Download as pdf or txt
You might also like
- Face Mask WaiverDocument2 pagesFace Mask WaiverLive 5 News0% (1)
- 14 Days Quarantine Plan in Canada: Personal DetailsDocument3 pages14 Days Quarantine Plan in Canada: Personal DetailsIshan WadiNo ratings yet
- Corona Virus Panic The Infectious MythDocument25 pagesCorona Virus Panic The Infectious MythLouisa Livingstone100% (1)
- J Jacbts 2021 10 011Document15 pagesJ Jacbts 2021 10 011Martha CeciliaNo ratings yet
- 2021 Page Covid-19 Thrombose Mecanismes TRDocument8 pages2021 Page Covid-19 Thrombose Mecanismes TRأمين الله القاضيNo ratings yet
- Myocarditis and Pericarditis Following The SARS-CoV-2 Infection and COVID-19 VaccinationDocument18 pagesMyocarditis and Pericarditis Following The SARS-CoV-2 Infection and COVID-19 VaccinationStephen DonovanNo ratings yet
- Covid19 y CardioDocument4 pagesCovid19 y CardioNestor Alonso Lopez RubioNo ratings yet
- Imaging in COVID 19 Related Myocardial InjuryDocument12 pagesImaging in COVID 19 Related Myocardial Injuryorkut verificationNo ratings yet
- Long COVID: Post-Acute Sequelae of COVID-19 With A Cardiovascular FocusDocument22 pagesLong COVID: Post-Acute Sequelae of COVID-19 With A Cardiovascular FocusPhitsanu SuntornpiyapanNo ratings yet
- Long COVID: Post-Acute Sequelae of COVID-19 With A Cardiovascular FocusDocument22 pagesLong COVID: Post-Acute Sequelae of COVID-19 With A Cardiovascular FocusWalter ReyesNo ratings yet
- COVID ProlongadoDocument22 pagesCOVID ProlongadoSMIBA MedicinaNo ratings yet
- (2021 - Atherosclerosis Reports) COVID and Cardiovascular Disease, What We Know in 2021Document12 pages(2021 - Atherosclerosis Reports) COVID and Cardiovascular Disease, What We Know in 2021Iván PérezNo ratings yet
- BackgroundDocument4 pagesBackgroundessay24.filesNo ratings yet
- Covid 19 and CardioDocument15 pagesCovid 19 and CardioMuhammad AfifNo ratings yet
- Molecular Basis of Cardiac and Vascular Injuries Associated With COVID-19Document15 pagesMolecular Basis of Cardiac and Vascular Injuries Associated With COVID-19Aji Prasetyo UtomoNo ratings yet
- Stroke As A Potential Complication of COVID-19-Associated Coagulopathy: A Narrative and Systematic Review of The LiteratureDocument11 pagesStroke As A Potential Complication of COVID-19-Associated Coagulopathy: A Narrative and Systematic Review of The LiteraturedenisNo ratings yet
- COVID-19 in Elderly Adults - Clinical Features, Molecular Mechanisms, and Proposed StrategiesDocument15 pagesCOVID-19 in Elderly Adults - Clinical Features, Molecular Mechanisms, and Proposed StrategiesDanisa EpaNo ratings yet
- Cardiovascular Diseases in Covid 19 A Narrative ReviewDocument6 pagesCardiovascular Diseases in Covid 19 A Narrative ReviewAtul DwivediNo ratings yet
- The Association of Cardiovascular Diseases and Diabetes Mellitus With COVID-19 (SARS-CoV-2) and Their Possible MechanismsDocument6 pagesThe Association of Cardiovascular Diseases and Diabetes Mellitus With COVID-19 (SARS-CoV-2) and Their Possible MechanismsPatty MArivel ReinosoNo ratings yet
- Miocarditis y Covid-19Document8 pagesMiocarditis y Covid-19Jesús Evangelista GomerNo ratings yet
- Clinical Microbiology and InfectionDocument12 pagesClinical Microbiology and Infectionre septian IlhamsyahNo ratings yet
- Dementia and Long CovidDocument16 pagesDementia and Long CovidMaria SilvaNo ratings yet
- Predictors of Mortality of Covid-19 Infected Patients With Acute Kidney InjuryDocument7 pagesPredictors of Mortality of Covid-19 Infected Patients With Acute Kidney InjuryKevin TandartoNo ratings yet
