Download as pdf or txt
You might also like
- Project For PractoDocument86 pagesProject For PractoMurali2k1369% (16)
- Tugas Pengantar Akuntansi-1Document23 pagesTugas Pengantar Akuntansi-1Wiedya fitrianaNo ratings yet
- Talent Handbook AddendumDocument21 pagesTalent Handbook AddendumJay SteeleNo ratings yet
- Nurse Change-Of-Shift Report PolicyDocument2 pagesNurse Change-Of-Shift Report Policyapi-235633705No ratings yet
- Market Profile - Trading Strategies 1 2-2Document26 pagesMarket Profile - Trading Strategies 1 2-2Jay Steele100% (1)
- Scope of Appointment FormDocument2 pagesScope of Appointment Formapi-260208821100% (1)
- Medical BillingDocument16 pagesMedical BillingAbdul Gaffoor100% (6)
- 2013 Scope of Appointment Form - CORBINDocument2 pages2013 Scope of Appointment Form - CORBINCorbin LindseyNo ratings yet
- Anthem Scope of App.Document2 pagesAnthem Scope of App.family-instituteNo ratings yet
- Scope of Appointment Form 2011 UniversalDocument2 pagesScope of Appointment Form 2011 UniversalvmgreekNo ratings yet
- Tref 22Document17 pagesTref 22sike1977No ratings yet
- Medicare Open Enrollment For 2014Document2 pagesMedicare Open Enrollment For 2014Doug PotashNo ratings yet
- Smileeee 86826468Document7 pagesSmileeee 86826468Frvrkpop LifeNo ratings yet
- Anthem Benefits Book 2016 10 4Document110 pagesAnthem Benefits Book 2016 10 4Hue LeNo ratings yet
- Medicare Private Fee For Service PlansDocument28 pagesMedicare Private Fee For Service PlansMabz BuanNo ratings yet
- Manulife Extended Group Health Booklet-April 1, 2022-1Document63 pagesManulife Extended Group Health Booklet-April 1, 2022-1ShanthiNo ratings yet
- Training Manual (New)Document16 pagesTraining Manual (New)fahhad lashari100% (3)
- 2020 Benefits Information Guide: Understanding Your Options Staffing EmployeesDocument28 pages2020 Benefits Information Guide: Understanding Your Options Staffing Employeeseric.risnerNo ratings yet
- Humana Scope of App. - 2Document2 pagesHumana Scope of App. - 2family-instituteNo ratings yet
- 2016 Uhc Hsa SBCDocument88 pages2016 Uhc Hsa SBCRodrigo RomeroNo ratings yet
- A Better Medicare. A Better You: MD Medicarechoice, IncDocument19 pagesA Better Medicare. A Better You: MD Medicarechoice, Inclancastd54No ratings yet
- Ba25180st Rev0912 WBDocument6 pagesBa25180st Rev0912 WBJamesMyersNo ratings yet
- Medicare Part C Medicare AdvantageDocument3 pagesMedicare Part C Medicare AdvantageJonathan CoutiñoNo ratings yet
- Assignment of Benefits MedicareDocument6 pagesAssignment of Benefits Medicarepmojoumpd100% (1)
- Ppo BR MD Pref Sta PR VaDocument16 pagesPpo BR MD Pref Sta PR VaMichael D ReevesNo ratings yet
- Medicare Participating Physician or Supplier AgreementDocument3 pagesMedicare Participating Physician or Supplier AgreementRohit GhuseNo ratings yet
- Eow HC Aca Upheld 062812Document4 pagesEow HC Aca Upheld 062812marshall_johnso6704No ratings yet
- Smileeee 86826468Document5 pagesSmileeee 86826468Frvrkpop LifeNo ratings yet
- HumanaChoice SNP-DE H5216-267 Summary of BenefitsDocument24 pagesHumanaChoice SNP-DE H5216-267 Summary of Benefitsadela EstradaNo ratings yet
- Medicare AssignmentDocument13 pagesMedicare AssignmentmivbciwlfNo ratings yet
- 11036Document28 pages11036api-309082881No ratings yet
- Welcome To Rio Grande Hospital and Clinics!Document2 pagesWelcome To Rio Grande Hospital and Clinics!swarnaNo ratings yet
