Download as pdf or txt
You might also like
- BCMB 415 Exam 3, Fall 2016 KeyDocument9 pagesBCMB 415 Exam 3, Fall 2016 KeyzzmasterNo ratings yet
- Digestive and Endocrine Systems: Chapter TestDocument5 pagesDigestive and Endocrine Systems: Chapter TestJunior SencionNo ratings yet
- 2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentDocument9 pages2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentCharley WangNo ratings yet
- Indications For Thyroid Surgeryexperience of The Ent Departmentof Moulay Ismail Military Hospital in Meknes (About 103 Cases)Document8 pagesIndications For Thyroid Surgeryexperience of The Ent Departmentof Moulay Ismail Military Hospital in Meknes (About 103 Cases)IJAR JOURNALNo ratings yet
- Treatment Outcome of Total Thyroidectomy For Multinodular GoiterDocument5 pagesTreatment Outcome of Total Thyroidectomy For Multinodular GoiterAngga ToragarryNo ratings yet
- Ying Li 2016Document8 pagesYing Li 2016Bogdan TrandafirNo ratings yet
- Multiple Endocrine Neoplasia Type 1 - Endotext - NCBI BookshelfDocument16 pagesMultiple Endocrine Neoplasia Type 1 - Endotext - NCBI BookshelfEszter KardosNo ratings yet
- Parathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022Document42 pagesParathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- HandbookDocument4 pagesHandbookDr Venkatachalapathy T S Ped SurgeonNo ratings yet
- Multiple Endocrine Neoplasia Type 1 - Clinical Manifestations and Diagnosis - UpToDateDocument9 pagesMultiple Endocrine Neoplasia Type 1 - Clinical Manifestations and Diagnosis - UpToDateverawoNo ratings yet
- Preoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022Document22 pagesPreoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- Authors: Section Editor: Deputy EditorDocument37 pagesAuthors: Section Editor: Deputy Editorbo gum parkNo ratings yet
- Benign Multinodular Goiter: A. Frilling, C. Liu, F. WeberDocument4 pagesBenign Multinodular Goiter: A. Frilling, C. Liu, F. WeberPrince AliNo ratings yet
- Thyroidectomy - UpToDateDocument65 pagesThyroidectomy - UpToDateDanya BarbozaNo ratings yet
- Initial Management of High-Risk Gestational Trophoblastic Neoplasia - UpToDateDocument28 pagesInitial Management of High-Risk Gestational Trophoblastic Neoplasia - UpToDateAlejandro DiezNo ratings yet
- TR VS Minimamente InvasivaDocument5 pagesTR VS Minimamente Invasivamanuel barrientosNo ratings yet
- Jurnal Efusi Pleura MalignaDocument12 pagesJurnal Efusi Pleura MalignaAsyraf HabibieNo ratings yet
- Ectopic PregnancyDocument7 pagesEctopic PregnancyAlex BelinschiiNo ratings yet
- Journal Reading - Pituitary AdenomasDocument3 pagesJournal Reading - Pituitary AdenomasKian HerreraNo ratings yet
- Medicina: Hemithyroidectomy For Thyroid Cancer: A ReviewDocument12 pagesMedicina: Hemithyroidectomy For Thyroid Cancer: A ReviewaisyahNo ratings yet
- Mic Coli 2017Document6 pagesMic Coli 2017Orlando CervantesNo ratings yet
- Worldwide Trends in Surgical Techniques in The Treatment of Esophageal and Gastroesophageal Junction CancerDocument7 pagesWorldwide Trends in Surgical Techniques in The Treatment of Esophageal and Gastroesophageal Junction CancerLuca BellaioNo ratings yet
- Multiple Endocrine NeoplasiaDocument40 pagesMultiple Endocrine Neoplasiamedical chroniclesNo ratings yet
- Cancers 14 03845Document15 pagesCancers 14 03845regigaby02No ratings yet
- Vipoma CompleteDocument154 pagesVipoma CompleteTei OcampoNo ratings yet
- Anesthesia For Transsphenoidal Pituitary Surgery.Document6 pagesAnesthesia For Transsphenoidal Pituitary Surgery.ismaelNo ratings yet
