Download as docx, pdf, or txt
You might also like
- Skill 15-6 Administering A Subcutaneous InjectionDocument2 pagesSkill 15-6 Administering A Subcutaneous InjectionMitul Peter100% (3)
- Ferosac InjDocument2 pagesFerosac InjMohamed Taleb75% (4)
- Nclex ReviewerDocument108 pagesNclex ReviewerKatrina Blancaver Nopuente100% (12)
- Merck Vitamin K Package Insert - Aquamephyton PIDocument5 pagesMerck Vitamin K Package Insert - Aquamephyton PIDonna100% (10)
- Nurse ResumeDocument4 pagesNurse ResumeBuddhi EkanayakaNo ratings yet
- Administering Z-Track Injection: Prepared By: Paul Allen Gabriel R. Tablico, RN, ManDocument9 pagesAdministering Z-Track Injection: Prepared By: Paul Allen Gabriel R. Tablico, RN, ManJamesClaveriaNo ratings yet
- Drug Preparation: (Ampule and Vial)Document25 pagesDrug Preparation: (Ampule and Vial)Ron Lucernas MayugaNo ratings yet
- Administering Intradermal InjectionDocument17 pagesAdministering Intradermal InjectionPattNo ratings yet
- Parenteral Medication: Prepared By: Level II InstructorsDocument105 pagesParenteral Medication: Prepared By: Level II InstructorsJayrelle D. SafranNo ratings yet
- Intramuscular Injectoin ChecklistDocument2 pagesIntramuscular Injectoin ChecklistBettina ChuaNo ratings yet
- Admin An IM InjectionsDocument2 pagesAdmin An IM InjectionsjepoiNo ratings yet
- Parenteral Catheterization Enema ChecklistDocument8 pagesParenteral Catheterization Enema ChecklistJessoliver GalvezNo ratings yet
- IM and ID Injection ChecklistsDocument2 pagesIM and ID Injection ChecklistsChesca LayosaNo ratings yet
- PARENTERAL MEDICATION Manual and Checklist 1Document14 pagesPARENTERAL MEDICATION Manual and Checklist 1Hazel Shaine BaybayanNo ratings yet
- PERFORMANCE CRITERIA CHECKLIST Oral Otic Optic Parenteral Drug AdministrationDocument3 pagesPERFORMANCE CRITERIA CHECKLIST Oral Otic Optic Parenteral Drug AdministrationRayzl GacayanNo ratings yet
- OSCE ReviewerDocument17 pagesOSCE Reviewerminangsung minangnengNo ratings yet
- Intra D-InjectionDocument2 pagesIntra D-InjectionAbby Trisha MadularaNo ratings yet
- Intra M-InjectionDocument4 pagesIntra M-InjectionAbby Trisha MadularaNo ratings yet
- RD For Id, Im, ChivDocument6 pagesRD For Id, Im, ChivPrincess Huey GreyNo ratings yet
- RD - MedicationsDocument15 pagesRD - MedicationsJiwi YuNo ratings yet
- Kami Export ID IM SC NewDocument104 pagesKami Export ID IM SC NewJayrelle D. SafranNo ratings yet
- ID-IM-SQ-E ToolDocument9 pagesID-IM-SQ-E TooltriciacamilleNo ratings yet
- Adminstration of Intramusclar InjectionDocument3 pagesAdminstration of Intramusclar InjectionDenise CastroNo ratings yet
- Administering Parental MedicationsDocument4 pagesAdministering Parental MedicationsAmanda Joy TuizaNo ratings yet
- Preparing and Administering Subcutaneous Injection PurposeDocument11 pagesPreparing and Administering Subcutaneous Injection PurposeLRBNo ratings yet
- Administering A Subcutaneous InjectionDocument2 pagesAdministering A Subcutaneous InjectionLiana Koh VillanuevaNo ratings yet
- Administering An Intradermal InjectionDocument2 pagesAdministering An Intradermal InjectionKrysstal GerongaNo ratings yet
- Performing Neonatal Suctioning 1Document2 pagesPerforming Neonatal Suctioning 1SharNo ratings yet
- 2 Intramuscular InjectionDocument5 pages2 Intramuscular InjectionKEANNA ZURRIAGANo ratings yet
- Mark King Joseph P. Cordovilla - Mid1a - CP100 - Module 9Document5 pagesMark King Joseph P. Cordovilla - Mid1a - CP100 - Module 9Mark king Joseph CordovillaNo ratings yet
- Sajo College of Nursing Sciences Birnin Kebbi, Kebbi State: Unit IxDocument22 pagesSajo College of Nursing Sciences Birnin Kebbi, Kebbi State: Unit IxyusufNo ratings yet
- (Bio 024) Lab Activity 12 - BloodDocument7 pages(Bio 024) Lab Activity 12 - BloodJelleane Paja TaoataoNo ratings yet