- Biomarcadores Covid19Document12 pagesBiomarcadores Covid19Alan MurilloNo ratings yet
- A Brand-New Cardiorenal Syndrome in The COVID-19 SettingDocument6 pagesA Brand-New Cardiorenal Syndrome in The COVID-19 SettingfannyNo ratings yet
- Medicina 56 00678 With CoverDocument11 pagesMedicina 56 00678 With CovermapsmaxNo ratings yet
- Endothelial Dysfunction in COVID-19 Potential Mechanisms and Possible Therapeutic OptionsDocument24 pagesEndothelial Dysfunction in COVID-19 Potential Mechanisms and Possible Therapeutic OptionssamuelNo ratings yet
- Comment: Lancet Infect Dis 2020Document2 pagesComment: Lancet Infect Dis 2020kayegi8666No ratings yet
- Myocarditis CovidDocument7 pagesMyocarditis CovidbagholderNo ratings yet
- The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 PneumoniaDocument5 pagesThe Clinical and Chest CT Features Associated With Severe and Critical COVID-19 PneumoniaNadanNadhifahNo ratings yet
- Severe Covid-19 Pneumonia - Pathogenesis and Clinical ManagementDocument19 pagesSevere Covid-19 Pneumonia - Pathogenesis and Clinical ManagementRodrigoNo ratings yet
- Severe Covid 19 Pneumonia Pathogenesis and ManagementDocument19 pagesSevere Covid 19 Pneumonia Pathogenesis and ManagementRey CaesarNo ratings yet
- Mediastinal Lymphadenopathy May Predict 30 Day Mortality in PatientsDocument7 pagesMediastinal Lymphadenopathy May Predict 30 Day Mortality in PatientsCess Abad AgcongNo ratings yet
- A Review of Ischemic Stroke in COVID 1910072 - 2021 - Article - 5679Document13 pagesA Review of Ischemic Stroke in COVID 1910072 - 2021 - Article - 5679nascool2016No ratings yet
- Profiling of Lung SARS-CoV-2 and Influenza Virus Infection Dissects Virus-Specific Host Responses and Gene SignaturesDocument19 pagesProfiling of Lung SARS-CoV-2 and Influenza Virus Infection Dissects Virus-Specific Host Responses and Gene Signaturesbrhpcn2rrfNo ratings yet
- Патентний оглядDocument16 pagesПатентний оглядsmarovozyaroslav29No ratings yet
- Article HematologicDisordersAssociatedDocument12 pagesArticle HematologicDisordersAssociatedGleidy M VelásquezNo ratings yet
- NeumoníaDocument19 pagesNeumoníadery sernaNo ratings yet
- Unilateral Common Carotid Artery Dissection in A PDocument3 pagesUnilateral Common Carotid Artery Dissection in A PidhebeatrickNo ratings yet
- Blood 2020006000 PDFDocument21 pagesBlood 2020006000 PDFothilia.obadaNo ratings yet
- Metabolic Characteristics in Patients With COVID 1Document9 pagesMetabolic Characteristics in Patients With COVID 1Nguyễn Tấn PhúNo ratings yet
- Literature Review of Cardiovascular Pathology in Coronavirus InfectionDocument5 pagesLiterature Review of Cardiovascular Pathology in Coronavirus InfectionCentral Asian StudiesNo ratings yet
- COVID 19AndHematology IndiaDocument6 pagesCOVID 19AndHematology IndiaVandana SharmaNo ratings yet
- Assessment of Changes and Complications Caused by Coronavirus Infection in The Lungs Using Computed TomographyDocument6 pagesAssessment of Changes and Complications Caused by Coronavirus Infection in The Lungs Using Computed TomographyCentral Asian StudiesNo ratings yet
- Dandel2021 Heart - Lung Interactions in COVID-19Document15 pagesDandel2021 Heart - Lung Interactions in COVID-19Mario TGNo ratings yet
- Extrapulmonary CT Findings Predict in Hospital Mortality in - 2022 - Academic RDocument14 pagesExtrapulmonary CT Findings Predict in Hospital Mortality in - 2022 - Academic RRicardo MirandaNo ratings yet
- Estado Del Arte CoronavirusDocument17 pagesEstado Del Arte CoronavirusJosé AñorgaNo ratings yet
- The COVID TerjemahanDocument3 pagesThe COVID TerjemahanSusilawaty LestariNo ratings yet
