
OB Ch.16,17
OB Ch.16,17
You might also like
- Lesson Plan in Grade 10 ScienceDocument4 pagesLesson Plan in Grade 10 ScienceRonald Jacob Picorro71% (17)
- Hema 1 August 2021Document84 pagesHema 1 August 2021Renz Gerard Amor100% (1)
- OB Test 2 Study GuideDocument21 pagesOB Test 2 Study GuideJaclyn FugateNo ratings yet
- NUR 145 Lecture 2 Term 2Document184 pagesNUR 145 Lecture 2 Term 2Maria Jonalyn Bautista RodelasNo ratings yet
- Open Pediatric ArcherDocument84 pagesOpen Pediatric Archerbaharada1979No ratings yet
- 103 Final MASTER GUIDEDocument131 pages103 Final MASTER GUIDEkpbrown32296No ratings yet
- Ballard, APGAR, EINC, BreastfeedingDocument91 pagesBallard, APGAR, EINC, BreastfeedingFaydhal SalikNo ratings yet
- FundamentalsDocument34 pagesFundamentalsColleen CalditoNo ratings yet
- Neonatal ResuscitationDocument51 pagesNeonatal ResuscitationAbdulkadir HasanNo ratings yet
- Maternity and Women Chapter 23Document11 pagesMaternity and Women Chapter 23Sam JonesNo ratings yet
- Introduction To NewbornDocument57 pagesIntroduction To Newbornnicu.aiims24No ratings yet
- Immediate Physical CareDocument73 pagesImmediate Physical CareronelnNo ratings yet
- Care For High Risk and Sick NewbornDocument78 pagesCare For High Risk and Sick NewbornMatthew CalaraNo ratings yet
- Nursing Care of A Family When A Child Has A Neurologic DisorderDocument8 pagesNursing Care of A Family When A Child Has A Neurologic DisorderBern NerquitNo ratings yet
- Neonatal CareDocument59 pagesNeonatal CareKeith LajotNo ratings yet
- AKuhlmann 4 ADocument2 pagesAKuhlmann 4 Ataylormharvey16No ratings yet
- Pediatrics NotesDocument72 pagesPediatrics NotesSHEENA MAE DE LOS REYES100% (1)
- Chapter 12 Wilkins - NeoPedia AssessmentDocument21 pagesChapter 12 Wilkins - NeoPedia AssessmentQuevee CondezNo ratings yet
- Peds Exam 2Document38 pagesPeds Exam 2Stephanie SuruNo ratings yet
- CARE OF NEWBORN HandoutDocument21 pagesCARE OF NEWBORN HandoutMonica SebastinNo ratings yet
- Unit 2 - Patient Assessment Study GuideDocument9 pagesUnit 2 - Patient Assessment Study Guidebraylyn.arisonNo ratings yet
- Postnatal CareDocument19 pagesPostnatal Carejomarie gamiao0% (1)
- Neonatal Resuscitation: Vineetha.T 1 Year MSC NursingDocument106 pagesNeonatal Resuscitation: Vineetha.T 1 Year MSC NursingVineetha ThachedathNo ratings yet
- Basic Care and ComfortDocument49 pagesBasic Care and Comfortdelrosariodenisejoy05No ratings yet
- Newborn (MSC BUK)Document68 pagesNewborn (MSC BUK)Aysha KurfiNo ratings yet
- Neonatal ResuscitationDocument34 pagesNeonatal ResuscitationAthul IgnatiusNo ratings yet
- New Born ResuscitationDocument34 pagesNew Born ResuscitationPAUL NDEKINo ratings yet
- Neonatal Emergencies FinalDocument90 pagesNeonatal Emergencies FinalDr Raseena VattamkandathilNo ratings yet
- FHR VariabilityDocument19 pagesFHR VariabilityLorraine Tuesday BuenviajeNo ratings yet
- At I Maternal NewbornDocument24 pagesAt I Maternal NewbornEunice Cortés100% (2)
- Nursing Care of A Neonate Part 1Document67 pagesNursing Care of A Neonate Part 1Rani G SNo ratings yet
