Download as pdf or txt
You might also like
- Quality Venipuncture: Special ConsiderationsDocument1 pageQuality Venipuncture: Special ConsiderationsAdicciòn entre LetrasNo ratings yet
- (White, John) Health and Safety ManagementDocument163 pages(White, John) Health and Safety ManagementRoj Peter Orzales100% (3)
- 10 1111@jdv 16752Document14 pages10 1111@jdv 16752barinho_No ratings yet
- Guideline KulitDocument38 pagesGuideline KulitRidho ForesNo ratings yet
- Chronic Nodular Prurigo: Clinical Pro File and Burden. A European Cross-Sectional StudyDocument11 pagesChronic Nodular Prurigo: Clinical Pro File and Burden. A European Cross-Sectional StudyAdiantoWinataTjiaNo ratings yet
- Prenatal PhenotypingDocument12 pagesPrenatal PhenotypingBenyam ZenebeNo ratings yet
- Pmed 1003208Document23 pagesPmed 1003208Nindie AulhieyaNo ratings yet
- Lancet 2023Document17 pagesLancet 2023Julia Urquiza LandaluceNo ratings yet
- Ijc 25050Document10 pagesIjc 25050Deviat Ast AmierNo ratings yet
- Casos y ControlesDocument12 pagesCasos y ControlestomasNo ratings yet
- ConsDocument29 pagesConsanon_526533404No ratings yet
- Acad Dermatol Venereol - 2018 - Wollenberg - Consensus Based European Guidelines For Treatment of Atopic Eczema AtopicDocument29 pagesAcad Dermatol Venereol - 2018 - Wollenberg - Consensus Based European Guidelines For Treatment of Atopic Eczema AtopicTúUyênSirisNo ratings yet
- PDF Soumission Révisions Papier2 MLetouzey v2-26-61Document36 pagesPDF Soumission Révisions Papier2 MLetouzey v2-26-61Stevie Guisbert ElescanoNo ratings yet
- 10 1371@journal Pone 0229380Document18 pages10 1371@journal Pone 0229380NESLİHAN ORALNo ratings yet
- Abstracts 853 125: 4 OCTOBER 2005: BackgroundDocument1 pageAbstracts 853 125: 4 OCTOBER 2005: BackgroundkelbmutsNo ratings yet
- ESCMID Guideline For The Diagnosis and Management of Candida Diseases 2012: Diagnostic ProceduresDocument10 pagesESCMID Guideline For The Diagnosis and Management of Candida Diseases 2012: Diagnostic ProceduresiisisiisNo ratings yet
- EDF-guideline Atopic-Eczema Update2018 PDFDocument117 pagesEDF-guideline Atopic-Eczema Update2018 PDFMonica MonikaNo ratings yet
- 10 1371@journal Pmed 1002744Document22 pages10 1371@journal Pmed 1002744christian murtaniNo ratings yet
- Use of Early Intervention For Young Children With Autism Spectrum Disorder Across EuropeDocument39 pagesUse of Early Intervention For Young Children With Autism Spectrum Disorder Across EuropeRenata BorgesNo ratings yet
- Virus y M. Pneumoniae Son Los Ppales Agentes Etiologicas de NAC en Pacientes Hospitalizados en EspañaDocument11 pagesVirus y M. Pneumoniae Son Los Ppales Agentes Etiologicas de NAC en Pacientes Hospitalizados en EspañaFernando FernándezNo ratings yet
- Pediatric Evans Syndrome Is Associated With A High Frequency of PDFDocument41 pagesPediatric Evans Syndrome Is Associated With A High Frequency of PDFJerryEddyaPutraBoerNo ratings yet
- Guias Dracma Ingles CompletaDocument125 pagesGuias Dracma Ingles CompletaaachgNo ratings yet
- Childhood-Onset of Primary Sjögren Syndrome: Phenotypic Characterization at Diagnosis of 158 ChildrenDocument25 pagesChildhood-Onset of Primary Sjögren Syndrome: Phenotypic Characterization at Diagnosis of 158 ChildrensilviaNo ratings yet
