Download as pdf or txt
You might also like
- 2 - Maternal Fetal Triage Index - RuhlDocument26 pages2 - Maternal Fetal Triage Index - RuhlGirish SinghNo ratings yet
- Chapter Four - Drug and Substance AbuseDocument49 pagesChapter Four - Drug and Substance AbuseBiruk Shiferaw100% (1)
- Case Study Questionnaire For Malnourished ChildrenDocument5 pagesCase Study Questionnaire For Malnourished ChildrenSta Cruz BacnotanNo ratings yet
- Final Hca 481 Internship Report 1 3Document11 pagesFinal Hca 481 Internship Report 1 3api-535414037No ratings yet
- Substance Abuse: Public Health DefinitionsDocument3 pagesSubstance Abuse: Public Health DefinitionsDebopriyaNo ratings yet
- AddictionDocument32 pagesAddictionISHIKA JAINNo ratings yet
- Understanding Addiction and Its Types CompressedDocument14 pagesUnderstanding Addiction and Its Types Compressedxoreweb780No ratings yet
- Sample Thesis About Drug AddictionDocument6 pagesSample Thesis About Drug Addictiontunwpmzcf100% (2)
- The Caused and Risk of Drugs On AdolescentsDocument20 pagesThe Caused and Risk of Drugs On AdolescentsSyra Mae LausaNo ratings yet
- Drug AddictionDocument29 pagesDrug Addictionavilaaubrey89% (9)
- Drug AbuseDocument5 pagesDrug Abuseduncankogi820No ratings yet
- Drug and Addiction in The WorkplaceDocument10 pagesDrug and Addiction in The WorkplaceMohd HussainNo ratings yet
- NSTP FinalsDocument14 pagesNSTP FinalsCarlton Jove AjosNo ratings yet
- Module 4 Unified Course Pack CWTS 1 2022 2023Document30 pagesModule 4 Unified Course Pack CWTS 1 2022 2023Jan Rey RizonNo ratings yet
- Effects of Drug Abuse and Addiction ON SocietyDocument9 pagesEffects of Drug Abuse and Addiction ON SocietyAditya guptaNo ratings yet
- Report On Drug AddictionDocument30 pagesReport On Drug AddictionChirag GoyalNo ratings yet
- ZezeDocument19 pagesZezeanon_332349544No ratings yet
- Department of Physics,: Submitted byDocument15 pagesDepartment of Physics,: Submitted byAzhar NawazNo ratings yet
- Psyc 311Document10 pagesPsyc 311Bongile MkhonzaNo ratings yet
- Drugs and Substance AbuseDocument10 pagesDrugs and Substance AbuseMark KinotiNo ratings yet
- Drug Addiction-Home AssignmentDocument7 pagesDrug Addiction-Home AssignmentLynxNo ratings yet
- Mid Term-Essay On Drug AddictionDocument12 pagesMid Term-Essay On Drug AddictionShubho Dev nathNo ratings yet
- Addiction Is A DiseaseDocument12 pagesAddiction Is A DiseaseNatalia IlinaNo ratings yet
- Research On Drugs AbuseDocument8 pagesResearch On Drugs AbusefredrickfoleyNo ratings yet
- Learning Kit in Health 9: Quarter 2 (Week 1 - 4)Document11 pagesLearning Kit in Health 9: Quarter 2 (Week 1 - 4)Reabels FranciscoNo ratings yet
- Introduction For Research Paper About DrugsDocument6 pagesIntroduction For Research Paper About Drugsfvf2ffp6100% (1)
- Drug WarDocument8 pagesDrug Warsiejuroa23No ratings yet
- Substance Abuse DefinedDocument4 pagesSubstance Abuse DefinedzzzzikiiiiNo ratings yet
- Substance Abuse DisorderDocument3 pagesSubstance Abuse DisorderZubiaNo ratings yet
- Dual Diagnosis: Mental Illness and Substance AbuseDocument2 pagesDual Diagnosis: Mental Illness and Substance AbuseShanna MitchellNo ratings yet
- Causes and Effect of Drug AddictionDocument3 pagesCauses and Effect of Drug AddictionEdmund HalleyNo ratings yet
- Drugs AbuseDocument20 pagesDrugs AbuseKrishnaNo ratings yet
- Drug Addiction Has Become A Worldwide ProblemDocument8 pagesDrug Addiction Has Become A Worldwide ProblemNor Mi NaNo ratings yet
