Download as pdf or txt
You might also like
- Iso 15213-1-2023Document28 pagesIso 15213-1-2023JOSEPH100% (7)
- CASE STUDY Intestinal ObstructionDocument68 pagesCASE STUDY Intestinal ObstructionMaria Paula Bungay91% (23)
- ATI Med Surg SPRING 2019 Post ReviewDocument11 pagesATI Med Surg SPRING 2019 Post ReviewQuincey Hamilton43% (7)
- Training Doc Mercedes 900Document195 pagesTraining Doc Mercedes 900mliugong98% (41)
- Studi Kasus SCMDocument8 pagesStudi Kasus SCMMuflihul Khair0% (5)
- Urinary Incontinence: Pathophysiology and Management OutlineDocument6 pagesUrinary Incontinence: Pathophysiology and Management OutlineNgurah AndhikaNo ratings yet
- Cmaj 157 8 1071Document7 pagesCmaj 157 8 1071hyunra kimNo ratings yet
- 0616 SCuDocument18 pages0616 SCuYolanda Dwi OktaviyaniNo ratings yet
- V21I3S1 06F DrRosenbergDocument10 pagesV21I3S1 06F DrRosenbergAfif AuliyaNo ratings yet
- Incontinencia de OrinaDocument5 pagesIncontinencia de OrinaJennifer EdwardsNo ratings yet
- Perspectives 3Document8 pagesPerspectives 3Golden DreamesNo ratings yet
- Advances in Urethral Stricture Management (Version 1 Referees: 4 Approved)Document9 pagesAdvances in Urethral Stricture Management (Version 1 Referees: 4 Approved)Omomomo781No ratings yet
- Session #42 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Document4 pagesSession #42 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Nicole Ken AgdanaNo ratings yet
- NCMB 314 - M2-Cu10Document10 pagesNCMB 314 - M2-Cu10Giselle EstoquiaNo ratings yet
- Edii StudimDocument31 pagesEdii StudimLindrit AliuNo ratings yet
- Urinary Tract Infection: Notre Dame of Marbel UniversityDocument4 pagesUrinary Tract Infection: Notre Dame of Marbel Universityspain michaelisNo ratings yet
- Management of Patients With Fecal IncontinenceDocument2 pagesManagement of Patients With Fecal IncontinenceJane Arian BerzabalNo ratings yet
- Diagnosis and Treatment of Chronic ConstipationDocument15 pagesDiagnosis and Treatment of Chronic Constipationcc vereNo ratings yet
- Enema. Jal. Pancha Bhuta-323Document6 pagesEnema. Jal. Pancha Bhuta-323Shree GaneshNo ratings yet
- Safety Pilot Study On DoctorsDocument4 pagesSafety Pilot Study On DoctorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Urinary IncontinenceDocument3 pagesUrinary IncontinenceB_i_a_n_c_a_25No ratings yet
- Nephrolithiasis Case StudyDocument31 pagesNephrolithiasis Case StudyL.a.Zumárraga67% (3)
- Urinary Incontinence in Women: John Goforth, Michelle LangakerDocument3 pagesUrinary Incontinence in Women: John Goforth, Michelle LangakerByan AnggaraNo ratings yet
- Renal Replacement Therapy-2Document13 pagesRenal Replacement Therapy-2Magic_OverNo ratings yet
- Thesis Statement For Urinary Tract InfectionDocument7 pagesThesis Statement For Urinary Tract Infectionaflnbwmjhdinys100% (2)
- Nocturia and Nocturnal PoliuriaDocument7 pagesNocturia and Nocturnal PoliuriaKrisna Adhitya WilantaraNo ratings yet
- Veterinary Internal Medicne - 2016 - Lulich - ACVIM Small Animal Consensus Recommendations On The Treatment and PreventionDocument11 pagesVeterinary Internal Medicne - 2016 - Lulich - ACVIM Small Animal Consensus Recommendations On The Treatment and PreventionkradoNo ratings yet
- Urinary Incontinence in Neurological Disease: Assessment and ManagementDocument14 pagesUrinary Incontinence in Neurological Disease: Assessment and ManagementTatiana TanyaNo ratings yet
- Urinary Incontinence in Individuals With Diabetes MellitusDocument1 pageUrinary Incontinence in Individuals With Diabetes MellitusBulan GhafirahNo ratings yet