- In Class Week 1 AbridgedDocument38 pagesIn Class Week 1 AbridgedAlejandro VillasenorNo ratings yet
- BLS 01 HX and PE of The Newborn, Child, and Adolescent 11 - 08 and 12 - 06 (Updated)Document17 pagesBLS 01 HX and PE of The Newborn, Child, and Adolescent 11 - 08 and 12 - 06 (Updated)Nikka ReyesNo ratings yet
- Assessment of The Normal NewbornDocument6 pagesAssessment of The Normal Newborndhalal100% (2)
- Immediate Postpartum Care 1Document31 pagesImmediate Postpartum Care 1CRISTINE DELNo ratings yet
- Neonatology 1Document104 pagesNeonatology 1Oluwanisola OgayemiNo ratings yet
- Qna MW Summary - 2024Document10 pagesQna MW Summary - 2024AZHAR NAWAWINo ratings yet
- Lecture 2 Asphyxia NeonatorumDocument66 pagesLecture 2 Asphyxia Neonatorumpokua34No ratings yet
- EincDocument14 pagesEincmendoza jhamNo ratings yet
- Level 2 Skills Lab PresentationDocument24 pagesLevel 2 Skills Lab PresentationJamie HaravataNo ratings yet
- Newborn AssessmentDocument46 pagesNewborn AssessmentAbigail Mangaoang50% (2)
- Essential Newborn CareDocument14 pagesEssential Newborn CareJam Corros100% (1)
- NCM 109 DR and Nursery 2023 1Document38 pagesNCM 109 DR and Nursery 2023 1Patricia CaladoNo ratings yet
- Newborn CareDocument51 pagesNewborn CareHurley ReefNo ratings yet
- Newborn CareDocument120 pagesNewborn Carejuly3ciaNo ratings yet
- Topic 8 - The NewbornDocument16 pagesTopic 8 - The NewbornReanne Mae AbreraNo ratings yet
- Immediate Care of The NewbornDocument3 pagesImmediate Care of The NewbornBianca CamilleNo ratings yet
- Immediate Care of The NewbornDocument4 pagesImmediate Care of The Newbornmelinda100% (1)
- Postnatal CareDocument28 pagesPostnatal CareChristineNo ratings yet
- NEWBORN ASSESSMENT DajuuuuuuuuuuuuuuuuDocument31 pagesNEWBORN ASSESSMENT Dajuuuuuuuuuuuuuuuuamal abdulrahmanNo ratings yet
- Assesment of The Newborn Baby-KuliahDocument67 pagesAssesment of The Newborn Baby-Kuliahamel015No ratings yet
- Peds Exam 1 ReviewDocument19 pagesPeds Exam 1 ReviewMahreen UmatiyaNo ratings yet
- PostnatalDocument99 pagesPostnatalPlain GerlNo ratings yet
- Pediatric ConceptDocument19 pagesPediatric ConceptAntonio Intia IVNo ratings yet
- Hesi Review For MaternityDocument29 pagesHesi Review For MaternitySteam Lc86% (21)
- Lec 107 - FinalsDocument23 pagesLec 107 - Finalsannie lalangNo ratings yet
- PretermDocument88 pagesPretermAhmed KitawNo ratings yet
- Obstetric ExaminationDocument12 pagesObstetric ExaminationNena MineNo ratings yet
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Imm - Tech.cell Culture - Class.1Document28 pagesImm - Tech.cell Culture - Class.1Uma MaheshNo ratings yet
- Kidney Function Test Essentials HandbookDocument66 pagesKidney Function Test Essentials HandbookVesna Danity100% (1)
- Influence of Coffee On The Health and Lifestyle of Singaporean YouthsDocument8 pagesInfluence of Coffee On The Health and Lifestyle of Singaporean YouthsMun Yen LoiNo ratings yet
- Neuropsychology 2O23Document8 pagesNeuropsychology 2O23farhaanah.abdullah02No ratings yet
