Download as pdf or txt
You might also like
- BCMB 415 Exam 3, Fall 2016 KeyDocument9 pagesBCMB 415 Exam 3, Fall 2016 KeyzzmasterNo ratings yet
- HyperthyroidismDocument38 pagesHyperthyroidismKenPedreso100% (2)
- Transcranial Magnetic StimulationDocument2 pagesTranscranial Magnetic StimulationCandle Shop FullNo ratings yet
- Thyroidectomy: Continuing Education ActivityDocument10 pagesThyroidectomy: Continuing Education Activitybo gum parkNo ratings yet
- Parathyroid Imaging PalestroDocument11 pagesParathyroid Imaging PalestroLadipo Temitope AyodejiNo ratings yet
- Parathyroid Embryology, Anatomy, and Pathophysiology of Primary HyperparathyroidismDocument21 pagesParathyroid Embryology, Anatomy, and Pathophysiology of Primary HyperparathyroidismelizabetioNo ratings yet
- Nihms 1613113Document20 pagesNihms 1613113João GasparNo ratings yet
- Surgical Anatomy of Thyroid and Incidence of Malignancy in Solitary Nodule of ThyroidDocument7 pagesSurgical Anatomy of Thyroid and Incidence of Malignancy in Solitary Nodule of ThyroidFloyd balansagNo ratings yet
- ParathyroidDocument6 pagesParathyroidoluwasujimNo ratings yet
- Parathyroid Gland, Anatom, Histology, and Physiology (A Short Review)Document7 pagesParathyroid Gland, Anatom, Histology, and Physiology (A Short Review)julioNo ratings yet
- Equine Castration AU Vet JournalDocument7 pagesEquine Castration AU Vet JournalYolandi Lewis StoltzNo ratings yet
- Chapter 138neck and Thyroid ExaminationDocument5 pagesChapter 138neck and Thyroid ExaminationAsem Al-domainiNo ratings yet
- 2012 - EAU HypospadiasDocument14 pages2012 - EAU HypospadiastiaraNo ratings yet
- Continuing Education Activity: HypospadiasDocument6 pagesContinuing Education Activity: HypospadiasMaulani Nurlatifah100% (1)
- Histology, Thyroid Gland: July 2020Document14 pagesHistology, Thyroid Gland: July 2020Angelita Torres LlacsahuangaNo ratings yet
- Department of ZoologyDocument27 pagesDepartment of ZoologyAleenaNo ratings yet
- Tiroida Ectopica 1Document8 pagesTiroida Ectopica 1Ionuț RusNo ratings yet
- BS ParatiroidDocument21 pagesBS ParatiroidNo StradamusNo ratings yet
- Full TextDocument8 pagesFull TextFabrício De LamareNo ratings yet
- Moderator: MR S Chirkut /prof Hafejee Commentators:V Pillay / F Joyalemi 5 Sept 2015Document20 pagesModerator: MR S Chirkut /prof Hafejee Commentators:V Pillay / F Joyalemi 5 Sept 2015Kishan Naidu100% (1)
- Para ThyroidDocument41 pagesPara ThyroidAdham YounesNo ratings yet
- Surgical Management of Parathyroid Disease: Endocrine SurgeryDocument7 pagesSurgical Management of Parathyroid Disease: Endocrine SurgeryNiatazya Mumtaz SagitaNo ratings yet
- ArtDocument11 pagesArtkarla QuinteroNo ratings yet
- CriptorchidsmDocument9 pagesCriptorchidsmemirilejlaNo ratings yet
- Operative Surgery ManualDocument273 pagesOperative Surgery Manualvikeshramkelawon8422100% (1)
- Male Reproductive SystemDocument10 pagesMale Reproductive SystemMox SwanNo ratings yet
- AEMV ProceedingDocument25 pagesAEMV ProceedingOrasanu Cristian100% (1)
- C10 Endocrine SystemDocument24 pagesC10 Endocrine Systemwajomi100% (1)
- Safe Female CircumcisionDocument51 pagesSafe Female Circumcisiond7rqqrk+vaii68100% (1)
- Parathyroid Glands: DR Priyanka ShastriDocument70 pagesParathyroid Glands: DR Priyanka ShastriNo StradamusNo ratings yet
- Salivary GlandsDocument26 pagesSalivary GlandssinNo ratings yet
- Pituitary GlandDocument66 pagesPituitary GlandAsmita BhattNo ratings yet
- Thyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneDocument41 pagesThyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneEsther AumaNo ratings yet
- ThyroidectomyDocument5 pagesThyroidectomyAmelee Ting YuNo ratings yet
- Ce (Ra1) F (T) PF1 (Swak)Document2 pagesCe (Ra1) F (T) PF1 (Swak)Darpan DadheechNo ratings yet
- Sarnelli 1980Document18 pagesSarnelli 1980vernadskyiNo ratings yet
- الدرقDocument10 pagesالدرقmas2k212No ratings yet
- Ectopic Thyroid: Etiology, Pathology and Management: ReviewDocument9 pagesEctopic Thyroid: Etiology, Pathology and Management: ReviewIonuț RusNo ratings yet
- Thyroid GlandDocument48 pagesThyroid GlandAnonymous BzS0RF1qyNo ratings yet
