Download as pdf or txt
You might also like
- Movie Recommendation SystemDocument41 pagesMovie Recommendation SystemSowmya Srinivasan100% (3)
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- ACLS Study Guide NewDocument35 pagesACLS Study Guide NewNIRANJANA SHALINI100% (1)
- Lower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsDocument59 pagesLower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsJamsidul Hassan RajibNo ratings yet
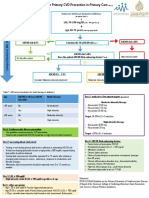
- Algoritma StatinDocument1 pageAlgoritma StatinAgnes Irene ZagotoNo ratings yet
- NACHC Statin Guideline Snapshot GenericDocument14 pagesNACHC Statin Guideline Snapshot GenericSaad KhanNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- Nicotinic Acid 10-20% 10-20% 14-35% 30-70% Reasonable To PoorDocument5 pagesNicotinic Acid 10-20% 10-20% 14-35% 30-70% Reasonable To PoorvmvlivNo ratings yet
- 2013 Cholesterol Guidelines at A Glance: - Robert Barnes, M3Document15 pages2013 Cholesterol Guidelines at A Glance: - Robert Barnes, M3CoolrobertizNo ratings yet
- Lipids Topic DiscussionDocument10 pagesLipids Topic Discussionapi-665372449No ratings yet
- Dyslipidemia Final Poster June 24Document2 pagesDyslipidemia Final Poster June 24drabdulrabbNo ratings yet
- HIPERLIPIDEMIADocument10 pagesHIPERLIPIDEMIAMarianaNo ratings yet
- Drogas en Dislipidemia para Prevemncion CVDocument19 pagesDrogas en Dislipidemia para Prevemncion CVeleanhy95No ratings yet
- ATP IV HandoutDocument2 pagesATP IV Handouthafidzz1No ratings yet
- Intensity of Cholesterol Lowering With Statin in PatientsDocument23 pagesIntensity of Cholesterol Lowering With Statin in Patientsandri ansyahNo ratings yet
- Ascvd PrimaryDocument21 pagesAscvd Primaryprk prkNo ratings yet
- Atherosclerotic Cardiovascular Disease (ASCVD) Primary Prevention GuidelineDocument21 pagesAtherosclerotic Cardiovascular Disease (ASCVD) Primary Prevention GuidelineHeryanti PusparisaNo ratings yet
- Understanding The Needs of The High Productive DyslipidemiaDocument47 pagesUnderstanding The Needs of The High Productive DyslipidemiachchchchkNo ratings yet
- Ongoing Therapy and MonitoringDocument1 pageOngoing Therapy and MonitoringDaveMartoneNo ratings yet
- Dyslipidemia - 2Document17 pagesDyslipidemia - 2Mohamed AbouzaidNo ratings yet
- JNC 8 PDFDocument15 pagesJNC 8 PDFcut herlindaNo ratings yet
- Management of Blood Cholesterol 2019Document2 pagesManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassNo ratings yet
- 10-Year Risk of Fatal CVD Is Based On Risk Factors: Age, Smoking, Sex, Systolic Blood Pressure and Total CholesterolDocument3 pages10-Year Risk of Fatal CVD Is Based On Risk Factors: Age, Smoking, Sex, Systolic Blood Pressure and Total CholesterolDidik SiswandoroNo ratings yet
- Dyslipidemia ATP4 GUIDLINESDocument9 pagesDyslipidemia ATP4 GUIDLINESSandy GunawanNo ratings yet
- Guidelines DyslipidDocument49 pagesGuidelines Dyslipidnoveldycb89No ratings yet
- 2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"Document51 pages2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"dr_yasserNo ratings yet
- Dyslipidaemia 2019Document61 pagesDyslipidaemia 2019fatima.shqeratNo ratings yet
- Guidelines Made Simple Tool 2018 CholesterolDocument22 pagesGuidelines Made Simple Tool 2018 CholesterolHussain HameedNo ratings yet
- 2018 Cholesterol Guidelines Made Simple ToolDocument22 pages2018 Cholesterol Guidelines Made Simple ToolLeoberto Batista Pereira SobrinhoNo ratings yet
- Role of Rosuvastatin in The Treatment of DyslipidemiaDocument16 pagesRole of Rosuvastatin in The Treatment of DyslipidemiaabcdefNo ratings yet