- High Percentage of Sleep Disturbances Can Affect The Recovery of The PatientDocument1 pageHigh Percentage of Sleep Disturbances Can Affect The Recovery of The PatientMatt SinnungNo ratings yet
- Testicular Torsion, Hydrocele & Fournier GangreneDocument41 pagesTesticular Torsion, Hydrocele & Fournier GangreneNur Insyirah100% (1)
- Comparison of The Effects of Yoga and LSM-1Document5 pagesComparison of The Effects of Yoga and LSM-1Irfan FauziNo ratings yet
- Tabela-De-Pressão-Arterial Inf Adolesc 2017 PDFDocument4 pagesTabela-De-Pressão-Arterial Inf Adolesc 2017 PDFTaináNo ratings yet
- High-Voltage Pulsed Galvanic Stimulation (HVPGS)Document12 pagesHigh-Voltage Pulsed Galvanic Stimulation (HVPGS)akheel ahammed100% (1)
- The Respiratory System: Anatomy & Physiology ReviewDocument1 pageThe Respiratory System: Anatomy & Physiology ReviewMaxinne Allyssa Cancino RoseñoNo ratings yet
- Intestinal Plasmacytoma in An African HedgehogDocument5 pagesIntestinal Plasmacytoma in An African HedgehogJoão Pedro PiccoloNo ratings yet
- Fill in The Blanks Muscular Fitness Edition: Name: Date: PeriodDocument2 pagesFill in The Blanks Muscular Fitness Edition: Name: Date: PeriodJack MessarosNo ratings yet
- Stoker C23Document15 pagesStoker C23Zahir Jayvee Gayak IINo ratings yet
- MATERNALDocument32 pagesMATERNALsean blaze100% (1)
- Racial Characteristics of Human Teeth With Special Emphasis On The Mongoloid DentitionDocument7 pagesRacial Characteristics of Human Teeth With Special Emphasis On The Mongoloid DentitionRidwan FajiriNo ratings yet
- Excerpt From "Presence" by Amy CuddyDocument10 pagesExcerpt From "Presence" by Amy CuddyOnPointRadioNo ratings yet
- Cell Division PDFDocument5 pagesCell Division PDFCabdicasiis Maxamuud GuuleedNo ratings yet
- Digestive System: Digestion and Absorption of Carbohydrates, Proteins and FatsDocument45 pagesDigestive System: Digestion and Absorption of Carbohydrates, Proteins and FatshiNo ratings yet
- Science Exam Part I. Write The Parts of The Excretory System. (4 Points)Document5 pagesScience Exam Part I. Write The Parts of The Excretory System. (4 Points)Siria PinedaNo ratings yet
- Drug AbuseDocument47 pagesDrug Abusekrishna100% (3)
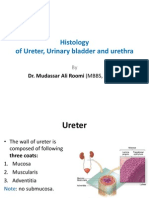
- Histology of Ureter, Urinary Bladder and Urethra by Dr. RoomiDocument20 pagesHistology of Ureter, Urinary Bladder and Urethra by Dr. RoomiMudassar Roomi100% (4)
- Motion Analysis Study of A Scapular Orientation ExerciseDocument6 pagesMotion Analysis Study of A Scapular Orientation ExerciseCmmb FisioterapiaNo ratings yet
- None 19cb74f7Document6 pagesNone 19cb74f7Odii MaraNo ratings yet
- Buku Saku UrologiDocument33 pagesBuku Saku UrologisitisarahNo ratings yet
- Zoology - WikipediaDocument33 pagesZoology - WikipediaAcuh Chii ArcaNo ratings yet
- Drug Induced Dyselectrolytemia - A Case ReportDocument4 pagesDrug Induced Dyselectrolytemia - A Case ReportBaru Chandrasekhar RaoNo ratings yet
- NCP ProperDocument9 pagesNCP Properstephanie eduarteNo ratings yet
- Q3 Science 10 Module 3Document26 pagesQ3 Science 10 Module 3Rizalyn Patalinghug100% (1)
























































