- Rare Congenital Genitourinary AnomaliesDocument27 pagesRare Congenital Genitourinary Anomaliesد. محمد عبد الباقي فهميNo ratings yet
- ThyroidDocument22 pagesThyroidTejas HankareNo ratings yet
- HistologyThyroidGland StatPearls NCBIBookshelf 1Document14 pagesHistologyThyroidGland StatPearls NCBIBookshelf 1Mohammed FaragNo ratings yet
- Presentation AnatomyDocument16 pagesPresentation AnatomyChaudryNomiNo ratings yet
- CASE REPORT - CA Tiroid Aldi - ProofreadDocument11 pagesCASE REPORT - CA Tiroid Aldi - ProofreadAldy BimaNo ratings yet
- The Endocrine System Path - Week 3Document11 pagesThe Endocrine System Path - Week 3joatasouzaNo ratings yet
- ThyroidectomyDocument38 pagesThyroidectomyMaria Paula BungayNo ratings yet
- Lobulated Spleen With A Fissure On Diaphragmatic Surface: RD RDDocument7 pagesLobulated Spleen With A Fissure On Diaphragmatic Surface: RD RDShantu ShirurmathNo ratings yet
- Current Concepts in The Management of Primary HypeDocument9 pagesCurrent Concepts in The Management of Primary Hypeoki harisandiNo ratings yet
- Anatomy of ParathyroidDocument2 pagesAnatomy of ParathyroidNnanyelugo AdaobiNo ratings yet
- Art 1Document4 pagesArt 1Claudia IrimieNo ratings yet
- The Avian Endocrine System: April 2008Document12 pagesThe Avian Endocrine System: April 2008MaheshyepuriNo ratings yet
- 10 5923 J Medicine 20200901 03Document5 pages10 5923 J Medicine 20200901 03Emanuel CandelasNo ratings yet
- Adrenal Gland Disease in Ferrets: Elisabeth Simone-Freilicher, DVM, DABVP-AvianDocument13 pagesAdrenal Gland Disease in Ferrets: Elisabeth Simone-Freilicher, DVM, DABVP-AvianGabriel MendesNo ratings yet
- By-Dr - Desh Deepak Ladia JR Iii Radiation Oncology SaimsDocument57 pagesBy-Dr - Desh Deepak Ladia JR Iii Radiation Oncology SaimsAttaufiq IrawanNo ratings yet
- CT Public v82 8 9Document2 pagesCT Public v82 8 9Dida HermaNo ratings yet
- Classification of Vaginal Epithelial CellsDocument14 pagesClassification of Vaginal Epithelial CellsShinta PuspitasariNo ratings yet
- Anatomy and Physiology of The Thyroid and Parathyroid GlandsDocument14 pagesAnatomy and Physiology of The Thyroid and Parathyroid GlandsSidiq AboobakerNo ratings yet
- Undescended TestisDocument66 pagesUndescended TestisalaaNo ratings yet
- Neck MassesDocument52 pagesNeck MassesRaman Prasad SharmaNo ratings yet
- Kondert2017 Medicina Reprodutiva ChinchilaDocument20 pagesKondert2017 Medicina Reprodutiva ChinchilaJoão Gabriel M. AlkmimNo ratings yet
- Thyroid Encyclopedia: Encyclopedia of Thyroid Disease, Thyroid Conditions and Thyroid CancerFrom EverandThyroid Encyclopedia: Encyclopedia of Thyroid Disease, Thyroid Conditions and Thyroid CancerNo ratings yet
- Parotidectomia - UpToDate 2022Document2 pagesParotidectomia - UpToDate 2022juanrangoneNo ratings yet
- Parathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022Document42 pagesParathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- Glandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.Document2 pagesGlandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.juanrangoneNo ratings yet
- Intraoperative Parathyroid Hormone Assays - Uptodate 2022Document18 pagesIntraoperative Parathyroid Hormone Assays - Uptodate 2022juanrangoneNo ratings yet
- Parathyroid Surgery For Inherited Syndromes - Uptodate 2022Document25 pagesParathyroid Surgery For Inherited Syndromes - Uptodate 2022juanrangoneNo ratings yet
- Parathyroidectomy in End-Stage Kidney Disease - Uptodate 2022Document27 pagesParathyroidectomy in End-Stage Kidney Disease - Uptodate 2022juanrangoneNo ratings yet
- 5 Axillary and Epitrochlear Lymph Node Dissection For MelanomaDocument11 pages5 Axillary and Epitrochlear Lymph Node Dissection For MelanomajuanrangoneNo ratings yet
- Preoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022Document22 pagesPreoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- The Attachments of The Breast To The Chest Wall: A Dissection StudyDocument12 pagesThe Attachments of The Breast To The Chest Wall: A Dissection StudyjuanrangoneNo ratings yet
- 23 Inguinofemoral, Iliac-Obturator, and Popliteal Lymphadenectomy For MelanomaDocument19 pages23 Inguinofemoral, Iliac-Obturator, and Popliteal Lymphadenectomy For MelanomajuanrangoneNo ratings yet
