Download as docx, pdf, or txt
You might also like
- SJT Practice Paper 2 Large PrintDocument82 pagesSJT Practice Paper 2 Large PrintezzezzatNo ratings yet
- Theories Applied To MidwiferyDocument25 pagesTheories Applied To Midwiferybhawna83% (24)
- NURSING CARE PLAN - Breast CancerDocument2 pagesNURSING CARE PLAN - Breast Cancerderic100% (3)
- A Problem of Display Codes Case StudyDocument7 pagesA Problem of Display Codes Case StudyJam EsNo ratings yet
- NCP Modified Radical MastectomyDocument5 pagesNCP Modified Radical MastectomyIvan Jules P. PALMARESNo ratings yet
- Case Study 6Document4 pagesCase Study 6Mary Hope Bacuta0% (2)
- 2 - EndometriosisDocument3 pages2 - EndometriosisJayson Olile100% (1)
- AssessmentDocument3 pagesAssessmentJemma GandaNo ratings yet
- Independent: IndependentDocument6 pagesIndependent: IndependentGina PrancelisoNo ratings yet
- Assessment Nursing Diagnosis Nursing Inference Nursing Goal Nursing Interventions EvaluationDocument4 pagesAssessment Nursing Diagnosis Nursing Inference Nursing Goal Nursing Interventions EvaluationtrishxianieNo ratings yet
- Teaching Plan For A Client Undergoing A Surgery: (Preoperative Phase)Document7 pagesTeaching Plan For A Client Undergoing A Surgery: (Preoperative Phase)Ezequiel RosalesNo ratings yet
- Subjective: Goal: Dependent: Dependent:: Assessment Diagnosis Plan Intervention Rationale EvaluationDocument2 pagesSubjective: Goal: Dependent: Dependent:: Assessment Diagnosis Plan Intervention Rationale EvaluationTrisha Cayabyab100% (1)
- Subjective Data Patient Said ," Malai Mero Swastha Awasthalai Liyera Pir Pari Rakheko Chha. Objective Data Anxious Facial Expression RestlessnessDocument9 pagesSubjective Data Patient Said ," Malai Mero Swastha Awasthalai Liyera Pir Pari Rakheko Chha. Objective Data Anxious Facial Expression RestlessnessVisha MainaliNo ratings yet
- Independent: IndependentDocument4 pagesIndependent: IndependentGina PrancelisoNo ratings yet
- AP NCP by Garcia, p.-1Document4 pagesAP NCP by Garcia, p.-1Princess GarciaNo ratings yet
- NCP For Bladder CaDocument4 pagesNCP For Bladder CaChris Tine CaccamNo ratings yet
- 3 Nursing Care PlanDocument6 pages3 Nursing Care PlanJeyser T. GamutiaNo ratings yet
- CARE PLAN Format - Deficient Knowledge PGDocument2 pagesCARE PLAN Format - Deficient Knowledge PGjinsi georgeNo ratings yet
- Tuano, Salma M. Bsn4-1 Fear/AnxietyDocument3 pagesTuano, Salma M. Bsn4-1 Fear/AnxietySALMA M. TUANO100% (1)
- Nueva Ecija University of Science and Technology: O V A ADocument16 pagesNueva Ecija University of Science and Technology: O V A AKym RonquilloNo ratings yet
- Assessment Nursing Diagnosis Outcome Identification Planning Nursing Intervention Evaluation IndependentDocument7 pagesAssessment Nursing Diagnosis Outcome Identification Planning Nursing Intervention Evaluation IndependentQueenie Silva100% (1)
- Formulation of Nursing Care Plan: Date/Ti Me Cues Need Nursing DiagnosisDocument4 pagesFormulation of Nursing Care Plan: Date/Ti Me Cues Need Nursing DiagnosisCooky JeonNo ratings yet
- Acute PainDocument4 pagesAcute PainRuffy AbdulazisNo ratings yet
- Nursing Care Plan For Breast Cancer NCPDocument2 pagesNursing Care Plan For Breast Cancer NCPEsha MeharNo ratings yet
- Discharge Planning: By: Chin V. UlamDocument2 pagesDischarge Planning: By: Chin V. UlamChin Villanueva UlamNo ratings yet
- Nursing Care Plan For Breast Cancer NCP PDFDocument2 pagesNursing Care Plan For Breast Cancer NCP PDFMaina Barman100% (1)
- Nursing Care Plan For Breast Cancer NCPDocument2 pagesNursing Care Plan For Breast Cancer NCPMaina BarmanNo ratings yet
- Nursing Care Plan For Breast Cancer NCP PDFDocument2 pagesNursing Care Plan For Breast Cancer NCP PDFMaina BarmanNo ratings yet
