Download as docx, pdf, or txt
You might also like
- MedSurg Notes - Cancer of The LiverDocument2 pagesMedSurg Notes - Cancer of The LiverMae CeaesarNo ratings yet
- Grand Case NP 1 Laparoscopic CholecystectomyDocument21 pagesGrand Case NP 1 Laparoscopic CholecystectomyFarida Paula R. SevillaNo ratings yet
- Case Study On AmputationDocument13 pagesCase Study On AmputationKristine Dela Pasion100% (2)
- Open Cholecystectomy ReportDocument7 pagesOpen Cholecystectomy ReportjosephcloudNo ratings yet
- CholecystectomyDocument17 pagesCholecystectomyStephanie Joy EscalaNo ratings yet
- Cholecystectomy (: Laparoscopic GallstonesDocument4 pagesCholecystectomy (: Laparoscopic GallstonesAlexia BatungbacalNo ratings yet
- Final EditDocument43 pagesFinal EditMary Rose LinatocNo ratings yet
- Case Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyDocument46 pagesCase Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyAjiMary M. DomingoNo ratings yet
- CholecystectomyDocument8 pagesCholecystectomyApril_Ivy_Raga_3835No ratings yet
- CHOLEDocument25 pagesCHOLEJane TuazonNo ratings yet
- BSN3C 2E Case Presentation On Blunt Abdominal Trauma November 2021Document42 pagesBSN3C 2E Case Presentation On Blunt Abdominal Trauma November 2021Assasination Classroom100% (1)
- Cholecystectomy 4 PrintingDocument19 pagesCholecystectomy 4 PrintingKyle Punzalan100% (2)
- Open Cholecystectomy Case StudyDocument3 pagesOpen Cholecystectomy Case StudyAngela Praz67% (3)
- Case Study About Rectal CADocument11 pagesCase Study About Rectal CACantiga Vhadz0% (1)
- Open CholecystectomyDocument7 pagesOpen CholecystectomyMonique CastroNo ratings yet
- Mastectomy (Case Analysis)Document7 pagesMastectomy (Case Analysis)Lester_Ocuaman_2248No ratings yet
- Modified Radical MastectomyDocument6 pagesModified Radical Mastectomymetch isulatNo ratings yet
- NCP CvaDocument4 pagesNCP CvaMariquita BuenafeNo ratings yet
- Case Study CholecystitisDocument13 pagesCase Study Cholecystitissanthyakunjumon100% (1)
- CVDDocument67 pagesCVDRachel PerandoNo ratings yet
- CHOLECYSTECTOMYDocument35 pagesCHOLECYSTECTOMYfaitheee100% (3)
- Percutaneous Endoscopic GastrostomyDocument27 pagesPercutaneous Endoscopic GastrostomyDoha EbedNo ratings yet
- Acute Lymphocytic LeukemiaDocument12 pagesAcute Lymphocytic Leukemiajustin_saneNo ratings yet
- HernioplastyDocument6 pagesHernioplastyCherry Delos ReyesNo ratings yet
- Pa Tho Physiology of OsteoporosisDocument2 pagesPa Tho Physiology of Osteoporosisjcam_o9No ratings yet
- Cancer Case StudyDocument15 pagesCancer Case StudyRobin HaliliNo ratings yet
- Esophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNDocument20 pagesEsophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNAnn SalvatierraNo ratings yet
- Case Study CholecystitisDocument27 pagesCase Study CholecystitisBandana RajpootNo ratings yet
- Seminar On MastectomyDocument8 pagesSeminar On Mastectomypooja singhNo ratings yet
- Pathophysiology (Client Base) :: Predisposing Factors: Precipitating FactorsDocument1 pagePathophysiology (Client Base) :: Predisposing Factors: Precipitating Factorsleslie_macasaetNo ratings yet
- HNP Case Scenario For Case StudyDocument2 pagesHNP Case Scenario For Case StudyDeinielle Magdangal RomeroNo ratings yet