- Automatic COVID 19 Severity Assessment From HRVDocument10 pagesAutomatic COVID 19 Severity Assessment From HRVCarlos Eduardo NorteNo ratings yet
- Cognitive Impact of COVID-19 Alzheimer ResearchDocument16 pagesCognitive Impact of COVID-19 Alzheimer ResearchDionisio Garcia AlvarezNo ratings yet
- Jim 2020 0023 1Document5 pagesJim 2020 0023 1diaconuNo ratings yet
- Multisystem Imaging Manifesta-Tions of COVID-19, Part 2: From Cardiac Complications To Pediatric ManifestationsDocument27 pagesMultisystem Imaging Manifesta-Tions of COVID-19, Part 2: From Cardiac Complications To Pediatric ManifestationsAdiel OjedaNo ratings yet
- Adults 4Document7 pagesAdults 4Bshara SleemNo ratings yet
- Association of History of CVD With Severity of COVID 19Document13 pagesAssociation of History of CVD With Severity of COVID 19claudiam.chavezvNo ratings yet
- Covid y CorazónDocument16 pagesCovid y CorazóndanielaNo ratings yet
- Scutelnic-Heldner2020 Article VascularEventsVascularDiseaseADocument16 pagesScutelnic-Heldner2020 Article VascularEventsVascularDiseaseAdenisNo ratings yet
- ARDS Causes Diffuse Alveolar Damage in The LungDocument5 pagesARDS Causes Diffuse Alveolar Damage in The LungArfyanda ZakariaNo ratings yet
- 1 s2.0 S1201971222004982 MainDocument10 pages1 s2.0 S1201971222004982 MainBazartseren BoldgivNo ratings yet
- Jama Wiersinga 2020 RV 200009 1597950376.62291Document12 pagesJama Wiersinga 2020 RV 200009 1597950376.62291Iziza LunaskhiNo ratings yet
- (RCT) Cardiovascular Injuries After Covid-19 InfectionDocument7 pages(RCT) Cardiovascular Injuries After Covid-19 InfectionPatrick NunsioNo ratings yet
- Song 2020 Cytokine Storm Induced by Sars CovDocument16 pagesSong 2020 Cytokine Storm Induced by Sars CovSusanyi ErvinNo ratings yet
- D-Dimer As An Indicator of Prognosis in Sars-Cov-2 Infection: A Systematic ReviewDocument10 pagesD-Dimer As An Indicator of Prognosis in Sars-Cov-2 Infection: A Systematic ReviewIraNo ratings yet
- How To Read A Next-Generation Sequencing Report-What Oncologists Need To KnowDocument9 pagesHow To Read A Next-Generation Sequencing Report-What Oncologists Need To KnowsamuelNo ratings yet
- Health Status of Aged Women With or Without The Experience of Practicing YogaDocument8 pagesHealth Status of Aged Women With or Without The Experience of Practicing YogasamuelNo ratings yet
- Evaluation of The Effectiveness of Two New Strains of Lactobacillus On Obesity-Induced Kidney Diseases in BALBc MiceDocument8 pagesEvaluation of The Effectiveness of Two New Strains of Lactobacillus On Obesity-Induced Kidney Diseases in BALBc MicesamuelNo ratings yet
- Endothelial Dysfunction in COVID-19 Potential Mechanisms and Possible Therapeutic OptionsDocument24 pagesEndothelial Dysfunction in COVID-19 Potential Mechanisms and Possible Therapeutic OptionssamuelNo ratings yet
- BiomedicinesDocument12 pagesBiomedicinessamuelNo ratings yet
- Empagliflozin Is Not Renoprotective in Non-Diabetic Rat Models of Chronic Kidney DiseaseDocument14 pagesEmpagliflozin Is Not Renoprotective in Non-Diabetic Rat Models of Chronic Kidney DiseasesamuelNo ratings yet
- Evolution of Mineralocorticoid Receptor Antagonists in The Treatment of Chronic Kidney Disease Associated With Type 2 Diabetes MellitusDocument16 pagesEvolution of Mineralocorticoid Receptor Antagonists in The Treatment of Chronic Kidney Disease Associated With Type 2 Diabetes MellitussamuelNo ratings yet
- Clinical Outcomes Among Patients With 1-Year Survival Following Intensive Care Unit Treatment For COVID-19Document7 pagesClinical Outcomes Among Patients With 1-Year Survival Following Intensive Care Unit Treatment For COVID-19samuelNo ratings yet