- Anxiety in WIlm's TumorDocument3 pagesAnxiety in WIlm's TumorDwinxelle Eiven CristobalNo ratings yet
- Ncp-Post OpDocument3 pagesNcp-Post OpFran LanNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Short Term GoalDocument2 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Short Term GoalKhatlen BagaresNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Goal MetDocument2 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Goal MetDickson,Emilia JadeNo ratings yet
- NCP For Hyperemesis GravidarumDocument5 pagesNCP For Hyperemesis Gravidarumclaire parkNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationDarlene LaudeNo ratings yet
- NCP Deficient KnowlwdgeDocument2 pagesNCP Deficient KnowlwdgeMICHELLE MALLARENo ratings yet
- NCP Self DeficitDocument2 pagesNCP Self DeficitSalume DayananNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanTrisha CayabyabNo ratings yet
- Marjorie ncp8Document2 pagesMarjorie ncp8Jovel CortezNo ratings yet
- Nursing DX Ineffective CopingDocument2 pagesNursing DX Ineffective CopingBillNo ratings yet
- Di Ko To Sure Kung Tama Yung Rel To Disease ProcessDocument8 pagesDi Ko To Sure Kung Tama Yung Rel To Disease ProcessNyeam NyeamNo ratings yet
- Nursing Care Plan: Efficiency: Were TheDocument2 pagesNursing Care Plan: Efficiency: Were TheDonato J JacintoNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanSophia Loraine Dorone Jesura100% (1)
- Case 1Document7 pagesCase 1Jullienne Ysabelle AngNo ratings yet
- TM 4-Patient Centered Communication .PPSXDocument51 pagesTM 4-Patient Centered Communication .PPSXribka sparkleNo ratings yet
- NURSING CARE PLAN (For Case Study)Document2 pagesNURSING CARE PLAN (For Case Study)Kathleen Martinez100% (1)
- NCP Ortho TanakaDocument4 pagesNCP Ortho TanakaJopaii TanakaNo ratings yet
- Sample NCPDocument5 pagesSample NCPRuffy AbdulazisNo ratings yet
- Local Theories and Their WorksDocument21 pagesLocal Theories and Their WorksSheen CatayongNo ratings yet
- Nursing Care Plan: Angeles University Foundation College of NursingDocument2 pagesNursing Care Plan: Angeles University Foundation College of NursingRey Ann PangilinanNo ratings yet
- Qst. Paul University Philippines: School of Nursing and Allied Health Sciences College of NursingDocument5 pagesQst. Paul University Philippines: School of Nursing and Allied Health Sciences College of NursingChristian UmosoNo ratings yet
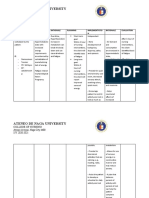
- Ateneo de Naga University: College of NursingDocument4 pagesAteneo de Naga University: College of NursingRenie SerranoNo ratings yet
- NCP FractureDocument7 pagesNCP FractureMacris BondocNo ratings yet
- ClinicalDocument5 pagesClinicalMary Hope BacutaNo ratings yet
- Ncma217 Rle - Case StudyDocument15 pagesNcma217 Rle - Case Studyanjie kamidNo ratings yet
- NCP For PCAPDocument4 pagesNCP For PCAPDianeNo ratings yet
- NCPDocument6 pagesNCPNik Rose ElNo ratings yet
- Acute PainDocument4 pagesAcute PainIvan Jules P. PALMARESNo ratings yet
- DRUGSTUDYDocument3 pagesDRUGSTUDYmyqs4d7rmxNo ratings yet
- Dr. D's Pain Treatment Manual: Practical Pain Management Solutions (REVISED NEW EDITION 2024)From EverandDr. D's Pain Treatment Manual: Practical Pain Management Solutions (REVISED NEW EDITION 2024)Rating: 5 out of 5 stars5/5 (1)
- Suggestion Therapeutic (Translated): Diseases treated by means suggestive and hypnoticFrom EverandSuggestion Therapeutic (Translated): Diseases treated by means suggestive and hypnoticNo ratings yet
- Medical Integration Model as it Pertains to Musculoskeletal ConditionsFrom EverandMedical Integration Model as it Pertains to Musculoskeletal ConditionsNo ratings yet
