Download as docx, pdf, or txt
You might also like
- BAMF LinkedIn Influencer ProgramDocument45 pagesBAMF LinkedIn Influencer ProgramAlina Zhoga100% (1)
- MMOGDocument30 pagesMMOGLorenzo Rodriguez100% (1)
- Emergency in OrthopaedicDocument41 pagesEmergency in Orthopaedicmade dollyNo ratings yet
- Pelayanan Digestif November 2021Document12 pagesPelayanan Digestif November 2021ari irawanNo ratings yet
- RCS Edinburgh Basic Surgical Skills Direct Observation of Procedural SkillDocument1 pageRCS Edinburgh Basic Surgical Skills Direct Observation of Procedural SkilljoslinmtggmailcomNo ratings yet
- Extravasation Guidance PDFDocument24 pagesExtravasation Guidance PDFAdiAri RosiuNo ratings yet
- Patofisiologi Nyeri Pada Kelainan BiliodigestifDocument25 pagesPatofisiologi Nyeri Pada Kelainan Biliodigestifbocah_britpopNo ratings yet
- Week 1 Handout 3 Contempt of CourtDocument5 pagesWeek 1 Handout 3 Contempt of CourtMatNo ratings yet
- Eugene Onegin Book PDFDocument2 pagesEugene Onegin Book PDFAmber0% (3)
- Pharm Shelf Big Boss Review Aka Pharmacology Shelf Study GuideDocument13 pagesPharm Shelf Big Boss Review Aka Pharmacology Shelf Study Guideemceelee100% (2)
- Business English SyllabusDocument2 pagesBusiness English SyllabusAde anugrahNo ratings yet
- Abdominal Distention inDocument45 pagesAbdominal Distention inArif Rahman DmNo ratings yet
- FOM STUDY GUIDE 3rd Block 1Document3 pagesFOM STUDY GUIDE 3rd Block 1Bernadine Cruz Par100% (1)
- Kuliah ATLSDocument63 pagesKuliah ATLSDwianggriany Adhetia Piesca Widoretno100% (1)
- CASP Checklist: Case Control Study How To Use This Appraisal ToolDocument6 pagesCASP Checklist: Case Control Study How To Use This Appraisal Toolanon_770867052No ratings yet
- Jurnal Tyroid PDFDocument3 pagesJurnal Tyroid PDFVinnaNo ratings yet
- Non Muscle Invasive Bladder Cancer - EAU Full Guidelines 2019Document50 pagesNon Muscle Invasive Bladder Cancer - EAU Full Guidelines 2019peroksidaseNo ratings yet
- CCDuodenum Periampullary Neoplasms ChuDocument68 pagesCCDuodenum Periampullary Neoplasms ChuSahirNo ratings yet
- Fraktur Humerus Sepertiga DistalDocument26 pagesFraktur Humerus Sepertiga DistalNurul Rezki Fitriani AzisNo ratings yet
- RozerplastyDocument4 pagesRozerplastyLutfi Aulia RahmanNo ratings yet
- Kompartemen SindromDocument9 pagesKompartemen SindromPutri PratiwiNo ratings yet
- LONG CASE Luka BakarDocument16 pagesLONG CASE Luka BakarAfiazka LuthfitaNo ratings yet
- Breast Cancer: Katherine Macgillivray & Melissa PoirierDocument62 pagesBreast Cancer: Katherine Macgillivray & Melissa PoirierJonathan Darell WijayaNo ratings yet
- Perioperative Management 1203114432600412 4Document53 pagesPerioperative Management 1203114432600412 4polushkyNo ratings yet
- OsteosarkomaDocument2 pagesOsteosarkomaLinawati DLNo ratings yet
- Infeksi NosokomialDocument29 pagesInfeksi NosokomialAlunaficha Melody KiraniaNo ratings yet
- Wound de His Cence FinalDocument26 pagesWound de His Cence Finaldanil armandNo ratings yet
- Anal Stenosis and Mucosal EctropionDocument7 pagesAnal Stenosis and Mucosal EctropionpologroNo ratings yet
- Xanthogranulomatous PyelonephritisDocument14 pagesXanthogranulomatous PyelonephritisalaaNo ratings yet
- Oeis SyndromeDocument9 pagesOeis SyndromeADEENo ratings yet
- Jurnal CA TyroidDocument4 pagesJurnal CA TyroidErvina ZelfiNo ratings yet
- Chest TubeDocument8 pagesChest TubeTaufik Nur YahyaNo ratings yet
- Buttonhole DislocationDocument13 pagesButtonhole DislocationHanif Andhika WardhanaNo ratings yet
- Tokyo Guidelines 2018 Flowchart For The Management of Acute CholecystitisDocument43 pagesTokyo Guidelines 2018 Flowchart For The Management of Acute Cholecystitisfranciscomejia14835No ratings yet