- A Multidisciplinary Approach and Current Perspective of Nonalcoholic Fatty Liver Disease A Systematic ReviewDocument12 pagesA Multidisciplinary Approach and Current Perspective of Nonalcoholic Fatty Liver Disease A Systematic ReviewsamuelNo ratings yet
- EULAR Points To Consider When Analysing and Reporting Comparative Effectiveness Research Using Observational Data in RheumatologyDocument6 pagesEULAR Points To Consider When Analysing and Reporting Comparative Effectiveness Research Using Observational Data in RheumatologysamuelNo ratings yet
- Standards of Medical Care in Diabetes - 2022Document22 pagesStandards of Medical Care in Diabetes - 2022samuelNo ratings yet
- Surgical Management of Axilla of Triple-Negative Breast Cancer in The Z1071 Era: A Propensity Score-Matched Analysis of The National Cancer DatabaseDocument13 pagesSurgical Management of Axilla of Triple-Negative Breast Cancer in The Z1071 Era: A Propensity Score-Matched Analysis of The National Cancer DatabasesamuelNo ratings yet
- Changes in The Abdominal Wall After Anterior, Posterior, and Combined Component SeparationDocument11 pagesChanges in The Abdominal Wall After Anterior, Posterior, and Combined Component SeparationsamuelNo ratings yet
- Infeccion Por Gram NegativosDocument12 pagesInfeccion Por Gram NegativossamuelNo ratings yet
- Best Practice & Research Clinical Rheumatology: John Stack, Geraldine MccarthyDocument8 pagesBest Practice & Research Clinical Rheumatology: John Stack, Geraldine MccarthysamuelNo ratings yet
- COVID-19 and Coagulopathy: Malay Sarkar - Irappa V. Madabhavi - Pham Nguyen Quy - Manjunath B. GovindagoudarDocument16 pagesCOVID-19 and Coagulopathy: Malay Sarkar - Irappa V. Madabhavi - Pham Nguyen Quy - Manjunath B. GovindagoudarsamuelNo ratings yet
- Patterns of Ischemic Posterior Circulation Strokes: A Clinical, Anatomical, and Radiological ReviewDocument9 pagesPatterns of Ischemic Posterior Circulation Strokes: A Clinical, Anatomical, and Radiological ReviewsamuelNo ratings yet
- Clinical Reasoning: Rare Cause of Hemiparesis and Ataxia in A 36-Year-Old ManDocument8 pagesClinical Reasoning: Rare Cause of Hemiparesis and Ataxia in A 36-Year-Old MansamuelNo ratings yet
- AGA Clinical Practice Guideline On The Management of Coagulation Disorders in Patients With CirrhosisDocument14 pagesAGA Clinical Practice Guideline On The Management of Coagulation Disorders in Patients With CirrhosissamuelNo ratings yet
- Articles: BackgroundDocument8 pagesArticles: BackgroundsamuelNo ratings yet
- Acuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiesDocument16 pagesAcuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiessamuelNo ratings yet
- Management of Acute Upper Gastrointestinal Bleeding: Urgent Versus Early EndosDocument5 pagesManagement of Acute Upper Gastrointestinal Bleeding: Urgent Versus Early EndossamuelNo ratings yet
- Registration Successful - Registration For Inter-District Movement With-In Uttarakhand PDFDocument2 pagesRegistration Successful - Registration For Inter-District Movement With-In Uttarakhand PDFPrakhar AgarwalNo ratings yet
- Choral Singing in The Time of COVID-19Document6 pagesChoral Singing in The Time of COVID-19Victor C100% (1)
- Who Calls The Shots? Climate of Change Nipped in The BudDocument26 pagesWho Calls The Shots? Climate of Change Nipped in The BudJHONY SALCEDO MARTINEZNo ratings yet
- Business Standards 27th MayDocument18 pagesBusiness Standards 27th MaydevNo ratings yet
