Family Medicine Training: A Study of Predictors of IntentionMirna Liliana Carmona GarciaNo ratings yet
- Nurs3126 Co - 2021.01.06Document27 pagesNurs3126 Co - 2021.01.06nolifeNo ratings yet
- Obesity Medicine Rotation OMA HP Student Syllabus 4 WK Online RotationDocument9 pagesObesity Medicine Rotation OMA HP Student Syllabus 4 WK Online RotationWill HNo ratings yet
- The Development of A Questionnaire To Assess The Readiness (Nurse)Document6 pagesThe Development of A Questionnaire To Assess The Readiness (Nurse)neizhaNo ratings yet
- The State of Communication Education in Family Medicine ResidenciesDocument7 pagesThe State of Communication Education in Family Medicine ResidenciesSilih Pulihan MedrofaNo ratings yet
- New Paradigm For CME - JCEHP Sep 2011Document8 pagesNew Paradigm For CME - JCEHP Sep 2011Daniel GuineeNo ratings yet
- Perspective On Teaching and LearningDocument43 pagesPerspective On Teaching and LearningJonalyn Cielito Francisco100% (2)
- Health Case Studies 1512494009Document258 pagesHealth Case Studies 1512494009lisa weareNo ratings yet
- Innovations in Medical Education - Arpit RevisedDocument10 pagesInnovations in Medical Education - Arpit RevisedArjumand FaruqiNo ratings yet
- The Curriculum Outlines of Health EducationDocument6 pagesThe Curriculum Outlines of Health Educationapi-3728690No ratings yet
- Critically Appraised Articles 3Document15 pagesCritically Appraised Articles 3api-638750949No ratings yet
- Writing Objectives WebDocument27 pagesWriting Objectives WebBeenish ShahNo ratings yet
- Teaching The Medical Interview: Methods and Key Learning Issues in A Faculty Development CourseDocument8 pagesTeaching The Medical Interview: Methods and Key Learning Issues in A Faculty Development CourseMaw BerryNo ratings yet
- Submit Due 9.12Document11 pagesSubmit Due 9.12Are HidayuNo ratings yet
- Final Research PaperDocument15 pagesFinal Research Paperapi-647278206No ratings yet
- Nur 602 Week 4 NarrativeDocument10 pagesNur 602 Week 4 Narrativeapi-429205355No ratings yet
- Slick J. - Project ProfessionalismDocument2 pagesSlick J. - Project ProfessionalismStachen SharpenerNo ratings yet
- Evaluation Methods For Prevention EducationDocument7 pagesEvaluation Methods For Prevention EducationtimtimNo ratings yet
- Nursing Arts LO Module 4Document7 pagesNursing Arts LO Module 4AmberpersonNo ratings yet
- Cadorin 2017 Instruments Evaluating The Self DirDocument13 pagesCadorin 2017 Instruments Evaluating The Self DirAndrada Marko PoloNo ratings yet
- Aet2 10354Document8 pagesAet2 10354Edris ZamroniNo ratings yet
- UA OMSE Med/Ed Enews v3 No. 02 (SEP 2014)Document10 pagesUA OMSE Med/Ed Enews v3 No. 02 (SEP 2014)KC Spear Ellinwood, former Director Instructional DevelopmentNo ratings yet
- The Core Curriculum and Integration in Medical Education: Nikoo Yamani, Masoumeh RahimiDocument5 pagesThe Core Curriculum and Integration in Medical Education: Nikoo Yamani, Masoumeh RahimiDoctorRonZ7No ratings yet
- Course Design for Public Health: A Competency Based ApproachFrom EverandCourse Design for Public Health: A Competency Based ApproachNo ratings yet
- Relationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationFrom EverandRelationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationNo ratings yet
- Quality Assurance in Medical Education: A Practical GuideFrom EverandQuality Assurance in Medical Education: A Practical GuideNo ratings yet