- SPD Ra Spd2011Document51 pagesSPD Ra Spd2011Judy RomatelliNo ratings yet
- MVP Sample LetterDocument2 pagesMVP Sample LetterKristieNo ratings yet
- What You Should Know About Provider NetworksDocument3 pagesWhat You Should Know About Provider NetworksAnthony El HageNo ratings yet
- Tufts Enrollment FormDocument2 pagesTufts Enrollment FormgeorgeNo ratings yet
- Welcome To Medicare!: Things To Think About When You Compare Medicare Drug CoverageDocument4 pagesWelcome To Medicare!: Things To Think About When You Compare Medicare Drug CoverageAlsayed General HospitalNo ratings yet
- Please Sign DocuSign Tandem Diabetes CareDocument64 pagesPlease Sign DocuSign Tandem Diabetes CareMyah SandovalNo ratings yet
- GCH PDFDocument32 pagesGCH PDFKevin ZhangNo ratings yet
- MD Medicarechoice Florida Optimum MB: Section I - Introduction To The Summary of Benefits ForDocument18 pagesMD Medicarechoice Florida Optimum MB: Section I - Introduction To The Summary of Benefits Forlancastd54No ratings yet
- Different Types of Medicare Insurance PlanDocument7 pagesDifferent Types of Medicare Insurance PlanGetmy PolicyNo ratings yet
- Medicare Supplement Insurance, Aug 2011Document16 pagesMedicare Supplement Insurance, Aug 2011Jon EnglekingNo ratings yet
- Maxicare Application FormDocument6 pagesMaxicare Application Formmeniemartin03No ratings yet
- Patient Information Sheet 091409Document2 pagesPatient Information Sheet 091409api-16816262No ratings yet
- Summary of Benefits: For Bcbsga Mediblue Access (Ppo)Document44 pagesSummary of Benefits: For Bcbsga Mediblue Access (Ppo)J MillerNo ratings yet
- Marketplace Exchange Notice - RetailDocument4 pagesMarketplace Exchange Notice - Retailangeliquei95No ratings yet
- Sisc Q ADocument7 pagesSisc Q Aapi-204910805No ratings yet
- Coordination of Benefits: Where Can I Get More Information?Document2 pagesCoordination of Benefits: Where Can I Get More Information?api-309082881No ratings yet
- Anthem Blue Cross Medical Enrollment Form 2014Document4 pagesAnthem Blue Cross Medical Enrollment Form 2014Tanveer ShaikhNo ratings yet
- Top 8 Medicare MistakesDocument4 pagesTop 8 Medicare MistakesTrisha Laraga100% (1)
- Fan Understanding The Insurance ProcessDocument12 pagesFan Understanding The Insurance ProcessWill SackettNo ratings yet
- How to Enroll in Medicare Health Insurance: Choose a Medicare Part D Drug Plan and a Medicare Supplement PlanFrom EverandHow to Enroll in Medicare Health Insurance: Choose a Medicare Part D Drug Plan and a Medicare Supplement PlanNo ratings yet
- Eligibility NoticeDocument17 pagesEligibility NoticeFlintston3No ratings yet
- School Employees Benefits Board (SEBB) Program Plan Overview and Cost of CoverageDocument4 pagesSchool Employees Benefits Board (SEBB) Program Plan Overview and Cost of CoverageRaisul ShakilNo ratings yet
- Enrollment PeriodsDocument12 pagesEnrollment Periodsapi-239463541No ratings yet
- Summary of Benefits While On Unpaid LeaveDocument5 pagesSummary of Benefits While On Unpaid LeavePatrick CoffeeNo ratings yet
- Healthcare Reform and You: Key ProvisionsDocument5 pagesHealthcare Reform and You: Key Provisionsapi-252555369No ratings yet
- UHC Description of BenefitsDocument9 pagesUHC Description of BenefitsSebastián GuevaraNo ratings yet
- 2020 Employer Toolkit V12 1Document22 pages2020 Employer Toolkit V12 1sachinitsmeNo ratings yet