- European Guidelines On Perioperative Venous.11Document5 pagesEuropean Guidelines On Perioperative Venous.11ionut.andruscaNo ratings yet
- Ahmed 2011Document10 pagesAhmed 2011skribekbenjaminNo ratings yet
- Clinicopathological Correlates of HyperparathyroidismDocument18 pagesClinicopathological Correlates of HyperparathyroidismmaryNo ratings yet
- Wilm's Tumor Powerpoint MMDocument36 pagesWilm's Tumor Powerpoint MMWai GyiNo ratings yet
- Primary Hyperparathyroidism 1Document16 pagesPrimary Hyperparathyroidism 1Marco MenesesNo ratings yet
- Workup of Well-Differentiated Thyroid Carcinoma: Cristian M. Slough, MD, and Gregory W. Randolph, MDDocument7 pagesWorkup of Well-Differentiated Thyroid Carcinoma: Cristian M. Slough, MD, and Gregory W. Randolph, MDELinkTulusNo ratings yet
- Tumori EndocrineDocument900 pagesTumori EndocrineFlorin Calin LungNo ratings yet
- Author: Section Editor: Deputy EditorDocument29 pagesAuthor: Section Editor: Deputy EditorSpital PneumoNo ratings yet
- Pheochromocytomas in Pediatric Surgery A Case ReportDocument2 pagesPheochromocytomas in Pediatric Surgery A Case Reportreza kurniawanNo ratings yet
- EMA/CO Regimen in High-Risk Gestational Trophoblastic Tumor (GTT)Document6 pagesEMA/CO Regimen in High-Risk Gestational Trophoblastic Tumor (GTT)Vidho El RiveraNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyMeriam MalindaNo ratings yet
- Predictive Value of Nodal Metastases On Local Recurrence in The Management of Differentiated Thyroid Cancer. Retrospective Clinical StudyDocument6 pagesPredictive Value of Nodal Metastases On Local Recurrence in The Management of Differentiated Thyroid Cancer. Retrospective Clinical StudyuqbaNo ratings yet
- Laparoscopic Resection of Pancreatic Neuroendocrine TumorsDocument10 pagesLaparoscopic Resection of Pancreatic Neuroendocrine TumorsWahyudi Permana DarlisNo ratings yet
- What Happens in A 5-Year Follow-Up of Benign Thyroid NodulesDocument4 pagesWhat Happens in A 5-Year Follow-Up of Benign Thyroid NodulesT.A.BNo ratings yet
- EcheverríaSepúlveda2022 Article TheUndescendedTestisInChildrenDocument11 pagesEcheverríaSepúlveda2022 Article TheUndescendedTestisInChildrenMELVIN JOHNNo ratings yet
- Pheochromocytomas in Pediatric Surgery A Case ReportDocument2 pagesPheochromocytomas in Pediatric Surgery A Case Reportreza kurniawanNo ratings yet
- Gs 10 03 1135Document12 pagesGs 10 03 1135Ashu AberaNo ratings yet
- Glandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.Document2 pagesGlandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.juanrangoneNo ratings yet
- Epithelial To Mesenchymal Transition and Cell Biology of Molecular Regulation in Endometrial CarcinogenesisDocument17 pagesEpithelial To Mesenchymal Transition and Cell Biology of Molecular Regulation in Endometrial CarcinogenesisMelati HasnailNo ratings yet
- Surgical Approach To Hysterectomy For Benign Gynaecological DiseaseDocument19 pagesSurgical Approach To Hysterectomy For Benign Gynaecological DiseasebambangtrionocNo ratings yet
- CorreaDocument7 pagesCorreasandyrraoNo ratings yet
- Chapter 14A Pituitary Adenomas and CraniopharyngiomasDocument8 pagesChapter 14A Pituitary Adenomas and CraniopharyngiomasMohammad Ali IsmailNo ratings yet
- What Is The Diagnosis?Document2 pagesWhat Is The Diagnosis?Mel ObisNo ratings yet
- Pheochromocytoma: Pheochromocytoma: The Facts You Need To KnowDocument5 pagesPheochromocytoma: Pheochromocytoma: The Facts You Need To KnowadityaNo ratings yet
- 2023 1840 OnlinePDFDocument7 pages2023 1840 OnlinePDFjuhiNo ratings yet