- P.V.C Pump Private Limited Plot No. 1c Industrial Area, Lokikere Road Davanagere-577005 Off.: 08192-260014Document1 pageP.V.C Pump Private Limited Plot No. 1c Industrial Area, Lokikere Road Davanagere-577005 Off.: 08192-260014Darshan DarshuNo ratings yet
- Shading Answer SheetDocument2 pagesShading Answer SheetSir D. LPT VlogNo ratings yet
- Slabon - CV - 05Document11 pagesSlabon - CV - 05api-655567758No ratings yet
- Semester - I: R.T.M.Nagpur University, Nagpur Syllabus For Bachelor of Science Part - I Supplementary English CourseDocument4 pagesSemester - I: R.T.M.Nagpur University, Nagpur Syllabus For Bachelor of Science Part - I Supplementary English CourseAkash DNo ratings yet
- En Paris Campus Other ProgramsDocument14 pagesEn Paris Campus Other ProgramsPinakpani DasNo ratings yet
- Afghanistan ResearchCenterProposalDocument8 pagesAfghanistan ResearchCenterProposalBarba GulatNo ratings yet
- Botswana Research PaperDocument7 pagesBotswana Research Paperfvj8675e100% (1)
- CUET UG ScoreCardDocument1 pageCUET UG ScoreCardraw991998No ratings yet
- Business Analytics Report: "The Factors Affect To Customers' Satisfaction of Techcombank Banking Services"Document8 pagesBusiness Analytics Report: "The Factors Affect To Customers' Satisfaction of Techcombank Banking Services"SơnNo ratings yet
- TESOL Methodology: Unit - 3 Teaching MethodsDocument26 pagesTESOL Methodology: Unit - 3 Teaching MethodsYhoel CalleNo ratings yet
- Department of Education: A Conversation - 3. A Speech or Presentation - 4. Having A Phone Call With SomeoneDocument2 pagesDepartment of Education: A Conversation - 3. A Speech or Presentation - 4. Having A Phone Call With SomeoneJan Alleana FernandezNo ratings yet
- IELTS Speaking Study Plan - 2 Months PDFDocument12 pagesIELTS Speaking Study Plan - 2 Months PDFAli AsgerovNo ratings yet
- What Happens If You Fail To Defend Your ThesisDocument5 pagesWhat Happens If You Fail To Defend Your Thesissprxzfugg100% (2)
- Math11 SP Q3 M8 PDFDocument12 pagesMath11 SP Q3 M8 PDFJessa Banawan EdulanNo ratings yet
- Lane - NIT-1Document11 pagesLane - NIT-1narendra29000No ratings yet
- (16-028) Final Essay - ELEVAZODocument2 pages(16-028) Final Essay - ELEVAZOMAEVEL HYACINTH ELEVAZONo ratings yet
- Middle School Interview QuestionsDocument3 pagesMiddle School Interview QuestionsJP ENGLISH100% (1)
- Assignment - Questionnaire Development - Chapter 15Document6 pagesAssignment - Questionnaire Development - Chapter 15akashNo ratings yet
- Indian Tra QUANTDocument148 pagesIndian Tra QUANTDevendra Yadav ME 23100% (1)
- Clinical Decision Making in Mental Health PracticeDocument339 pagesClinical Decision Making in Mental Health PracticeLeidy Paola Mendez Roncancio100% (3)
- Red Hat Enterprise Linux-6Document809 pagesRed Hat Enterprise Linux-6lamsal123No ratings yet
- Course Hero Application KitDocument17 pagesCourse Hero Application KitRONALYN GONZALESNo ratings yet
- Project RubricDocument2 pagesProject Rubricapi-246410580100% (1)
- ERP BibliographyDocument56 pagesERP BibliographySmriti MishraNo ratings yet
- Color WheelDocument3 pagesColor Wheelapi-300965210No ratings yet
- GCAC Fall 2023 Course DescriptionsDocument6 pagesGCAC Fall 2023 Course DescriptionspranavshreniNo ratings yet
- Guidance On Teaching, Learning and Assessment at Key Stage 4Document115 pagesGuidance On Teaching, Learning and Assessment at Key Stage 4Lisa TalNo ratings yet