Download as docx, pdf, or txt
You might also like
- Lesson Plan in Grade 10 ScienceDocument4 pagesLesson Plan in Grade 10 ScienceRonald Jacob Picorro71% (17)
- Hema 1 August 2021Document84 pagesHema 1 August 2021Renz Gerard Amor100% (1)
- OB Test 2 Study GuideDocument21 pagesOB Test 2 Study GuideJaclyn FugateNo ratings yet
- NUR 145 Lecture 2 Term 2Document184 pagesNUR 145 Lecture 2 Term 2Maria Jonalyn Bautista RodelasNo ratings yet
- Open Pediatric ArcherDocument84 pagesOpen Pediatric Archerbaharada1979No ratings yet
- 103 Final MASTER GUIDEDocument131 pages103 Final MASTER GUIDEkpbrown32296No ratings yet
- Ballard, APGAR, EINC, BreastfeedingDocument91 pagesBallard, APGAR, EINC, BreastfeedingFaydhal SalikNo ratings yet
- FundamentalsDocument34 pagesFundamentalsColleen CalditoNo ratings yet
- Neonatal ResuscitationDocument51 pagesNeonatal ResuscitationAbdulkadir HasanNo ratings yet
- Maternity and Women Chapter 23Document11 pagesMaternity and Women Chapter 23Sam JonesNo ratings yet
- Introduction To NewbornDocument57 pagesIntroduction To Newbornnicu.aiims24No ratings yet
- Immediate Physical CareDocument73 pagesImmediate Physical CareronelnNo ratings yet
- Care For High Risk and Sick NewbornDocument78 pagesCare For High Risk and Sick NewbornMatthew CalaraNo ratings yet
- Nursing Care of A Family When A Child Has A Neurologic DisorderDocument8 pagesNursing Care of A Family When A Child Has A Neurologic DisorderBern NerquitNo ratings yet
- Neonatal CareDocument59 pagesNeonatal CareKeith LajotNo ratings yet
- AKuhlmann 4 ADocument2 pagesAKuhlmann 4 Ataylormharvey16No ratings yet
- Pediatrics NotesDocument72 pagesPediatrics NotesSHEENA MAE DE LOS REYES100% (1)
- Chapter 12 Wilkins - NeoPedia AssessmentDocument21 pagesChapter 12 Wilkins - NeoPedia AssessmentQuevee CondezNo ratings yet
- Peds Exam 2Document38 pagesPeds Exam 2Stephanie SuruNo ratings yet
- CARE OF NEWBORN HandoutDocument21 pagesCARE OF NEWBORN HandoutMonica SebastinNo ratings yet
- Unit 2 - Patient Assessment Study GuideDocument9 pagesUnit 2 - Patient Assessment Study Guidebraylyn.arisonNo ratings yet
- Postnatal CareDocument19 pagesPostnatal Carejomarie gamiao0% (1)
- Neonatal Resuscitation: Vineetha.T 1 Year MSC NursingDocument106 pagesNeonatal Resuscitation: Vineetha.T 1 Year MSC NursingVineetha ThachedathNo ratings yet
- Basic Care and ComfortDocument49 pagesBasic Care and Comfortdelrosariodenisejoy05No ratings yet
- Newborn (MSC BUK)Document68 pagesNewborn (MSC BUK)Aysha KurfiNo ratings yet
- Neonatal ResuscitationDocument34 pagesNeonatal ResuscitationAthul IgnatiusNo ratings yet
- New Born ResuscitationDocument34 pagesNew Born ResuscitationPAUL NDEKINo ratings yet
- Neonatal Emergencies FinalDocument90 pagesNeonatal Emergencies FinalDr Raseena VattamkandathilNo ratings yet
- FHR VariabilityDocument19 pagesFHR VariabilityLorraine Tuesday BuenviajeNo ratings yet
- At I Maternal NewbornDocument24 pagesAt I Maternal NewbornEunice Cortés100% (2)