- Management and Complications of Tubo-Ovarian Abscess - UpToDateDocument19 pagesManagement and Complications of Tubo-Ovarian Abscess - UpToDateAnne Lorraine BringasNo ratings yet
- Practice Essentials: Signs and SymptomsDocument20 pagesPractice Essentials: Signs and SymptomsrainbowshopNo ratings yet
- Completion Thyroidectomy: Predicting Bilateral Disease: Originalresearcharticle Open AccessDocument7 pagesCompletion Thyroidectomy: Predicting Bilateral Disease: Originalresearcharticle Open AccessRadita Dwihaning PutriNo ratings yet
- 10 1016@j Beem 2019 101290Document22 pages10 1016@j Beem 2019 101290Alirio Angulo QuinteroNo ratings yet
- Medical Therapy: Radical NephrectomyDocument4 pagesMedical Therapy: Radical Nephrectomychuckydoll1989No ratings yet
- Follow-Up of DTC - What Should (And What Should Not) Be DoneDocument14 pagesFollow-Up of DTC - What Should (And What Should Not) Be DoneYulius DonyNo ratings yet
- Hemithyroidectomy Papillary Thyroid Carcinoma in Low Risk Group PatientsDocument5 pagesHemithyroidectomy Papillary Thyroid Carcinoma in Low Risk Group PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Thesis UrologyDocument5 pagesThesis Urologydeepjonesmanchester100% (2)
- Mr. Para's Case Study-For Mam ZenDocument191 pagesMr. Para's Case Study-For Mam ZenWestly JucoNo ratings yet
- Management of Peritoneal Metastases- Cytoreductive Surgery, HIPEC and BeyondFrom EverandManagement of Peritoneal Metastases- Cytoreductive Surgery, HIPEC and BeyondAditi BhattNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- Parotidectomia - UpToDate 2022Document2 pagesParotidectomia - UpToDate 2022juanrangoneNo ratings yet
- Parathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022Document42 pagesParathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- Glandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.Document2 pagesGlandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.juanrangoneNo ratings yet
- Intraoperative Parathyroid Hormone Assays - Uptodate 2022Document18 pagesIntraoperative Parathyroid Hormone Assays - Uptodate 2022juanrangoneNo ratings yet
- Surgical Anatomy of The Parathyroid Glands - Uptodate 2022Document8 pagesSurgical Anatomy of The Parathyroid Glands - Uptodate 2022juanrangoneNo ratings yet
- Parathyroidectomy in End-Stage Kidney Disease - Uptodate 2022Document27 pagesParathyroidectomy in End-Stage Kidney Disease - Uptodate 2022juanrangoneNo ratings yet
- 5 Axillary and Epitrochlear Lymph Node Dissection For MelanomaDocument11 pages5 Axillary and Epitrochlear Lymph Node Dissection For MelanomajuanrangoneNo ratings yet
- Preoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022Document22 pagesPreoperative Localization For Parathyroid Surgery in Patients With Primary Hyperparathyroidism - Uptodate 2022juanrangoneNo ratings yet
- The Attachments of The Breast To The Chest Wall: A Dissection StudyDocument12 pagesThe Attachments of The Breast To The Chest Wall: A Dissection StudyjuanrangoneNo ratings yet
- 23 Inguinofemoral, Iliac-Obturator, and Popliteal Lymphadenectomy For MelanomaDocument19 pages23 Inguinofemoral, Iliac-Obturator, and Popliteal Lymphadenectomy For MelanomajuanrangoneNo ratings yet
- Vandeventer 2016Document10 pagesVandeventer 2016juanrangoneNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangoneNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
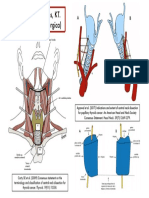
- Niveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesDocument1 pageNiveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesjuanrangoneNo ratings yet
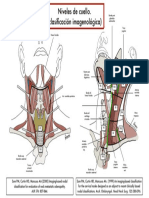