- Medicare and BTGC 2014Document4 pagesMedicare and BTGC 2014Todd GroveNo ratings yet
- US HealthcareDocument3 pagesUS HealthcareRaghu TejaNo ratings yet
- Remistart Enrollment FormDocument2 pagesRemistart Enrollment FormDerek LemonNo ratings yet
- Aetna Open Access Managed Choice: Answers Important Questions Why This MattersDocument8 pagesAetna Open Access Managed Choice: Answers Important Questions Why This MattersChris BohoNo ratings yet
- Medicare: Socialsecurity - GovDocument24 pagesMedicare: Socialsecurity - Govtreb trebNo ratings yet
- 2023 Bankruptcy Forms For Florida - UpsolveDocument1 page2023 Bankruptcy Forms For Florida - UpsolveJay SteeleNo ratings yet
- Passing Chords - Jazz Guitar Online Premium Courses - WWW - Jazzguitar.beDocument1 pagePassing Chords - Jazz Guitar Online Premium Courses - WWW - Jazzguitar.beJay SteeleNo ratings yet
- Blank Ukulele Chord Paper - Ukulele Club AmsterdamDocument1 pageBlank Ukulele Chord Paper - Ukulele Club AmsterdamJay SteeleNo ratings yet
- AudioThing StringsDocument3 pagesAudioThing StringsJay SteeleNo ratings yet
- Plug-In Reference, CubaseDocument213 pagesPlug-In Reference, CubaseJay SteeleNo ratings yet
- Harmony For Interlude MirageDocument1 pageHarmony For Interlude MirageJay SteeleNo ratings yet
- Kontakt 5 Application Reference EnglishDocument339 pagesKontakt 5 Application Reference EnglishJay SteeleNo ratings yet
- Chord ChartsDocument1 pageChord ChartsJay SteeleNo ratings yet
- Daryl Streumer Solo.2Document2 pagesDaryl Streumer Solo.2Jay SteeleNo ratings yet
- 16 Cubase Secrets You Might Not Know A - HTTP - WWW - Musicradar.com - TuitionDocument1 page16 Cubase Secrets You Might Not Know A - HTTP - WWW - Musicradar.com - TuitionJay SteeleNo ratings yet
- Don T Give UpDocument7 pagesDon T Give UpJay Steele100% (1)
- Kat Pad1Document11 pagesKat Pad1Jay SteeleNo ratings yet
- Domestic Violence PetitionDocument1 pageDomestic Violence PetitionJay SteeleNo ratings yet
- Installing Uvi Soundbanks enDocument15 pagesInstalling Uvi Soundbanks enJay SteeleNo ratings yet
- Florida Courts E-Filing Portal User Manual Sept 2014Document106 pagesFlorida Courts E-Filing Portal User Manual Sept 2014Jay SteeleNo ratings yet
- UVIWorkstation User GuideDocument19 pagesUVIWorkstation User GuideJay SteeleNo ratings yet
- Jazziz - Earl Klugh - PDF - Jazz - American Styles of MusicDocument1 pageJazziz - Earl Klugh - PDF - Jazz - American Styles of MusicJay SteeleNo ratings yet
- 2022 FL FormularyDocument174 pages2022 FL FormularyJay SteeleNo ratings yet
- Waltz For Ruth - P MethenyDocument1 pageWaltz For Ruth - P MethenyJay SteeleNo ratings yet
- Little KidsDocument1 pageLittle KidsJay SteeleNo ratings yet
- Medicareful Enrollment Process - MCDocument2 pagesMedicareful Enrollment Process - MCJay SteeleNo ratings yet
- KYNC VerticalsRevenueDocument28 pagesKYNC VerticalsRevenueJay SteeleNo ratings yet
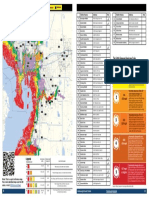
- Hillsborough Evacuation Zone Map EnglishDocument1 pageHillsborough Evacuation Zone Map EnglishJay SteeleNo ratings yet
- Zimmerman Aff. Part 4 Ex. P ZDocument79 pagesZimmerman Aff. Part 4 Ex. P ZJay SteeleNo ratings yet
- EON206P UserGuide 082914 EmailDocument16 pagesEON206P UserGuide 082914 EmailJay SteeleNo ratings yet
- How To pdft-2Document5 pagesHow To pdft-2Jay SteeleNo ratings yet
- Uviworkstation User Guide enDocument20 pagesUviworkstation User Guide enJay SteeleNo ratings yet