- Human Behavior and VictimologyDocument7 pagesHuman Behavior and VictimologyE&M ArtsNo ratings yet
- What Is Addiction?Document2 pagesWhat Is Addiction?sopho10No ratings yet
- What Are Illegal Drugs?Document6 pagesWhat Are Illegal Drugs?Rustumme Mirelle ReyesNo ratings yet
- Drug AddictionDocument7 pagesDrug AddictionZechariah NicholasNo ratings yet
- Research Paper 10-BerylDocument11 pagesResearch Paper 10-BerylMaria Del AdelantarNo ratings yet
- Rsemue Video IsiDocument5 pagesRsemue Video IsiPuvaan RaajNo ratings yet
- Facts You Should Know About Drug Abuse and Addiction DisorderDocument2 pagesFacts You Should Know About Drug Abuse and Addiction DisorderElijah Tochukwu DavidNo ratings yet
- Drug Addiction and Traffic Rules 1Document31 pagesDrug Addiction and Traffic Rules 1ISHIKA JAINNo ratings yet
- Lesson 3 - Substance Use, Addictions, Mental Health, Stigma and Discrimination and in The WorkplaceDocument8 pagesLesson 3 - Substance Use, Addictions, Mental Health, Stigma and Discrimination and in The WorkplaceCala WritesNo ratings yet
- 211-11-1251 FinalDocument5 pages211-11-1251 FinalFoysal AhmedNo ratings yet
- Drug AbuseDocument7 pagesDrug Abusemativenganokutenda400No ratings yet
- Cause and Effects of Substance Abuse Among The Students Community480Document15 pagesCause and Effects of Substance Abuse Among The Students Community480Suman MondalNo ratings yet
- Submitted By:Shagun Vishwanath 1020202148 Ballb Semester 1: TopicDocument13 pagesSubmitted By:Shagun Vishwanath 1020202148 Ballb Semester 1: TopicShagun VishwanathNo ratings yet
- Drug Dependence What Is Drug Dependence?Document6 pagesDrug Dependence What Is Drug Dependence?Bibiana ZapataNo ratings yet
- Drugs and Substance AbuseDocument4 pagesDrugs and Substance Abusevaibhavch2904No ratings yet
- Alcohol and Substance AbuseDocument30 pagesAlcohol and Substance AbusejackrosesNo ratings yet
- English Proficiency 3Document16 pagesEnglish Proficiency 3aribniminnakNo ratings yet
- What Is Drug Abuse: Prescription Medicines OpioidsDocument11 pagesWhat Is Drug Abuse: Prescription Medicines OpioidsAnusuya BaruahNo ratings yet
- Drug AddictionDocument8 pagesDrug AddictionNgan TracKimNo ratings yet
- English Language School Base Assessment: Drug Abuse The Impact of Drug Abuse in Family RelationshipDocument10 pagesEnglish Language School Base Assessment: Drug Abuse The Impact of Drug Abuse in Family RelationshipsrtwgwfwwgwNo ratings yet
- Prescription Drug Abuse Research Paper ThesisDocument6 pagesPrescription Drug Abuse Research Paper Thesiselizabethjenkinsatlanta100% (1)
- Causes and Treatment of AddictionDocument21 pagesCauses and Treatment of AddictionNizam100% (1)
- Drug AddictionDocument9 pagesDrug Addictionbirinder31No ratings yet
- Drug Addiction 1Document4 pagesDrug Addiction 1Dharthi KNo ratings yet
- Drug Ed Chapter VDocument15 pagesDrug Ed Chapter VCOLOMA, Jasper R.No ratings yet
- Drug Addiction EditedDocument28 pagesDrug Addiction EditedBea PaneloNo ratings yet
- Global Institutes of Management and Emerging Technology: Project On Drug AddictionDocument17 pagesGlobal Institutes of Management and Emerging Technology: Project On Drug AddictionSumitpal SinghNo ratings yet
- Present Simple Vs Present Continuous - English Grammar in Use - Intermediate - 3e - Supplementary ExercisesDocument5 pagesPresent Simple Vs Present Continuous - English Grammar in Use - Intermediate - 3e - Supplementary ExercisesAgZawNo ratings yet