- Pancretic Cancer Case Study - BurkeDocument52 pagesPancretic Cancer Case Study - Burkeapi-282999254No ratings yet
- NCP - Risk For Other-Directed ViolenceDocument2 pagesNCP - Risk For Other-Directed ViolenceKasandra Dawn Moquia BerisoNo ratings yet
- Acute Appendicitis Group CDocument40 pagesAcute Appendicitis Group CHeart TolenadaNo ratings yet
- Acute Cholecystolithiasis - G4 SB2Document125 pagesAcute Cholecystolithiasis - G4 SB2Jeofy PamaNo ratings yet
- CholedocholithiasisDocument3 pagesCholedocholithiasisPao AcelajadoNo ratings yet
- V. Developmental DataDocument6 pagesV. Developmental DataTrixie Al MarieNo ratings yet
- Pulmonary AngiographyDocument3 pagesPulmonary AngiographyBiway RegalaNo ratings yet
- Spinal Cord InjuryDocument28 pagesSpinal Cord InjuryLouie John AbilaNo ratings yet
- AML Case StudyDocument66 pagesAML Case StudyNoel Christian PeraltaNo ratings yet
- Nursing Case AuditDocument53 pagesNursing Case AuditJhean MeansNo ratings yet
- Peritoneal Carcinomatosis Grand Case StudyDocument69 pagesPeritoneal Carcinomatosis Grand Case StudyBeverly Joy RubiNo ratings yet
- Skin Cancer: I. Overview of The DisorderDocument3 pagesSkin Cancer: I. Overview of The DisorderSung ChiiNo ratings yet
- Case Study Ugib Lower MBDocument65 pagesCase Study Ugib Lower MBQuolette Constante100% (1)
- GastritisDocument23 pagesGastritisLisnawati Nur Farida100% (1)
- Tahbso ArticleDocument4 pagesTahbso ArticleAlianna Kristine OhNo ratings yet
- Lap Chole Case StudyDocument3 pagesLap Chole Case StudyKinshuki Jain100% (1)
- Cu 3 Week 3Document3 pagesCu 3 Week 3Maica LectanaNo ratings yet
- Case Study - Dengue Fever V - S UtiDocument12 pagesCase Study - Dengue Fever V - S UtiHarlene Joyce ReyNo ratings yet
- NCP OsteosarcomaDocument6 pagesNCP OsteosarcomaNiksNo ratings yet
- CholelithiasisDocument6 pagesCholelithiasismarkzamNo ratings yet
- Liver AbscessDocument3 pagesLiver AbscessStephanie Pe100% (1)
- Cholelithiasis 0232Document118 pagesCholelithiasis 0232Kz LonerNo ratings yet
- Liver CancerDocument2 pagesLiver CancerPrincess Barnuevo100% (2)
- Final CholelithiasisDocument36 pagesFinal CholelithiasisRalph Pelegrino100% (2)
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Patient Information From Your Surgeon & Sages Laparoscopic Gallbladder RemovalDocument5 pagesPatient Information From Your Surgeon & Sages Laparoscopic Gallbladder RemovalolarrozaNo ratings yet
- Chole SysDocument8 pagesChole SysKas MulyadiNo ratings yet
- Rubella Quantitative IgG - IMMULITE 2000 SystemsDocument40 pagesRubella Quantitative IgG - IMMULITE 2000 SystemsMaria Ruth Moreno VargasNo ratings yet
- Balio Ox-580 Brochure enDocument4 pagesBalio Ox-580 Brochure enMo AlyNo ratings yet
- Association Food Allergy Dried Fish Complex Regional Pain SyndromeDocument5 pagesAssociation Food Allergy Dried Fish Complex Regional Pain SyndromeSSR-IIJLS JournalNo ratings yet
- BV Exam2Document33 pagesBV Exam2Andrew CoatesNo ratings yet
- Eye Essentials Cataract Assessment Classification and Management PDFDocument245 pagesEye Essentials Cataract Assessment Classification and Management PDFihsansiregarNo ratings yet