- Clasif Imagenológica Niveles de CuelloDocument1 pageClasif Imagenológica Niveles de CuellojuanrangoneNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document5 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
- Lympathic System TransesDocument9 pagesLympathic System TransesMonica SabarreNo ratings yet
- Investigation of The Effects of Selected Activities Onsecretion of Serotonin Hormone and Some Other HormonesDocument34 pagesInvestigation of The Effects of Selected Activities Onsecretion of Serotonin Hormone and Some Other HormonesGökhan DoğanNo ratings yet
- Liver FibrosisDocument29 pagesLiver FibrosisAmira HelayelNo ratings yet
- Cara Membaca Foto Thoraks Yang BaikDocument2 pagesCara Membaca Foto Thoraks Yang BaikIdi Nagan RayaNo ratings yet
- Respon UroDocument20 pagesRespon UroNurul FajrinaNo ratings yet
- Mod 8 ZooDocument10 pagesMod 8 ZooLM Tricia T. DE LA CRUZNo ratings yet
- Anatomy of Hepatobiliary SystemDocument46 pagesAnatomy of Hepatobiliary SystemAyu Tiara FitriNo ratings yet
- 7.reflex Regulation of Physiological Function PDFDocument2 pages7.reflex Regulation of Physiological Function PDFNektarios TsakalosNo ratings yet
- Adrenal Gland Physiology (DRDocument77 pagesAdrenal Gland Physiology (DRapi-3769252100% (4)
- Psychological and Neural Mechanisms of The Affective Dimension of PainDocument4 pagesPsychological and Neural Mechanisms of The Affective Dimension of PainJulian GorositoNo ratings yet
- Circulatory System PPT - 2022Document94 pagesCirculatory System PPT - 2022Eugene Osei AmoakoNo ratings yet
- Gastrointestinal Anatomy and PhysiologyDocument85 pagesGastrointestinal Anatomy and Physiologyrowenaabante100% (3)
- Chapter 10 - Immune Responses Against Tumors and TransplantsDocument11 pagesChapter 10 - Immune Responses Against Tumors and TransplantsFYMNo ratings yet
- Presentation BreastDocument17 pagesPresentation Breastmayeth galeraNo ratings yet
- Fundamentals of Urine & Body Fluid Analysis 5th Edition 2023 ALGRAWANYDocument461 pagesFundamentals of Urine & Body Fluid Analysis 5th Edition 2023 ALGRAWANYDr-Issam IrakNo ratings yet
- Drugs Affecting The Endocrine SystemDocument3 pagesDrugs Affecting The Endocrine SystemJerica Jaz F. VergaraNo ratings yet
- Oyungu BrainDocument17 pagesOyungu BrainElvis KiprotichNo ratings yet
- Clinical Presentation of Renal Disease: Persistent Urinary AbnormalitiesDocument27 pagesClinical Presentation of Renal Disease: Persistent Urinary AbnormalitiesradhiinathahirNo ratings yet
- Pex 09 01Document5 pagesPex 09 01Gerardien Elham AfifahNo ratings yet
- -renalเ -adrenalเ -aortaเ: FeverDocument4 pages-renalเ -adrenalเ -aortaเ: FeverWipaporn ChaengsriNo ratings yet
- (Lib-Ebooks Com) 0207202122145Document458 pages(Lib-Ebooks Com) 0207202122145Stefan Bauman100% (2)
- Addison's Disease:-: SymptomsDocument2 pagesAddison's Disease:-: SymptomsIjaz KhanNo ratings yet
- Subcortical 1Document46 pagesSubcortical 1IRSHAD SHAN KNo ratings yet
- Introduction To Brain Anatomy: Wieslaw L. NowinskiDocument37 pagesIntroduction To Brain Anatomy: Wieslaw L. NowinskiAditya Rama DevaraNo ratings yet
- Gastric AcidDocument15 pagesGastric AcidCaressa Marie EstradaNo ratings yet
- Guia Anatomia TerminadaDocument120 pagesGuia Anatomia TerminadaAlex ZuritaNo ratings yet
- PHC411 - Practical 3 - Oct 2021 - StudentsDocument14 pagesPHC411 - Practical 3 - Oct 2021 - StudentsALISYA SOPHIA MOHAMMAD ABU SHAHID CHRISNo ratings yet
- Treatment of Pituitary Adenoma by Traditional Medicine TherapiesDocument3 pagesTreatment of Pituitary Adenoma by Traditional Medicine TherapiesPirasan Traditional Medicine CenterNo ratings yet