- Past Tense-AcititiesDocument6 pagesPast Tense-AcititiesAgZawNo ratings yet
- Hsot Law MapDocument2 pagesHsot Law MapAgZawNo ratings yet
- Jade and Conflict Executive Summary EN - June 2021Document10 pagesJade and Conflict Executive Summary EN - June 2021AgZaw100% (1)
- The Kachin Conflict 2014Document54 pagesThe Kachin Conflict 2014AgZawNo ratings yet
- Gothic ArchitectureDocument1 pageGothic ArchitectureAgZawNo ratings yet
- Present-Tenses Oxford English Grammar Course 2-IntermediateDocument3 pagesPresent-Tenses Oxford English Grammar Course 2-IntermediateAgZawNo ratings yet
- Reading Table Completion Complete IELTS Bands 4-5 WB p.6Document1 pageReading Table Completion Complete IELTS Bands 4-5 WB p.6AgZawNo ratings yet
- Program Milestone 2 - ADAPT Rapid Assessment ReportDocument51 pagesProgram Milestone 2 - ADAPT Rapid Assessment ReportAgZawNo ratings yet
- ADAPT Rehabilitation 90 Days Activities - Thandar (N) 26 May 2022Document34 pagesADAPT Rehabilitation 90 Days Activities - Thandar (N) 26 May 2022AgZawNo ratings yet
- ADAPT - Rapid Assessment SummaryDocument4 pagesADAPT - Rapid Assessment SummaryAgZawNo ratings yet
- Reading - True-False - MAKING FRIENDS - Bridge To IELTS - Preinter (35-45) - p5Document2 pagesReading - True-False - MAKING FRIENDS - Bridge To IELTS - Preinter (35-45) - p5AgZawNo ratings yet
- Reading - Yes-No-Not-Given - The Funcation of Language - From Objective IELTS - Intermediate - SB - p12Document2 pagesReading - Yes-No-Not-Given - The Funcation of Language - From Objective IELTS - Intermediate - SB - p12AgZaw100% (1)
- Community Profile Meed Assessment Teachers GuideDocument24 pagesCommunity Profile Meed Assessment Teachers GuideAgZawNo ratings yet
- Reading - True-False-Not Given - THE CASHLESS SOCIETY - Achieve IELTS 2Document2 pagesReading - True-False-Not Given - THE CASHLESS SOCIETY - Achieve IELTS 2AgZawNo ratings yet
- Syllabus - Political Sociology - MAPol Science - 901C English - 21072017Document188 pagesSyllabus - Political Sociology - MAPol Science - 901C English - 21072017AgZawNo ratings yet
- Swallow in Migration - Improve - Your - Skills - Reading - For - IELTS - 4.5-6.0 - SB - p12Document2 pagesSwallow in Migration - Improve - Your - Skills - Reading - For - IELTS - 4.5-6.0 - SB - p12AgZaw50% (2)
- Appendix 1: LTO Weekly Report Format: 1. Voter Information / Education Yes NODocument28 pagesAppendix 1: LTO Weekly Report Format: 1. Voter Information / Education Yes NOAgZawNo ratings yet
- Going To Vs WillDocument2 pagesGoing To Vs WillAgZawNo ratings yet
- NGO Funding and ChinaDocument6 pagesNGO Funding and ChinaAgZawNo ratings yet
- Connected Speech - Assimilation - New Headway Pronunciation Course - Upper-Intermediate - p.52 PDFDocument1 pageConnected Speech - Assimilation - New Headway Pronunciation Course - Upper-Intermediate - p.52 PDFAgZawNo ratings yet
- Img 20200315 0002Document1 pageImg 20200315 0002AgZawNo ratings yet
- Chief Auditor's Report Written According To Laws, Chief Auditor RespondsDocument3 pagesChief Auditor's Report Written According To Laws, Chief Auditor RespondsAgZawNo ratings yet
- Topic, Main Idea, Suporting Details-TestDocument5 pagesTopic, Main Idea, Suporting Details-TestAgZawNo ratings yet
- Yangon Region Hluttaw Draws Up A Draft-Bill To Reduce Waste To Public FundsDocument3 pagesYangon Region Hluttaw Draws Up A Draft-Bill To Reduce Waste To Public FundsAgZawNo ratings yet