- Craniosacral Therapy: A Beginner's Guide and Overview on Its Use Cases, with an FAQFrom EverandCraniosacral Therapy: A Beginner's Guide and Overview on Its Use Cases, with an FAQNo ratings yet
- The Optic Neuritis Mastery Bible: Your Blueprint for Complete Optic Neuritis ManagementFrom EverandThe Optic Neuritis Mastery Bible: Your Blueprint for Complete Optic Neuritis ManagementNo ratings yet
- World Patient Safety DayDocument17 pagesWorld Patient Safety DayNam PHẠM THÀNHNo ratings yet
- Health CenterDocument12 pagesHealth Centerjobel alejandrinoNo ratings yet
- Sample Test 1 - QuestionnaireDocument5 pagesSample Test 1 - QuestionnaireAira CatubayNo ratings yet
- Creating Customer Value, Satisfaction and LoyaltyDocument22 pagesCreating Customer Value, Satisfaction and LoyaltyVictor BureaNo ratings yet
- Action ResearchDocument12 pagesAction ResearchLee CelNo ratings yet
- Nama: Yoga Eka Prasetyo NIM: 16105 Mata Kuliah: Bahasa Inggris 2 Tugas: Make A SentenceDocument10 pagesNama: Yoga Eka Prasetyo NIM: 16105 Mata Kuliah: Bahasa Inggris 2 Tugas: Make A SentenceYoga EkaNo ratings yet
- Explanation About Medical Writing - JemsDocument2 pagesExplanation About Medical Writing - JemsJemma Rose TegioNo ratings yet
- Emma Cohen Resume MsotDocument2 pagesEmma Cohen Resume Msotapi-362293951No ratings yet
- EY Ripe For Investment The Indonesian Health Care Industry Post Introduction of Universal Health CoverageDocument76 pagesEY Ripe For Investment The Indonesian Health Care Industry Post Introduction of Universal Health CoverageIka Wulan PermataNo ratings yet
- Why Become A DoctorDocument12 pagesWhy Become A DoctorKIDD1987No ratings yet
- NURS FPX 6612 Assessment 1 Triple Aim Outcome MeasuresDocument6 pagesNURS FPX 6612 Assessment 1 Triple Aim Outcome Measuresfarwaamjad771No ratings yet
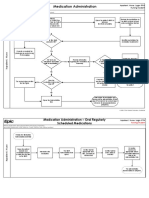
- Medication Administration-Held MedicationsDocument5 pagesMedication Administration-Held MedicationsRawad JamaleddineNo ratings yet
- 5 Benefits of Patient Recall For Chiropractic PracticesDocument13 pages5 Benefits of Patient Recall For Chiropractic PracticeszHealthEHRNo ratings yet
- Weebly Resume-Cover LetterDocument3 pagesWeebly Resume-Cover Letterapi-297917925No ratings yet
- Narrative Report Qip March 2023Document4 pagesNarrative Report Qip March 2023api-237856094No ratings yet
- Tools For Quality MeasurementDocument11 pagesTools For Quality MeasurementFranhel alexandra GarciaNo ratings yet
- Pradnya E Combine For PDFDocument44 pagesPradnya E Combine For PDFAlba Peace100% (1)
- Klickitat Co (WA) Protocols (2010)Document218 pagesKlickitat Co (WA) Protocols (2010)Anthony James-HartwellNo ratings yet
- 02 Family Oriented Medical RecordDocument4 pages02 Family Oriented Medical RecordFernandez-De Ala NicaNo ratings yet
- Nutrition Diagnosis From and (ADA)Document177 pagesNutrition Diagnosis From and (ADA)Cyntia ReyesNo ratings yet
- Wockhardt Hospital HELP DESKDocument2 pagesWockhardt Hospital HELP DESKRajesh MosesNo ratings yet
- Hospital: Ms .Neethu Vincent Asst Professor KVM College of NursingDocument29 pagesHospital: Ms .Neethu Vincent Asst Professor KVM College of NursingNeethu VincentNo ratings yet
- Aggrement PathologyDocument2 pagesAggrement PathologyVIKAS PANERI100% (1)
- Towards Cultural CompetenceDocument12 pagesTowards Cultural CompetenceEmily MuirNo ratings yet
- Quality of Care Before, During, and After Casting: A Cross-Sectional StudyDocument7 pagesQuality of Care Before, During, and After Casting: A Cross-Sectional StudyChristian SierNo ratings yet
- Bupa GuidelineDocument31 pagesBupa GuidelineSara MahsoubNo ratings yet
- Dissertation Topics in Psychiatric NursingDocument8 pagesDissertation Topics in Psychiatric NursingBuyPapersOnlineCheapCanada100% (1)