- Skill Labs, Clinical History Taking, and ExaminationDocument84 pagesSkill Labs, Clinical History Taking, and ExaminationJoo Se HyukNo ratings yet
- SL PNCM 1079 Administering An Intramuscular InjectionDocument3 pagesSL PNCM 1079 Administering An Intramuscular Injectionpreciouslagundi226No ratings yet
- Uf Health Pathology Laboratories Venipuncture ProcedureDocument6 pagesUf Health Pathology Laboratories Venipuncture ProcedureMikyla CorpuzNo ratings yet
- Parenteral PRDocument4 pagesParenteral PRGlecy CastañaresNo ratings yet
- Parenteral Administration - ChecklistDocument4 pagesParenteral Administration - ChecklistKeila RosalesNo ratings yet
- Procedure Checklist DrugDocument4 pagesProcedure Checklist DrugAllysa D.R RemosNo ratings yet
- Intramuscular InjectionDocument2 pagesIntramuscular InjectionBARANGAY ANIBAN 2100% (1)
- Id Im SCDocument104 pagesId Im SCEunice CameroNo ratings yet
- Intramuscular InjectionDocument10 pagesIntramuscular InjectionGheorghe HotaranNo ratings yet
- Procedural Checklist For Tracheostomy CareDocument6 pagesProcedural Checklist For Tracheostomy CareAbegail TabuniagNo ratings yet
- Parenteral-Administration IM IDDocument2 pagesParenteral-Administration IM IDcarlomonteclaro335No ratings yet
- Name: - Caring For A Patient On Isolation PrecautionDocument5 pagesName: - Caring For A Patient On Isolation PrecautionLarr SumalpongNo ratings yet
- Observation Competence Checklist For Administration of An Intramuscular InjectionDocument24 pagesObservation Competence Checklist For Administration of An Intramuscular InjectionNada S'jNo ratings yet
- Administering An Intramuscular InjectionDocument3 pagesAdministering An Intramuscular InjectionPattNo ratings yet
- Using Prepackaged Sterile KitDocument14 pagesUsing Prepackaged Sterile KitHannaNo ratings yet
- IV ChecklistDocument27 pagesIV ChecklistKyle VargasNo ratings yet
- Subcutaneous InjectionsDocument2 pagesSubcutaneous InjectionsIman NamyraNo ratings yet
- Checklist Administering An Intramuscular InjectionDocument3 pagesChecklist Administering An Intramuscular InjectionCAMPOSANO, JHANNA MARIENo ratings yet
- (BIO 024) LAB ACTIVITY 12 - BLOODDocument9 pages(BIO 024) LAB ACTIVITY 12 - BLOODmaggan donnaNo ratings yet
- IM InjectionDocument4 pagesIM InjectionAdrija SenNo ratings yet
- Procedure Checklist Chapter 23: Administering Intramuscular InjectionsDocument3 pagesProcedure Checklist Chapter 23: Administering Intramuscular InjectionsLiezel CauilanNo ratings yet
- NUR Tracheostomy Care and Suctioning NUR 113Document2 pagesNUR Tracheostomy Care and Suctioning NUR 113anju rachel joseNo ratings yet
- Routine Venipuncture GuidelinesDocument6 pagesRoutine Venipuncture GuidelinesAndleeb AshrafNo ratings yet
- Administering MedicationDocument13 pagesAdministering MedicationOfficially RandomNo ratings yet
- Nursing Procedure Checklist: Suctioning An Endotracheal Tube: Open SystemDocument2 pagesNursing Procedure Checklist: Suctioning An Endotracheal Tube: Open Systemmark OrpillaNo ratings yet
- Subcutaneous InjectionsDocument2 pagesSubcutaneous InjectionsIman NamyraNo ratings yet
- 16 Administering Intradermal InjectionsDocument3 pages16 Administering Intradermal InjectionsMarky RoqueNo ratings yet
- Parenteral Medication ScriptDocument6 pagesParenteral Medication ScriptJoanna MontebonNo ratings yet
- Administering An Intramuscular InjectionDocument3 pagesAdministering An Intramuscular Injectionapi-26570979100% (4)
- IntradermalDocument2 pagesIntradermalAdrija SenNo ratings yet
- EMERGENCY CARE FOR BEGINNERS: Essential First Aid Techniques and Tips (2024)From EverandEMERGENCY CARE FOR BEGINNERS: Essential First Aid Techniques and Tips (2024)No ratings yet