- LipidsupdateDocument23 pagesLipidsupdatedrshekarforyouNo ratings yet
- Variability of Low-Density Lipoprotein Cholesterol Response With Different Doses of Atorvastatin, Rosuvastatin, and Simvastatin: Results From VoyagerDocument6 pagesVariability of Low-Density Lipoprotein Cholesterol Response With Different Doses of Atorvastatin, Rosuvastatin, and Simvastatin: Results From Voyagerfaradila cahyaniNo ratings yet
- 2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryDocument77 pages2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryBetsy Brown ByersmithNo ratings yet
- Beyond Statins - NEW AHA/ACC Cholesterol Guidelines: Diane Osborn ARNP, CLSDocument54 pagesBeyond Statins - NEW AHA/ACC Cholesterol Guidelines: Diane Osborn ARNP, CLSDilan GalaryNo ratings yet
- Global Risk of Cardiovascular Disease: Assessment and ApplicationDocument18 pagesGlobal Risk of Cardiovascular Disease: Assessment and ApplicationEmdan SengadjiNo ratings yet
- 2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/ Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryDocument77 pages2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/ Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummarydanielNo ratings yet
- Lipid ManagementDocument2 pagesLipid ManagementMedicina FamiliarNo ratings yet
- A Pragmatic View of The New Cholesterol Treatment GuidelinesDocument4 pagesA Pragmatic View of The New Cholesterol Treatment GuidelinesMaria Fernanda CoralNo ratings yet
- Cholesterol Management: ACC/AHA Updates Guideline: Practice GuidelinesDocument2 pagesCholesterol Management: ACC/AHA Updates Guideline: Practice GuidelinesNikita ShakyaNo ratings yet
- Cholesterol Guidelines Review 2020Document6 pagesCholesterol Guidelines Review 2020oriannaocantoNo ratings yet
- Hyperlipidemia - Drugs For Cardiovascular Risk Reduction in AdultsDocument12 pagesHyperlipidemia - Drugs For Cardiovascular Risk Reduction in AdultssuperkshiluppyNo ratings yet
- New Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesDocument6 pagesNew Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesJustinaNo ratings yet
- Clinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Document61 pagesClinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Bassant Ahmed Mahmoud Ragab Abdallah AyaadNo ratings yet
- Final Hyperlipidaemia GuidelinesDocument2 pagesFinal Hyperlipidaemia Guidelinesalialison7666No ratings yet
- Guidelines Made Simple Tool 2018 CholesterolDocument22 pagesGuidelines Made Simple Tool 2018 CholesterolMuhammad Ali Ridho ShahabNo ratings yet
- What's New in Lipid GuidelinesDocument31 pagesWhat's New in Lipid GuidelinesYunita WidyaningsihNo ratings yet
- Guidelines Made Simple Tool 2018 CholesterolDocument22 pagesGuidelines Made Simple Tool 2018 CholesterolSafira HalimatussadiahNo ratings yet
- AtorvastatinDocument7 pagesAtorvastatinKrima PatelNo ratings yet
- Management of Dyslipidemia and The Prevention of Cardiovascular DiseaseDocument2 pagesManagement of Dyslipidemia and The Prevention of Cardiovascular DiseaseBenny TrisaktyariNo ratings yet
- Aha Guidelinedriven Management of Hypertension An Evidencebased UpdateDocument56 pagesAha Guidelinedriven Management of Hypertension An Evidencebased UpdateNanda Gopal Reddy AnamNo ratings yet
- StatinsUpdate FINAL PDFDocument24 pagesStatinsUpdate FINAL PDFanthonyNo ratings yet
- PH Errata V1Document18 pagesPH Errata V1kelvinNo ratings yet
- 2017 DCP 1. Telmisartan Untuk KasusDocument26 pages2017 DCP 1. Telmisartan Untuk KasusOcto IndradjajaNo ratings yet