- Principles of Minimal Invasive SurgeryDocument39 pagesPrinciples of Minimal Invasive SurgeryAvinash KannanNo ratings yet
- Cystostomy NewDocument32 pagesCystostomy Newkuncupcupu1368No ratings yet
- SEJARAH DAN PERKEMBANGAN ILMU BEDAH September 2017Document18 pagesSEJARAH DAN PERKEMBANGAN ILMU BEDAH September 2017Dipo Mas Suyudi100% (2)
- PDF Lecture 9 Benign Soft Tissue TumorsDocument131 pagesPDF Lecture 9 Benign Soft Tissue TumorsMuhammad Rizqi100% (1)
- Tracheostomy: Indications and ProcedureDocument10 pagesTracheostomy: Indications and ProcedureAinur AbdrakhmanovaNo ratings yet
- WIFI Score For Diabetes Foot UlcerDocument17 pagesWIFI Score For Diabetes Foot Ulcertonylee24100% (1)
- Ivc InjuryDocument17 pagesIvc InjuryAnishChowdhuryNo ratings yet
- Current Concepts in The Management of Dupuytren.3Document8 pagesCurrent Concepts in The Management of Dupuytren.3Shu Yang HuNo ratings yet
- Atelektasis: Penyaji: Martvera SDocument20 pagesAtelektasis: Penyaji: Martvera Saidil ilham100% (1)
- 2013 - Pancreaticoduodenectomy (Whipple Procedure) TechniquesDocument11 pages2013 - Pancreaticoduodenectomy (Whipple Procedure) TechniquesOlteanu IonutNo ratings yet
- 11 Suturing21012015Document30 pages11 Suturing21012015Putri Sari SeptirianiNo ratings yet
- Craniotomy FlapsDocument41 pagesCraniotomy FlapsKaramsi Gopinath NaikNo ratings yet
- Stoma Care Specialist NursingDocument335 pagesStoma Care Specialist Nursingdale rojasNo ratings yet
- To HerniotomiDocument16 pagesTo HerniotomikawaishoneNo ratings yet
- Acute Scrotum 231016 PDFDocument50 pagesAcute Scrotum 231016 PDFDany Dias100% (1)
- Jurnal BTKV Herman 1Document11 pagesJurnal BTKV Herman 1Elyas MuhammadNo ratings yet
- CSP Groin LumpDocument39 pagesCSP Groin LumpFebby ShabrinaNo ratings yet
- Nervus Laryngeus RecurrensDocument5 pagesNervus Laryngeus RecurrensAri Julian SaputraNo ratings yet
- Burst Abdomen: by DR - SuhaibDocument15 pagesBurst Abdomen: by DR - Suhaibsuhaibrehaman100% (1)
- Crush Injuries: Prepared By: Lynette J. CaldoDocument17 pagesCrush Injuries: Prepared By: Lynette J. CaldoLynette JavaNo ratings yet
- Volkmann's Ischemic ContractureDocument41 pagesVolkmann's Ischemic ContractureAayush AryalNo ratings yet
- PCL's Avulsion FractureDocument22 pagesPCL's Avulsion FractureNey da OnneyNo ratings yet
- CombinedDocument3 pagesCombinedSolape Akin-WilliamsNo ratings yet
- Pterigium: Dr. Purnamanita Syawal, SPM, MarsDocument39 pagesPterigium: Dr. Purnamanita Syawal, SPM, Marsyayat muhammadNo ratings yet
- HEMOROIDDocument29 pagesHEMOROIDDanang Aryo PinujiNo ratings yet
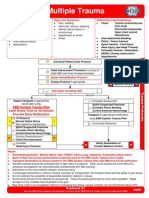
- Multiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationDocument1 pageMultiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationKelly JacksonNo ratings yet
- Hukum CourvoisierDocument1 pageHukum CourvoisierFahryHamkaNo ratings yet
- Penetrating Chest InjuryDocument33 pagesPenetrating Chest InjuryJARRIE BADJIENo ratings yet
- Abdominal Trauma: Supervised By: Dr. Hussein Al-HeisDocument63 pagesAbdominal Trauma: Supervised By: Dr. Hussein Al-HeisRashed ShatnawiNo ratings yet
- EmpyemaDocument17 pagesEmpyemadeo_gratias14No ratings yet
- Stenosing Tenosynovitis, (Trigger Finger) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandStenosing Tenosynovitis, (Trigger Finger) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Clinical Science Session CT Scan Anatomi Kepala Normal: Preceptor: Dyana Eka Hadiati, DR., SP - RadDocument25 pagesClinical Science Session CT Scan Anatomi Kepala Normal: Preceptor: Dyana Eka Hadiati, DR., SP - Radfatimah putriNo ratings yet
- Patgen - Patfis Case 7Document1 pagePatgen - Patfis Case 7fatimah putriNo ratings yet