- Vandeventer 2016Document10 pagesVandeventer 2016juanrangoneNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangoneNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
- Niveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesDocument1 pageNiveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesjuanrangoneNo ratings yet
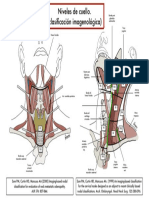
- Clasif Imagenológica Niveles de CuelloDocument1 pageClasif Imagenológica Niveles de CuellojuanrangoneNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document5 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
- 07 Post Mortem Examination (Autopsy)Document48 pages07 Post Mortem Examination (Autopsy)ARIF-UR-REHMAN100% (5)
- Lympathic System TransesDocument9 pagesLympathic System TransesMonica SabarreNo ratings yet
- Heart, Nerve and Mucsle, Membrane Transport Mcqs With KeyDocument8 pagesHeart, Nerve and Mucsle, Membrane Transport Mcqs With KeyMudassar Roomi100% (7)
- Digestion Test BiologyDocument3 pagesDigestion Test BiologyKatrīna SimanovskaNo ratings yet
- Unit 8Document11 pagesUnit 8FatmawatiNo ratings yet
- Gastric AcidDocument15 pagesGastric AcidCaressa Marie EstradaNo ratings yet
- (S) Digestive SystemDocument31 pages(S) Digestive SystemRehanNo ratings yet
- Hyperthyroidism and HypothyroidismDocument59 pagesHyperthyroidism and HypothyroidismJun AmaroNo ratings yet
- Diagnostic Approach To The Patient With Newly Identified Chronic Kidney DiseaseDocument1 pageDiagnostic Approach To The Patient With Newly Identified Chronic Kidney DiseaseLauraNo ratings yet
- Psychological and Neural Mechanisms of The Affective Dimension of PainDocument4 pagesPsychological and Neural Mechanisms of The Affective Dimension of PainJulian GorositoNo ratings yet
- Case of AmoebiasisDocument100 pagesCase of Amoebiasisglenn guanzonNo ratings yet
- Oyungu BrainDocument17 pagesOyungu BrainElvis KiprotichNo ratings yet
- Liver Transplantation: What Is Liver Transplantation? Who Needs A Liver Transplant?Document12 pagesLiver Transplantation: What Is Liver Transplantation? Who Needs A Liver Transplant?RatihSeptianiNo ratings yet
- Chapter 39 AntihypertensivesDocument4 pagesChapter 39 AntihypertensivesErika Joy Cabison TamayoNo ratings yet
- Pyloric StenosisDocument46 pagesPyloric Stenosishayssam rashwan81% (16)
- 1-Basic Concepts of Electrophysical Agents 1Document41 pages1-Basic Concepts of Electrophysical Agents 1Faiz HadiNo ratings yet
- Pathophysiology of HypertensionDocument14 pagesPathophysiology of HypertensionRessy HastoprajaNo ratings yet
- Chapter 10 - Immune Responses Against Tumors and TransplantsDocument11 pagesChapter 10 - Immune Responses Against Tumors and TransplantsFYMNo ratings yet
- Thyroid GlandDocument10 pagesThyroid GlandSheena Mae Atienza100% (2)
- Bingswati Mukherjee 09-11-16Document2 pagesBingswati Mukherjee 09-11-16Arka Prava PaulNo ratings yet
- Circulatory System FKM'12Document55 pagesCirculatory System FKM'12muhammadsudrajadNo ratings yet
- Yanzlee P. Ananayo Grade 4-Bl. Sandor Science 4 Laboratory Activity #2 How Is Different Food Digested?Document3 pagesYanzlee P. Ananayo Grade 4-Bl. Sandor Science 4 Laboratory Activity #2 How Is Different Food Digested?Marvin SalvadorNo ratings yet
- Review Article: Relevant Biliary Anatomy During CholecystectomyDocument11 pagesReview Article: Relevant Biliary Anatomy During CholecystectomyAbrar SabawiNo ratings yet
- Previous Year'S Questions (Excretion)Document1 pagePrevious Year'S Questions (Excretion)veeresh punjaniNo ratings yet
- Digestive System: Submitted By: Caimoso, Tricia Ann D. Quiambao, Aliyah Lourdes D. Bs Psychology 3-3Document9 pagesDigestive System: Submitted By: Caimoso, Tricia Ann D. Quiambao, Aliyah Lourdes D. Bs Psychology 3-3Tricia Ann CaimosoNo ratings yet
- Neftali de La Cruz EmeterioDocument2 pagesNeftali de La Cruz EmeterioNeftali EmeterioNo ratings yet
- Acute Interstitial NephritisDocument36 pagesAcute Interstitial NephritisosaqerNo ratings yet
- Acute GlomerulonephritisDocument18 pagesAcute GlomerulonephritisdanielaNo ratings yet