- Kachin State Chief Auditor's Report Points Out Certain Departments Not Acting According To Laws (Part - 1)Document6 pagesKachin State Chief Auditor's Report Points Out Certain Departments Not Acting According To Laws (Part - 1)AgZawNo ratings yet
- 5-Aminolevulinic Acid Photodynamic Therapy For Condyloma Acuminatum of Urethral MeatusDocument19 pages5-Aminolevulinic Acid Photodynamic Therapy For Condyloma Acuminatum of Urethral MeatusRiefka Ananda ZulfaNo ratings yet
- CHN Lab - Quiz IMCIDocument3 pagesCHN Lab - Quiz IMCIKristine KimNo ratings yet
- Post Marketing Surveillance Plan NMRA NewDocument9 pagesPost Marketing Surveillance Plan NMRA NewDeshal RanasingheNo ratings yet
- BGH Case SlipsDocument7 pagesBGH Case SlipsLoungayvan BatuyogNo ratings yet
- WhataretheargumentsforandagainstvaccinationsforchildrenDocument11 pagesWhataretheargumentsforandagainstvaccinationsforchildrenapi-220893802100% (1)
- Ebola Virus Disease: SeminarDocument13 pagesEbola Virus Disease: Seminarximena rodriguez cadenaNo ratings yet
- Stages of Labour ChartDocument1 pageStages of Labour ChartAisyahrahma93No ratings yet
- Certificate Nih Stroke ScaleDocument1 pageCertificate Nih Stroke Scaleapi-354841289No ratings yet
- Pathophysiology of Breast CancerDocument3 pagesPathophysiology of Breast Cancerpauline mangadaNo ratings yet
- Myths in Infection ControlDocument30 pagesMyths in Infection ControlDukeNo ratings yet
- Case Study For Hepa ADocument5 pagesCase Study For Hepa AGabbii CincoNo ratings yet
- Lecture - Nutrition and Diet TherapyDocument9 pagesLecture - Nutrition and Diet TherapyLalaine Marie BianzonNo ratings yet
- Policy Relating To Health Safety and Welfare of EmployeesDocument13 pagesPolicy Relating To Health Safety and Welfare of Employeeslucky javellanaNo ratings yet
- Stage 3 Handbook 2012Document21 pagesStage 3 Handbook 2012Nikhil KumarNo ratings yet
- Chapter 02Document44 pagesChapter 02Carlos ChuNo ratings yet
- Outcomes of Percutaneous Endoscopic Gastrostomy in ChildrenDocument7 pagesOutcomes of Percutaneous Endoscopic Gastrostomy in ChildrenHenry BarberenaNo ratings yet
- School Form 2 Daily Attendance Report of Learners For Senior High School (SF2-SHS)Document3 pagesSchool Form 2 Daily Attendance Report of Learners For Senior High School (SF2-SHS)Jemarjo SalandananNo ratings yet
- Critical Evaluation of Nursing ProgrammeDocument31 pagesCritical Evaluation of Nursing ProgrammeManoj Garg86% (14)
- Health ProblemDocument2 pagesHealth ProblemDilausan B MolukNo ratings yet
- GP Maternal NICE Final 1Document1 pageGP Maternal NICE Final 1Guillermo CalderaroNo ratings yet
- E P N M (Mhgap) : Saint Tonis College, IncDocument11 pagesE P N M (Mhgap) : Saint Tonis College, IncDivine MacaibaNo ratings yet
- Autoimmune Hemolytic AnemiaDocument7 pagesAutoimmune Hemolytic AnemiaHoopmen SilaenNo ratings yet
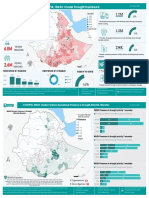
- 2023 WASH Cluster Drought Product JuneDocument2 pages2023 WASH Cluster Drought Product JuneResilient GemeNo ratings yet
- Colon, Rectum and Anus-Dr. SigitDocument121 pagesColon, Rectum and Anus-Dr. SigitYuliana Latif100% (1)
- SAGES Consent 2019 2023Document16 pagesSAGES Consent 2019 2023cNo ratings yet
- Research 3Document12 pagesResearch 3Pratxxm PatelNo ratings yet
- 2020 Status Report As of August 31, 2021Document192 pages2020 Status Report As of August 31, 2021Jasper Kenneth PeraltaNo ratings yet