- Medina Et Al-2016-Neurourology and UrodynamicsDocument11 pagesMedina Et Al-2016-Neurourology and UrodynamicsMarianaNo ratings yet
- Lecture 10.2. Over Active Bladder Blok-CompressedDocument34 pagesLecture 10.2. Over Active Bladder Blok-CompressedkrisnadewirahadiNo ratings yet
- Urinary Incontinence - DiagnosisDocument2 pagesUrinary Incontinence - DiagnosisHoney Roselle MorenoNo ratings yet
- Prostate CancerDocument6 pagesProstate CancerfheisanzNo ratings yet
- Urinary Incontinence: 2 PathophysiologyDocument8 pagesUrinary Incontinence: 2 PathophysiologyZiedTrikiNo ratings yet
- Urinary IncontinenceDocument0 pagesUrinary Incontinencemango91286No ratings yet
- كوزرملا حاضو .د .م.أ لباب ةعماج/ بطلا ةيلك 2019 Urinary Incontinence. Involuntary loss of urine in sufficient amount or frequency to constituteDocument8 pagesكوزرملا حاضو .د .م.أ لباب ةعماج/ بطلا ةيلك 2019 Urinary Incontinence. Involuntary loss of urine in sufficient amount or frequency to constitutewzeer mohammedNo ratings yet
- ACVIM Consensus Statement: J.P. Lulich, A.C. Berent, L.G. Adams, J.L. Westropp, J.W. Bartges, and C.A. OsborneDocument11 pagesACVIM Consensus Statement: J.P. Lulich, A.C. Berent, L.G. Adams, J.L. Westropp, J.W. Bartges, and C.A. OsborneAlana SoaresNo ratings yet
- 44 Danfulani EtalDocument3 pages44 Danfulani EtaleditorijmrhsNo ratings yet
- Fecal IncontinenceDocument5 pagesFecal IncontinenceDaniel Galindo SotomayorNo ratings yet
- Urinary GuidelinesDocument9 pagesUrinary GuidelinesCabinet VeterinarNo ratings yet
- Management of IncontinenceDocument91 pagesManagement of IncontinenceVahid Msmi100% (1)
- Practice: A Review The Relevance of Gastrointestinal Fistulae in ClinicalDocument10 pagesPractice: A Review The Relevance of Gastrointestinal Fistulae in ClinicalCecilia VillaverdeNo ratings yet
- Urinary Tract TumorsDocument13 pagesUrinary Tract Tumors4D RAGUINI, Meeka EllaNo ratings yet
- Thesis UrologyDocument5 pagesThesis Urologydeepjonesmanchester100% (2)
- Emergencia UrologicaDocument13 pagesEmergencia UrologicaEduardo DV MunizNo ratings yet
- ACVIM Consensus Statement: J.P. Lulich, A.C. Berent, L.G. Adams, J.L. Westropp, J.W. Bartges, and C.A. OsborneDocument11 pagesACVIM Consensus Statement: J.P. Lulich, A.C. Berent, L.G. Adams, J.L. Westropp, J.W. Bartges, and C.A. OsborneSofía DruckerNo ratings yet
- 1 s2.0 S183695532100014X MainDocument8 pages1 s2.0 S183695532100014X MainMetin HakkanNo ratings yet
- Page 4062693Document53 pagesPage 4062693alexandermarcusNo ratings yet
- UTIsDocument25 pagesUTIsAnamul MasumNo ratings yet
- Antireflux Surgery 2015 PDFDocument247 pagesAntireflux Surgery 2015 PDFDiego Andres VasquezNo ratings yet
- FGRGDocument14 pagesFGRGRicky Adi witokoNo ratings yet
- Urinary Incontinence in Norwegian Nursing Home ResidentsDocument7 pagesUrinary Incontinence in Norwegian Nursing Home ResidentsKrisnawatiNo ratings yet
- Chiropractic - Management - of - Pubic - Symphysis - Shear - in Overactive BladderDocument10 pagesChiropractic - Management - of - Pubic - Symphysis - Shear - in Overactive BladderDenise MathreNo ratings yet
- A Healthy Bladder: A Consensus StatementDocument11 pagesA Healthy Bladder: A Consensus StatementAndrew WongkarNo ratings yet
- Managing Urinary Incontinence in Older PeopleDocument5 pagesManaging Urinary Incontinence in Older PeopleSarah Naura IrbahNo ratings yet
- Kidney StoneDocument28 pagesKidney StoneAlreem AlhajryNo ratings yet
- Bladder News 10 HydroDocument3 pagesBladder News 10 HydrosaidyanzNo ratings yet
- Augmentation Bladder KomplikasiDocument9 pagesAugmentation Bladder KomplikasiOlivia BawaedaNo ratings yet