- Broadcaster Summer 2020Document21 pagesBroadcaster Summer 2020ConcordiaNebraskaNo ratings yet
- In Response To Covid-19: Hcs Reopening Plan Fall 2020: Motivated - Dedicated - EducatedDocument46 pagesIn Response To Covid-19: Hcs Reopening Plan Fall 2020: Motivated - Dedicated - EducatedNews 8 WROCNo ratings yet
- MoralagentdoxDocument12 pagesMoralagentdoxMirafelNo ratings yet
- Benefits and Contributions Schedule 2021Document72 pagesBenefits and Contributions Schedule 2021MarcoNo ratings yet
- Outpatient Otolaryngology in The Era of COVID-19: A Data-Driven Analysis of Practice PatternsDocument7 pagesOutpatient Otolaryngology in The Era of COVID-19: A Data-Driven Analysis of Practice PatternsMada Dwi HariNo ratings yet
- Chamber-DM Health Department LetterDocument2 pagesChamber-DM Health Department LetterNBC MontanaNo ratings yet
- English 8 Q1 - M1 FinalDocument21 pagesEnglish 8 Q1 - M1 FinalMJ Zarate100% (3)
- Acute Prescribing - Challenges and Solutions - Ajit KulkarniDocument51 pagesAcute Prescribing - Challenges and Solutions - Ajit KulkarniAgha QaimiNo ratings yet
- Journal Pre-Proof: International Journal of Antimicrobial AgentsDocument9 pagesJournal Pre-Proof: International Journal of Antimicrobial AgentsBeatrizNo ratings yet
- Department of Education: Republic of The PhilippinesDocument35 pagesDepartment of Education: Republic of The PhilippinesJerson S. SantiagoNo ratings yet
- During The Holiday Weekend Second Home-Owners Are Allowed in Tahoe Tourists Are Still Not Allowed at This Time FINALDocument2 pagesDuring The Holiday Weekend Second Home-Owners Are Allowed in Tahoe Tourists Are Still Not Allowed at This Time FINALFOX40 NewsNo ratings yet
- Rotogravure Printing Machine, Flexo Printing Machine, Coating Machine, Dry Lamination Machine, Solvent-Less Laminator Suppliers, ShaanxibeirenDocument6 pagesRotogravure Printing Machine, Flexo Printing Machine, Coating Machine, Dry Lamination Machine, Solvent-Less Laminator Suppliers, ShaanxibeirenFoufou IshakNo ratings yet
- Role of The Pharmacist During The COVID-19 PandemiDocument10 pagesRole of The Pharmacist During The COVID-19 Pandemiallen reyesNo ratings yet
- Guidelines For Dental ServicesDocument6 pagesGuidelines For Dental Servicesdruzair007No ratings yet
- Metro Recovery Task Force Progress Report 2Document37 pagesMetro Recovery Task Force Progress Report 2Metro Los AngelesNo ratings yet
- 29-09-2020 HMB EnglishDocument22 pages29-09-2020 HMB EnglishNeeraj S GNo ratings yet
- Cebu Youth Mental Health Conference-FridayDocument2 pagesCebu Youth Mental Health Conference-FridayDyanne BautistaNo ratings yet
- Safety On Accident Site:: Bloodborne Pathogen AwarenessDocument69 pagesSafety On Accident Site:: Bloodborne Pathogen Awarenessdaily absurdNo ratings yet
- Uninsured Patient Covid Services PosterDocument1 pageUninsured Patient Covid Services PosterIndiana Family to FamilyNo ratings yet
- The Effect of COVID-19 On The Hospitality IndustryDocument17 pagesThe Effect of COVID-19 On The Hospitality Industryhehe20211742No ratings yet
- Reviews: COVID-19 and Cardiovascular Disease: From Basic Mechanisms To Clinical PerspectivesDocument16 pagesReviews: COVID-19 and Cardiovascular Disease: From Basic Mechanisms To Clinical PerspectivesLAURA ALEJANDRA PARRA GOMEZNo ratings yet
- CDC MMWR Coronavirus Prisons StudyDocument5 pagesCDC MMWR Coronavirus Prisons StudyStephen LoiaconiNo ratings yet
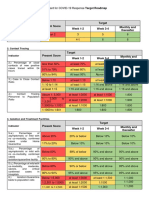
- Present Score Target Week 1-2 Week 3-4 Monthly and ThereafterDocument2 pagesPresent Score Target Week 1-2 Week 3-4 Monthly and ThereafterFret Ramirez Coronia RNNo ratings yet