- PacesetterAug2022 SpreadsDocument5 pagesPacesetterAug2022 SpreadsJay SteeleNo ratings yet
- LogRhythm Microsoft Office 365 Log CollectionDocument3 pagesLogRhythm Microsoft Office 365 Log CollectionCesar AlmadaNo ratings yet
- Transunion Rwanda Limited Comprehensive Consumer Report With Risk Score Bank of Kigali (Bank Sector Bureau) All Sector ReportDocument9 pagesTransunion Rwanda Limited Comprehensive Consumer Report With Risk Score Bank of Kigali (Bank Sector Bureau) All Sector Reportnalpha66No ratings yet
- 244585723Document43 pages244585723Raymundo EirahNo ratings yet
- Let Us Discover: Tvl-Computer Systems Servicing-Grade 12Document6 pagesLet Us Discover: Tvl-Computer Systems Servicing-Grade 12KibasuperNo ratings yet
- Fixed Wireless Access With 5G at Mid-BandsDocument9 pagesFixed Wireless Access With 5G at Mid-BandsChannuNo ratings yet
- 9788131531907Document5 pages9788131531907B SRIRAMNo ratings yet
- VikramDocument15 pagesVikramPavan ShindeNo ratings yet
- ECS Tuning - Order Receipt #237492127Document1 pageECS Tuning - Order Receipt #237492127LuisNo ratings yet
- Conversation Between Waiter and A Customer ..Document6 pagesConversation Between Waiter and A Customer ..irina KPOPNo ratings yet
- Lamesgin ResearchDocument24 pagesLamesgin ResearchRobbob JahloveNo ratings yet
- How To Manage A Spend2Save Account: Internet Banking Mobile BankingDocument1 pageHow To Manage A Spend2Save Account: Internet Banking Mobile BankingAKANHO TIMOTHYNo ratings yet
- Indemnity Bond Universal Sompo General Insurane Co LTDDocument2 pagesIndemnity Bond Universal Sompo General Insurane Co LTDRajendraNo ratings yet
- Vlan-Rutas EstaticasDocument5 pagesVlan-Rutas EstaticasJuan CarlosNo ratings yet
- Internal Audit For Organizational Resilience: Balancing Assurance - Advisory-AnticipateDocument70 pagesInternal Audit For Organizational Resilience: Balancing Assurance - Advisory-Anticipatemikael abubakarNo ratings yet
- Cpa Review Auditing ProblemsDocument16 pagesCpa Review Auditing ProblemsMellinia MantesNo ratings yet
- Lab 1 TelecommunicationDocument17 pagesLab 1 TelecommunicationDhamirah MirahNo ratings yet
- Visa Global Registry of Service Providers January 26 2024 (USA)Document141 pagesVisa Global Registry of Service Providers January 26 2024 (USA)outmuscleNo ratings yet
- Zigbee Technology: A Seminar Report ONDocument68 pagesZigbee Technology: A Seminar Report ONarchanasingh88100% (3)
- SPD eRAN7.0 CSFB Feature Introduction-20140228-A-1.0Document50 pagesSPD eRAN7.0 CSFB Feature Introduction-20140228-A-1.0contact2vikasNo ratings yet
- TMT 4q 2015 Software Reader PDFDocument28 pagesTMT 4q 2015 Software Reader PDFanwinphilipsNo ratings yet
- Proxying Eduroam With freeRADIUSDocument37 pagesProxying Eduroam With freeRADIUSakun1994No ratings yet
- Workshop About TransportDocument6 pagesWorkshop About TransportYure Acuña GüetteNo ratings yet
- Assessment of Internal Auditing Practice in Dashen Bank Jimma BranchDocument41 pagesAssessment of Internal Auditing Practice in Dashen Bank Jimma Branchwossen gebremariam100% (4)
- Packet Tracer 5.3 - IP Telephony Basic Configuration Tutorial DescriptionDocument4 pagesPacket Tracer 5.3 - IP Telephony Basic Configuration Tutorial DescriptionJoseOctavioGonzalezNo ratings yet
- RimDocument21 pagesRimmartinhochihangNo ratings yet
- Kotak MahindraDocument30 pagesKotak Mahindrakaushal2442No ratings yet