- Nursing Care of A Neonate Part 1Document67 pagesNursing Care of A Neonate Part 1Rani G SNo ratings yet
- In Class Week 1 AbridgedDocument38 pagesIn Class Week 1 AbridgedAlejandro VillasenorNo ratings yet
- BLS 01 HX and PE of The Newborn, Child, and Adolescent 11 - 08 and 12 - 06 (Updated)Document17 pagesBLS 01 HX and PE of The Newborn, Child, and Adolescent 11 - 08 and 12 - 06 (Updated)Nikka ReyesNo ratings yet
- Assessment of The Normal NewbornDocument6 pagesAssessment of The Normal Newborndhalal100% (2)
- Immediate Postpartum Care 1Document31 pagesImmediate Postpartum Care 1CRISTINE DELNo ratings yet
- Neonatology 1Document104 pagesNeonatology 1Oluwanisola OgayemiNo ratings yet
- Qna MW Summary - 2024Document10 pagesQna MW Summary - 2024AZHAR NAWAWINo ratings yet
- Lecture 2 Asphyxia NeonatorumDocument66 pagesLecture 2 Asphyxia Neonatorumpokua34No ratings yet
- EincDocument14 pagesEincmendoza jhamNo ratings yet
- Level 2 Skills Lab PresentationDocument24 pagesLevel 2 Skills Lab PresentationJamie HaravataNo ratings yet
- Newborn AssessmentDocument46 pagesNewborn AssessmentAbigail Mangaoang50% (2)
- Essential Newborn CareDocument14 pagesEssential Newborn CareJam Corros100% (1)
- NCM 109 DR and Nursery 2023 1Document38 pagesNCM 109 DR and Nursery 2023 1Patricia CaladoNo ratings yet
- Newborn CareDocument51 pagesNewborn CareHurley ReefNo ratings yet
- Newborn CareDocument120 pagesNewborn Carejuly3ciaNo ratings yet
- Topic 8 - The NewbornDocument16 pagesTopic 8 - The NewbornReanne Mae AbreraNo ratings yet
- Immediate Care of The NewbornDocument3 pagesImmediate Care of The NewbornBianca CamilleNo ratings yet
- Immediate Care of The NewbornDocument4 pagesImmediate Care of The Newbornmelinda100% (1)
- Postnatal CareDocument28 pagesPostnatal CareChristineNo ratings yet
- NEWBORN ASSESSMENT DajuuuuuuuuuuuuuuuuDocument31 pagesNEWBORN ASSESSMENT Dajuuuuuuuuuuuuuuuuamal abdulrahmanNo ratings yet
- Assesment of The Newborn Baby-KuliahDocument67 pagesAssesment of The Newborn Baby-Kuliahamel015No ratings yet
- Peds Exam 1 ReviewDocument19 pagesPeds Exam 1 ReviewMahreen UmatiyaNo ratings yet
- PostnatalDocument99 pagesPostnatalPlain GerlNo ratings yet
- Pediatric ConceptDocument19 pagesPediatric ConceptAntonio Intia IVNo ratings yet
- Hesi Review For MaternityDocument29 pagesHesi Review For MaternitySteam Lc86% (21)
- Lec 107 - FinalsDocument23 pagesLec 107 - Finalsannie lalangNo ratings yet
- PretermDocument88 pagesPretermAhmed KitawNo ratings yet
- Obstetric ExaminationDocument12 pagesObstetric ExaminationNena MineNo ratings yet
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Imm - Tech.cell Culture - Class.1Document28 pagesImm - Tech.cell Culture - Class.1Uma MaheshNo ratings yet
- Kidney Function Test Essentials HandbookDocument66 pagesKidney Function Test Essentials HandbookVesna Danity100% (1)
- Influence of Coffee On The Health and Lifestyle of Singaporean YouthsDocument8 pagesInfluence of Coffee On The Health and Lifestyle of Singaporean YouthsMun Yen LoiNo ratings yet
- Neuropsychology 2O23Document8 pagesNeuropsychology 2O23farhaanah.abdullah02No ratings yet