- Journal ReadingDocument9 pagesJournal Readingshirley_ling_15No ratings yet
- 1 s2.0 S1198743X14607631 MainDocument8 pages1 s2.0 S1198743X14607631 MainiisisiisNo ratings yet
- 2022 - European Guideline Dermite AtopiqueDocument23 pages2022 - European Guideline Dermite AtopiqueLydia LydiaNo ratings yet
- Acad Dermatol Venereol - 2020 - Wollenberg - ETFAD EADV Eczema Task Force 2020 Position Paper On Diagnosis and Treatment ofDocument28 pagesAcad Dermatol Venereol - 2020 - Wollenberg - ETFAD EADV Eczema Task Force 2020 Position Paper On Diagnosis and Treatment ofmaituuyen1997No ratings yet
- 10 1111@bjd 19561Document31 pages10 1111@bjd 19561Fang MuNo ratings yet
- Alzheimer's DiseaseDocument31 pagesAlzheimer's DiseasePAULA ITZEL AVALOS POLANCONo ratings yet
- 03.2018 ScabiesDocument38 pages03.2018 ScabiesputriNo ratings yet
- PIMS SUIZA FrontiersDocument14 pagesPIMS SUIZA FrontiersDeyanira May BastoNo ratings yet
- Soil Transmitted Helminth PDFDocument90 pagesSoil Transmitted Helminth PDFMinarni HoNo ratings yet
- Faktor Risiko HipospadiDocument8 pagesFaktor Risiko HipospadiNindhyaPutriNo ratings yet
- 1 s2.0 S2213219820303718 MainDocument20 pages1 s2.0 S2213219820303718 Mainrawr rawrNo ratings yet
- EDF Guideline AE 2018 - Modified - 190508Document117 pagesEDF Guideline AE 2018 - Modified - 190508Iuliana TarceaNo ratings yet
- Acad Dermatol Venereol - 2018 - Wollenberg - Consensus Based European Guidelines For Treatment of Atopic Eczema AtopicDocument26 pagesAcad Dermatol Venereol - 2018 - Wollenberg - Consensus Based European Guidelines For Treatment of Atopic Eczema Atopicmaituuyen1997No ratings yet
- TB GrahamDocument10 pagesTB GrahamAsri RachmawatiNo ratings yet
- 2018 Article 279 PDFDocument14 pages2018 Article 279 PDFvinni_mandasariNo ratings yet
- Bio Project LatestDocument42 pagesBio Project LatestDebdeep DanNo ratings yet
- Algorithm For Treatment of ImpetigoDocument9 pagesAlgorithm For Treatment of Impetigodrmostafa087No ratings yet
- 1 s2Document3 pages1 s2RyanNo ratings yet
- CDC 30614 DS1Document29 pagesCDC 30614 DS1David Sergio Salas VargasNo ratings yet
- mySinusitisCoach - Patient Empowerment in Chronic Rhinosinusitis Using Mobile TechnologyDocument7 pagesmySinusitisCoach - Patient Empowerment in Chronic Rhinosinusitis Using Mobile TechnologyMRMISSYNo ratings yet
- PIISComplicationsDocument12 pagesPIISComplicationsPhuong VuNo ratings yet
- Nps D8Document7 pagesNps D8Jasper Benjamin JuradoNo ratings yet
- Guideline For Treatment of Cutaneous Lupus Erythematosus Guided by TheDocument16 pagesGuideline For Treatment of Cutaneous Lupus Erythematosus Guided by TheLydia LydiaNo ratings yet
- 1 s2.0 S1198743X14607667 MainDocument15 pages1 s2.0 S1198743X14607667 MainiisisiisNo ratings yet
- 1471 5945 13 12Document5 pages1471 5945 13 12jukilokiNo ratings yet
- Cancers 12 02747Document15 pagesCancers 12 02747Hematología INSNSBNo ratings yet
- Guillon Baduel Et Al AUTISM Detection AutismDocument36 pagesGuillon Baduel Et Al AUTISM Detection AutismjoseNo ratings yet
- Aria Guidelines 2016 Revision PDFDocument9 pagesAria Guidelines 2016 Revision PDFSiska HarapanNo ratings yet