- PDF Fish S Clinical Psychopathology Signs and Symptoms in Psychiatry Fourth Edition Patricia Casey Ebook Full ChapterDocument53 pagesPDF Fish S Clinical Psychopathology Signs and Symptoms in Psychiatry Fourth Edition Patricia Casey Ebook Full Chapterkrystal.driscoll313100% (3)
- Participant GandhiMCSecunderabadDocument186 pagesParticipant GandhiMCSecunderabadKriti Kumari100% (1)
- Medical Immunology, 7th Edition PDFDocument479 pagesMedical Immunology, 7th Edition PDFoswaldo bigottNo ratings yet
- General Principles of Clinical ToxicologyDocument34 pagesGeneral Principles of Clinical ToxicologySigita KazūneNo ratings yet
- Post Operative Visit ReportDocument10 pagesPost Operative Visit ReportMARIA CHARMIN M. MEJIANo ratings yet
- RA - Heat StresssDocument5 pagesRA - Heat Stresssradeep0% (1)
- Canine Brucellosis Old Foe and Reemerging ScourgeDocument17 pagesCanine Brucellosis Old Foe and Reemerging ScourgeMargarita CCNo ratings yet
- Antivenom Reactions IntroductionDocument14 pagesAntivenom Reactions IntroductionppgpcsNo ratings yet
- The Routes of Administration For Acute Postoperative Pain MedicationDocument17 pagesThe Routes of Administration For Acute Postoperative Pain Medicationronald97hgNo ratings yet
- GlaucomaDocument18 pagesGlaucomaOncología CdsNo ratings yet
- Developmental Dysplasia of The Hip: Dr. Bassel El-Osta SPR Trauma & OrthopaedicsDocument71 pagesDevelopmental Dysplasia of The Hip: Dr. Bassel El-Osta SPR Trauma & OrthopaedicsvadimmadanNo ratings yet
- Bmet 262 Outline 2022 2023Document12 pagesBmet 262 Outline 2022 2023Emmanuel PrahNo ratings yet
- IPA Lantana Poison FlyerDocument2 pagesIPA Lantana Poison FlyerAlan StephenNo ratings yet
- Dr. Larry Blum Testified August 15, 2012Document65 pagesDr. Larry Blum Testified August 15, 2012dubplateNo ratings yet
- American Academy of Sleep Medicine Position Paper For The Use of A Home Sleep Apnea Test For The Diagnosis of OSA in ChildrenDocument5 pagesAmerican Academy of Sleep Medicine Position Paper For The Use of A Home Sleep Apnea Test For The Diagnosis of OSA in ChildrenBenja GuzmánNo ratings yet
- DR Nilofer Saleem - SR - GynecologistDocument10 pagesDR Nilofer Saleem - SR - GynecologistVTekis ConsultingNo ratings yet
- Tic Disorders: by Rawan ChakasDocument17 pagesTic Disorders: by Rawan ChakasRawan ChakasNo ratings yet
- 01.2 Craniotomy and CraniectomyDocument1 page01.2 Craniotomy and Craniectomyfebi novrizalNo ratings yet
- Wound Bed Preparation Leg UlcerDocument6 pagesWound Bed Preparation Leg UlcerAndrei ZbucheaNo ratings yet
- 5 Paragraph Expository Essay OutlineDocument3 pages5 Paragraph Expository Essay Outlineb71bpjha100% (2)
- Endo-Perio Inter Relationship PerioDocument30 pagesEndo-Perio Inter Relationship PerioFourthMolar.com67% (3)
- MI-I Stethoscope and Oto-Ophtalmoscope PPDocument11 pagesMI-I Stethoscope and Oto-Ophtalmoscope PPMani DhamodharanNo ratings yet
- DR. B R Ambedkar Medical Aid SchemeDocument7 pagesDR. B R Ambedkar Medical Aid Schemevineet shendeNo ratings yet
- Sexually Transmitted InfectionDocument16 pagesSexually Transmitted InfectionSonam ChaudharyNo ratings yet
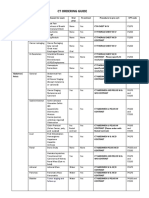
- CT Ordering Guide: Tumor Staging and Follow UpDocument2 pagesCT Ordering Guide: Tumor Staging and Follow UpanonNo ratings yet