- Compartment SyndromeDocument14 pagesCompartment Syndromefatimah putriNo ratings yet
- Di Indo Cuma DuaDocument2 pagesDi Indo Cuma Duafatimah putriNo ratings yet
- Dermatovenereological ExamDocument3 pagesDermatovenereological ExamArya MaheswaraNo ratings yet
- Toorthj 8 185Document10 pagesToorthj 8 185fatimah putriNo ratings yet
- CSS Perawatan LukaDocument19 pagesCSS Perawatan Lukafatimah putriNo ratings yet
- Guide BLS + SkenarioDocument4 pagesGuide BLS + Skenariofatimah putriNo ratings yet
- Anatomi Lumbal: Basic ScienceDocument17 pagesAnatomi Lumbal: Basic Sciencefatimah putriNo ratings yet
- CSS Osteoarthritis GenuDocument33 pagesCSS Osteoarthritis Genufatimah putriNo ratings yet
- What Is AsbestosDocument73 pagesWhat Is Asbestosfatimah putriNo ratings yet
- Sbi PDFDocument2 pagesSbi PDFpavans25No ratings yet
- 2018:19 Crime StatsDocument220 pages2018:19 Crime StatsBusinessTech64% (14)
- The Girl With Green Eyes-John EscottDocument9 pagesThe Girl With Green Eyes-John EscottTanuiNo ratings yet
- Lingo 18 Users Manual (001-500)Document500 pagesLingo 18 Users Manual (001-500)Horacio Jesus Prado GarciaNo ratings yet
- Corona Virus (Covid19) : The Grim RealityDocument6 pagesCorona Virus (Covid19) : The Grim RealityGenevieve GayosoNo ratings yet
- Special Relativity Simultaneity, Time Dilation and Length ContractionDocument21 pagesSpecial Relativity Simultaneity, Time Dilation and Length ContractionMuhammad Noman HameedNo ratings yet
- Defense Mechanisms of Plants To Insect Pests: From Morphological To Biochemical ApproachDocument10 pagesDefense Mechanisms of Plants To Insect Pests: From Morphological To Biochemical ApproachDayanaNo ratings yet
- Worksheet 6-Chapter 6 - Bhakti and Suffi TraditionsDocument8 pagesWorksheet 6-Chapter 6 - Bhakti and Suffi TraditionsAvni JainNo ratings yet
- Elementary Logic Gates PDFDocument14 pagesElementary Logic Gates PDFGokaran ShuklaNo ratings yet
- Monday To Friday Except Wednesday For INNA (No Class) : Before SchoolDocument3 pagesMonday To Friday Except Wednesday For INNA (No Class) : Before SchoolJhullian Frederick Val VergaraNo ratings yet
- Gaining Power and InfluenceDocument17 pagesGaining Power and InfluenceMd SelimNo ratings yet
- How To Write Your ReusmeDocument7 pagesHow To Write Your ReusmeBrian Israel Avila FloresNo ratings yet
- Research Project Report STUDENTSDocument15 pagesResearch Project Report STUDENTSAnkit BhatiNo ratings yet
- Tantrik Sadhana For WealthDocument13 pagesTantrik Sadhana For Wealthmanchiraju raj kumarNo ratings yet
- Module in ArtDocument14 pagesModule in ArtMarie Antonette Dacanay LaraNo ratings yet
- Admin Law Case Digest 2Document43 pagesAdmin Law Case Digest 2jstin_jstin100% (1)
- Sewa 2022Document4 pagesSewa 2022eyrxtnnudwjtghbomgNo ratings yet
- BeckettDocument16 pagesBeckettVincenzo Di GioiaNo ratings yet
- Erdogan V Economics: A Scheme To Save The Lira Piles On The Risks InsteadDocument1 pageErdogan V Economics: A Scheme To Save The Lira Piles On The Risks InsteadRuslan AbduraxmanovNo ratings yet
- TafubobunopozomigomasoDocument2 pagesTafubobunopozomigomasoPriyanshusamratNo ratings yet
- Reading Hormonal Changes During PregnancyDocument6 pagesReading Hormonal Changes During PregnancyKlinik Asy syifaNo ratings yet
- Baytan vs. COMELEC, G.R. No. 153945, 396 SCRA 703, 716Document8 pagesBaytan vs. COMELEC, G.R. No. 153945, 396 SCRA 703, 716JM EnguitoNo ratings yet
- Chapter 1 From A Cultural Study of Mary and The AnnunciationDocument15 pagesChapter 1 From A Cultural Study of Mary and The AnnunciationPickering and Chatto100% (1)
- Biochem - Hormone and Signal TransductionDocument36 pagesBiochem - Hormone and Signal TransductionPrincess Jeyan PagatpatanNo ratings yet