- Community-Acquired Pneumonia: Strategies for ManagementFrom EverandCommunity-Acquired Pneumonia: Strategies for ManagementAntoni TorresRating: 4.5 out of 5 stars4.5/5 (2)
- Atopic guideline-JEADV 2022 Part IIDocument23 pagesAtopic guideline-JEADV 2022 Part IIwasuchon chaichanNo ratings yet
- Roujeau 1995Document8 pagesRoujeau 1995Dimas Gatra DiantoroNo ratings yet
- CR Mbak YuliDocument10 pagesCR Mbak YuliNovel WidyaNo ratings yet
- Gist Richtlijn (Esmo Eurocan)Document40 pagesGist Richtlijn (Esmo Eurocan)Bas FrietmanNo ratings yet
- Impact of COVID-19 On Pediatric Asthma in RsudzaDocument11 pagesImpact of COVID-19 On Pediatric Asthma in Rsudzatayo diqNo ratings yet
- ESPGHAN - ESPEN - ESPR Guidelines On Pediatric Parenteral Nutrition ComplicationsDocument12 pagesESPGHAN - ESPEN - ESPR Guidelines On Pediatric Parenteral Nutrition Complicationsalexandra BravoNo ratings yet
- Olfactory and Oral Manifestations of COVID-19: Sex-Related Symptoms - A Potential Pathway To Early DiagnosisDocument7 pagesOlfactory and Oral Manifestations of COVID-19: Sex-Related Symptoms - A Potential Pathway To Early DiagnosisDevi Debora TakimaiNo ratings yet
- 10 1093@rheumatology@kez041Document10 pages10 1093@rheumatology@kez041afrilia.iNo ratings yet
- Sepsis y Shock Septico en NiñosDocument55 pagesSepsis y Shock Septico en NiñosRonald FernandezNo ratings yet
- PIIS0190962220305661Document3 pagesPIIS0190962220305661Roxanne KapNo ratings yet
- PIIS0190962221020739Document2 pagesPIIS0190962221020739Roxanne KapNo ratings yet
- Acad Dermatol Venereol - 2021 - Gambichler - Cutaneous Findings Following COVID 19 Vaccination Review of World LiteratureDocument9 pagesAcad Dermatol Venereol - 2021 - Gambichler - Cutaneous Findings Following COVID 19 Vaccination Review of World LiteratureRoxanne KapNo ratings yet
- Acad Dermatol Venereol - 2022 - Roth - Safe Administration of Subsequent mRNA COVID 19 Vaccine Doses Following A PossibleDocument4 pagesAcad Dermatol Venereol - 2022 - Roth - Safe Administration of Subsequent mRNA COVID 19 Vaccine Doses Following A PossibleRoxanne KapNo ratings yet
- Laser Hair Removal (R. Anderson)Document14 pagesLaser Hair Removal (R. Anderson)Roxanne KapNo ratings yet
- Syphilis Module OnlineDocument68 pagesSyphilis Module OnlineRoxanne KapNo ratings yet
- Hazard Identification Risk Assessment and Risk Control Register HIRARC Review / Revision Control SheetDocument38 pagesHazard Identification Risk Assessment and Risk Control Register HIRARC Review / Revision Control Sheetusman4428No ratings yet
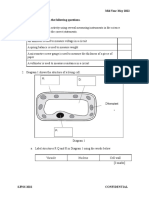
- F2 Mid-Year Exam Section BDocument3 pagesF2 Mid-Year Exam Section BAnne Marian Anak JOSEPHNo ratings yet
- Study of These Parasitic Worms and Their Medical ConsequenceDocument33 pagesStudy of These Parasitic Worms and Their Medical Consequenceabel semuNo ratings yet
- Design For Elderly Drivers and Signal TimingDocument19 pagesDesign For Elderly Drivers and Signal TimingMigz EscutinNo ratings yet
- Report No. 11 of 2023 - PA On PMJAY - English PDF A 064d22bab2b83b5.38721048Document168 pagesReport No. 11 of 2023 - PA On PMJAY - English PDF A 064d22bab2b83b5.38721048arish.khanNo ratings yet
- Lois's ResumeDocument1 pageLois's ResumeloistetteyNo ratings yet