- High Percentage of Sleep Disturbances Can Affect The Recovery of The PatientDocument1 pageHigh Percentage of Sleep Disturbances Can Affect The Recovery of The PatientMatt SinnungNo ratings yet
- Testicular Torsion, Hydrocele & Fournier GangreneDocument41 pagesTesticular Torsion, Hydrocele & Fournier GangreneNur Insyirah100% (1)
- Comparison of The Effects of Yoga and LSM-1Document5 pagesComparison of The Effects of Yoga and LSM-1Irfan FauziNo ratings yet
- Tabela-De-Pressão-Arterial Inf Adolesc 2017 PDFDocument4 pagesTabela-De-Pressão-Arterial Inf Adolesc 2017 PDFTaináNo ratings yet
- High-Voltage Pulsed Galvanic Stimulation (HVPGS)Document12 pagesHigh-Voltage Pulsed Galvanic Stimulation (HVPGS)akheel ahammed100% (1)
- The Respiratory System: Anatomy & Physiology ReviewDocument1 pageThe Respiratory System: Anatomy & Physiology ReviewMaxinne Allyssa Cancino RoseñoNo ratings yet
- Intestinal Plasmacytoma in An African HedgehogDocument5 pagesIntestinal Plasmacytoma in An African HedgehogJoão Pedro PiccoloNo ratings yet
- Fill in The Blanks Muscular Fitness Edition: Name: Date: PeriodDocument2 pagesFill in The Blanks Muscular Fitness Edition: Name: Date: PeriodJack MessarosNo ratings yet
- Stoker C23Document15 pagesStoker C23Zahir Jayvee Gayak IINo ratings yet
- MATERNALDocument32 pagesMATERNALsean blaze100% (1)
- Racial Characteristics of Human Teeth With Special Emphasis On The Mongoloid DentitionDocument7 pagesRacial Characteristics of Human Teeth With Special Emphasis On The Mongoloid DentitionRidwan FajiriNo ratings yet
- Excerpt From "Presence" by Amy CuddyDocument10 pagesExcerpt From "Presence" by Amy CuddyOnPointRadioNo ratings yet
- Cell Division PDFDocument5 pagesCell Division PDFCabdicasiis Maxamuud GuuleedNo ratings yet
- Digestive System: Digestion and Absorption of Carbohydrates, Proteins and FatsDocument45 pagesDigestive System: Digestion and Absorption of Carbohydrates, Proteins and FatshiNo ratings yet
- Science Exam Part I. Write The Parts of The Excretory System. (4 Points)Document5 pagesScience Exam Part I. Write The Parts of The Excretory System. (4 Points)Siria PinedaNo ratings yet
- Drug AbuseDocument47 pagesDrug Abusekrishna100% (3)
- Histology of Ureter, Urinary Bladder and Urethra by Dr. RoomiDocument20 pagesHistology of Ureter, Urinary Bladder and Urethra by Dr. RoomiMudassar Roomi100% (4)
- Motion Analysis Study of A Scapular Orientation ExerciseDocument6 pagesMotion Analysis Study of A Scapular Orientation ExerciseCmmb FisioterapiaNo ratings yet
- None 19cb74f7Document6 pagesNone 19cb74f7Odii MaraNo ratings yet
- Buku Saku UrologiDocument33 pagesBuku Saku UrologisitisarahNo ratings yet
- Zoology - WikipediaDocument33 pagesZoology - WikipediaAcuh Chii ArcaNo ratings yet
- Drug Induced Dyselectrolytemia - A Case ReportDocument4 pagesDrug Induced Dyselectrolytemia - A Case ReportBaru Chandrasekhar RaoNo ratings yet
- NCP ProperDocument9 pagesNCP Properstephanie eduarteNo ratings yet
- Q3 Science 10 Module 3Document26 pagesQ3 Science 10 Module 3Rizalyn Patalinghug100% (1)