- Survival Skills: How to Survive Anything and Anywhere in the World (A Comprehensive Guide to Preparing for and Overcoming Challenges of Earthquakes)From EverandSurvival Skills: How to Survive Anything and Anywhere in the World (A Comprehensive Guide to Preparing for and Overcoming Challenges of Earthquakes)No ratings yet
- Medication Administration in Patients With Swallowing DifficultiesDocument134 pagesMedication Administration in Patients With Swallowing DifficultiesChandan SinghNo ratings yet
- Medical Aesthetics Certificate Understanding The Safe Use of Dermal Fillers in Cosmetic Procedures SpecificationDocument8 pagesMedical Aesthetics Certificate Understanding The Safe Use of Dermal Fillers in Cosmetic Procedures Specificationdocrubes50No ratings yet
- Pil Exoaparin 0.6 MLDocument12 pagesPil Exoaparin 0.6 MLLavictoire ColetteNo ratings yet
- An Approach To Structural Facial Rejuvenation With Fillers in WomenDocument15 pagesAn Approach To Structural Facial Rejuvenation With Fillers in WomenJhon RodriguezNo ratings yet
- Insulin AdministrationDocument15 pagesInsulin Administrationmec17No ratings yet
- 2010Document59 pages2010ejyoung928No ratings yet
- Tetanusimmunoglobulin VFinjDocument9 pagesTetanusimmunoglobulin VFinjMichael Oscarius LoisanjayaNo ratings yet
- Development of An Advanced Injection Time Model For An AutoinjectorDocument10 pagesDevelopment of An Advanced Injection Time Model For An AutoinjectorjuanibirisNo ratings yet
- SJZ 108Document8 pagesSJZ 108Guilherme BergantonNo ratings yet
- Demonstration of Child HealthDocument5 pagesDemonstration of Child HealthAmy Lalringhluani100% (1)
- Compiled Skills LabDocument14 pagesCompiled Skills LabJolaine ValloNo ratings yet
- Important Point To Be Included in HR Project: Claris Lifescience LTDDocument30 pagesImportant Point To Be Included in HR Project: Claris Lifescience LTDMegha HumbalNo ratings yet
- Maxillary Injection TechniquesDocument127 pagesMaxillary Injection TechniquesD YasIr MussaNo ratings yet
- Pediatric Drug AdministrationDocument32 pagesPediatric Drug AdministrationNobleScarletNo ratings yet
- Pharmacokinetics and Pharmacodynamics 40Document40 pagesPharmacokinetics and Pharmacodynamics 40Shoaib BiradarNo ratings yet
- BRP Controlling Worms and Liver Fluke in Cattle 180116 PDFDocument20 pagesBRP Controlling Worms and Liver Fluke in Cattle 180116 PDFAISHWARYNo ratings yet
- Copy-History Taking in Obstetrics&gynaecology MakandaDocument1 pageCopy-History Taking in Obstetrics&gynaecology MakandaAhlam Azam, MohamedNo ratings yet
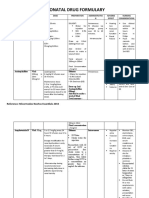
- Neonatal Drug FormularyDocument6 pagesNeonatal Drug FormularyLucian CaelumNo ratings yet
- Appropriate Use of Benzathine Penicillin G For Treatment of SyphilisDocument2 pagesAppropriate Use of Benzathine Penicillin G For Treatment of SyphilisNaela RizqiNo ratings yet
- Medication AdmnistrationDocument34 pagesMedication AdmnistrationAmit MartinNo ratings yet
- VN 130-Clinical Lab I Internal Clinical ExperienceDocument15 pagesVN 130-Clinical Lab I Internal Clinical ExperienceSharon TanveerNo ratings yet
- 8in1 Hydra Facial Mahine User Manual: Model:FQ077-2Document19 pages8in1 Hydra Facial Mahine User Manual: Model:FQ077-2komaill naqviNo ratings yet
- Con 046543Document37 pagesCon 046543Prince AliNo ratings yet
- Anesthesia Onset Time and Injection Pain Between Buffered and Unbuffered Lidocaine Used As Local Anesthetic For Dental Care in ChildrenDocument4 pagesAnesthesia Onset Time and Injection Pain Between Buffered and Unbuffered Lidocaine Used As Local Anesthetic For Dental Care in ChildrenFernando MenesesNo ratings yet
- IA Injection GuideDocument8 pagesIA Injection GuidevetermanNo ratings yet
- Dehydrated AlcoholDocument5 pagesDehydrated AlcoholRodica GrecuNo ratings yet