- Urinary Incontinence 335236 153 38333 v3Document6 pagesUrinary Incontinence 335236 153 38333 v3jermumNo ratings yet
- Rapunzel Sindrom EngDocument6 pagesRapunzel Sindrom Engzhrqryr8npNo ratings yet
- Female Urinary Tract Infections in Clinical PracticeFrom EverandFemale Urinary Tract Infections in Clinical PracticeBob YangNo ratings yet
- Rules and Directions for the Employment of Injections in Various DiseasesFrom EverandRules and Directions for the Employment of Injections in Various DiseasesNo ratings yet
- 19 - Bearing Capacity - Eccentric LoadingDocument5 pages19 - Bearing Capacity - Eccentric LoadinghiyeonNo ratings yet
- The Talmud of Jerusalem - Schwab Moise 1839-1918 TRDocument201 pagesThe Talmud of Jerusalem - Schwab Moise 1839-1918 TRJanice O'BrianNo ratings yet
- Outsmart Your Anxious Brain - Worksheet Diagnosis Guide ExercisesDocument6 pagesOutsmart Your Anxious Brain - Worksheet Diagnosis Guide Exercisesdoppler_100% (1)
- SOLOXLEXDocument4 pagesSOLOXLEXAlex KamaraNo ratings yet
- Experiment 4 Turbine CharacteristicsDocument12 pagesExperiment 4 Turbine CharacteristicsChong Ru YinNo ratings yet
- PTCL Stormfiber Packages - Google SearchDocument1 pagePTCL Stormfiber Packages - Google Searchmachinekicking63No ratings yet
- Maersk IntrepidDocument8 pagesMaersk Intrepidrickyngs100% (1)
- 635 BrainwritingDocument8 pages635 BrainwritingTran TrungNo ratings yet
- QnA Intro To Gas Regulation in Indonesia (Ilham Maulana)Document15 pagesQnA Intro To Gas Regulation in Indonesia (Ilham Maulana)Ilham Maulana Ash Shiddieq100% (1)
- Parts Catalog ARDFDocument30 pagesParts Catalog ARDFUlmanu ValentinNo ratings yet
- English FinalDocument71 pagesEnglish FinalKhadeeja MarjanNo ratings yet
- KKSB1273 Teknologi Binaan Dan Bahan 01 1112 - 09 Konkrit Sebagai Bahan BinaanDocument56 pagesKKSB1273 Teknologi Binaan Dan Bahan 01 1112 - 09 Konkrit Sebagai Bahan BinaanFarhana NorzelanNo ratings yet
- STRUCTURE Magazine - Condition Assessment of Old Stone Retaining Walls PDFDocument8 pagesSTRUCTURE Magazine - Condition Assessment of Old Stone Retaining Walls PDFShabbir LokhandwalaNo ratings yet
- Adriafil SummerDocument5 pagesAdriafil SummerTatu AradiNo ratings yet
- Experienced Based Rules of Chemical EngineeringDocument13 pagesExperienced Based Rules of Chemical Engineeringvazzoleralex6884No ratings yet
- Pathway - Skoliosis GROUPDocument12 pagesPathway - Skoliosis GROUPAnonymous NZTQVgjaNo ratings yet
- Unit Two. Dominant Theories Approaches: Positivism Rational Choice Theory MarxismDocument8 pagesUnit Two. Dominant Theories Approaches: Positivism Rational Choice Theory MarxismPaul RicoNo ratings yet
- Up ListDocument200 pagesUp Listprashant guptaNo ratings yet
- 2012 Training Materials PDFDocument32 pages2012 Training Materials PDFWisam Ankah100% (1)
- P2 Chp2 Section 2.1ADocument3 pagesP2 Chp2 Section 2.1APaing Khant KyawNo ratings yet
- GSB PDFDocument4 pagesGSB PDFsachin sNo ratings yet
- Project Documentation SandeepDocument19 pagesProject Documentation SandeepFYIT80Sultan ShaikhNo ratings yet
- Ap One Pagers Combined PDFDocument10 pagesAp One Pagers Combined PDFJack KirbyNo ratings yet
- ARTS7 Q3 Week6Document7 pagesARTS7 Q3 Week6Samantha Nicole CarlotoNo ratings yet
- Nclex Boot CampDocument24 pagesNclex Boot CampMariekris Sangalang100% (12)
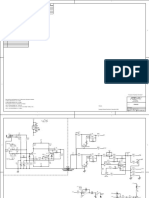
- Peavey Xr8000 SCHDocument12 pagesPeavey Xr8000 SCHLisandro Orrego SalvadorNo ratings yet
- Scienco AP-30: Air Piston PumpDocument2 pagesScienco AP-30: Air Piston PumpSergio SalgadoNo ratings yet