- EXT - 230914 - 0850 - MS32 - V001 - BMW15.10 - SYN - QA - MS - 0032 - 01-ESD CoatingDocument13 pagesEXT - 230914 - 0850 - MS32 - V001 - BMW15.10 - SYN - QA - MS - 0032 - 01-ESD CoatingТамер БакировNo ratings yet
- A Comparison Between Conventional and Digital Radiography in Root Canal Working Length DeterminationDocument6 pagesA Comparison Between Conventional and Digital Radiography in Root Canal Working Length DeterminationGede AnjasmaraNo ratings yet
- Acute Respiratory Distress SyndromeDocument17 pagesAcute Respiratory Distress SyndromeSanjeet Sah100% (1)
- Wa0006Document24 pagesWa0006Saheli Mandal MitraNo ratings yet
- Hearing ImpairmentDocument13 pagesHearing ImpairmentNicoletteReinPererasNo ratings yet
- Different Abilities Associated With Intelligence Test: Cristine Lae C. ErasgaDocument10 pagesDifferent Abilities Associated With Intelligence Test: Cristine Lae C. ErasgaDaisyNo ratings yet
- Module 3 WorksheetDocument6 pagesModule 3 Worksheetemje torrionNo ratings yet
- The Nutritional Properties of Mushrooms: Button MushroomDocument1 pageThe Nutritional Properties of Mushrooms: Button MushroomMarcelApostolacheNo ratings yet
- Nurs FPX 4010 Assessment 1 Collaboration and Leadership Reflection VideoDocument7 pagesNurs FPX 4010 Assessment 1 Collaboration and Leadership Reflection Videojoohnsmith070No ratings yet
- CF Exemplar NURS-FPX4020 Assessment 4Document13 pagesCF Exemplar NURS-FPX4020 Assessment 4Sabahat BashirNo ratings yet
- Interpretation of Liver Function Test in Ayurveda-2Document4 pagesInterpretation of Liver Function Test in Ayurveda-2tasmitadas9101No ratings yet
- Module 6. Unfolding The Emotional SelfDocument16 pagesModule 6. Unfolding The Emotional SelfLeila ParungaoNo ratings yet
- OHS-PR-09-03-F02 RISK ASSESSMENT For INSTALLATION OF WALL MOUNTED JIB CRANEDocument21 pagesOHS-PR-09-03-F02 RISK ASSESSMENT For INSTALLATION OF WALL MOUNTED JIB CRANEmohammed tofiqNo ratings yet
- Exercise For Cardiovascular Disease Prevention and Treatment From Molecular To Clinical Part 1Document320 pagesExercise For Cardiovascular Disease Prevention and Treatment From Molecular To Clinical Part 1Diego CardosoNo ratings yet
- Daftar Barang: PT Pharmacon Ageng AbadiDocument6 pagesDaftar Barang: PT Pharmacon Ageng AbadiApoteker LannyNo ratings yet
- Stein Sept 29 LetterDocument2 pagesStein Sept 29 LetterMitchell BlackNo ratings yet
- The Lingual Liberty System Advantages of A Digital Li - 2018 - Seminars in Orth PDFDocument11 pagesThe Lingual Liberty System Advantages of A Digital Li - 2018 - Seminars in Orth PDFOmy J. CruzNo ratings yet
- QC How To Make A Good Method StatementDocument3 pagesQC How To Make A Good Method StatementRsjBugtongNo ratings yet
- RETRATRUTIDEDocument13 pagesRETRATRUTIDECristobal Alvarado LivacicNo ratings yet
- Drug Study - ClarithromycinDocument2 pagesDrug Study - ClarithromycinTrisha Lapid MatulaNo ratings yet
- Supplementary Online Content: © 2020 American Medical Association. All Rights ReservedDocument19 pagesSupplementary Online Content: © 2020 American Medical Association. All Rights ReservedMai GonzalezNo ratings yet
- 3.hospital RHC Stgs - Federal Government of Somalia PDFDocument200 pages3.hospital RHC Stgs - Federal Government of Somalia PDFFaisal mohammed AbdullahiNo ratings yet