- Screening and Management of Lipids: Patient Population: ObjectiveDocument20 pagesScreening and Management of Lipids: Patient Population: ObjectiveKatie Kroll BradyNo ratings yet
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNo ratings yet
- Baseline Low-Density LipoproteinDocument9 pagesBaseline Low-Density LipoproteinjoNo ratings yet
- Lipid ManagementDocument58 pagesLipid ManagementDenti NugraheniNo ratings yet
- Dyslipedemia ShortDocument5 pagesDyslipedemia Shortذوالفقار أحمدNo ratings yet
- Lipids JBDocument48 pagesLipids JBMuvenn KannanNo ratings yet
- Diabetes Algorithm Executive SummaryDocument30 pagesDiabetes Algorithm Executive SummaryLuis Alberto Alvarez AnkassNo ratings yet
- Cholesterol-Lowering Agents Statins-For Everyone? 2019Document10 pagesCholesterol-Lowering Agents Statins-For Everyone? 2019Luis Alberto Alvarez AnkassNo ratings yet
- Coagulacion Intravascular Diseminada PDFDocument12 pagesCoagulacion Intravascular Diseminada PDFLuis Alberto Alvarez AnkassNo ratings yet
- Management of Blood Cholesterol 2019Document2 pagesManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassNo ratings yet
- Aspirin For Primary Prevention of Atherosclerotic Cardiovascular Disease 2016Document10 pagesAspirin For Primary Prevention of Atherosclerotic Cardiovascular Disease 2016Luis Alberto Alvarez AnkassNo ratings yet
- Ecv Aha Recovery 2016Document73 pagesEcv Aha Recovery 2016Luis Alberto Alvarez AnkassNo ratings yet
- Manulife Smart Call Call MenuDocument1 pageManulife Smart Call Call MenuNazreen AmirdeenNo ratings yet
- 74 HCT 148Document11 pages74 HCT 148Merényi OszkárNo ratings yet
- FEA - Calculation of The Hydroforming Process With LS-DYNADocument8 pagesFEA - Calculation of The Hydroforming Process With LS-DYNAadrianNo ratings yet
- Curriculum VitaeDocument3 pagesCurriculum Vitaenotapernota101100% (2)
- Adaptable Multi Nut Fastner With Manual Height Adjustment SystemDocument48 pagesAdaptable Multi Nut Fastner With Manual Height Adjustment SystemANAND KRISHNANNo ratings yet
- KickStart 19Document2 pagesKickStart 19Venu GopalNo ratings yet
- Braille Actuator Report MAJORDocument32 pagesBraille Actuator Report MAJORSwapnil BeheraNo ratings yet
- Temidayo Cybercrime ReportDocument13 pagesTemidayo Cybercrime ReportMAYOWA ADEBAYONo ratings yet
- IMS JRDocument4 pagesIMS JRRyoNo ratings yet
- Mr. Anil Wanarse PatilDocument29 pagesMr. Anil Wanarse PatilANIL INTERAVIONNo ratings yet
- PNP ACG - Understanding Digital ForensicsDocument76 pagesPNP ACG - Understanding Digital ForensicsTin TinNo ratings yet
- OSINTDocument49 pagesOSINTMARCUS VINICIUSNo ratings yet
- Ema Emits: UndergraduateDocument7 pagesEma Emits: UndergraduateJanineNo ratings yet
- A Comprehensive Guide To Oil Sight GlassesDocument15 pagesA Comprehensive Guide To Oil Sight GlassesTalha NizamiNo ratings yet
- 3 Odometer DisclosureDocument1 page3 Odometer DisclosureJuan Carlos MartinezNo ratings yet
- UMAM Fee Structure EditedVer2Document1 pageUMAM Fee Structure EditedVer2AKMA SAUPINo ratings yet
- Q PapersDocument53 pagesQ PapersTanu RdNo ratings yet
- Edu 3 AssDocument19 pagesEdu 3 Assparvathy bNo ratings yet
- Lesson 10b: Aggregate Planning Finding An Optimal Production Plan Using Excel SolverDocument7 pagesLesson 10b: Aggregate Planning Finding An Optimal Production Plan Using Excel SolvervaraduNo ratings yet
- Dynamic Simulation of A Crude Oil DistillationDocument14 pagesDynamic Simulation of A Crude Oil DistillationAL-JABERI SADEQ AMEEN ABDO / UPMNo ratings yet
- Business Unit Performance Measurement: Mcgraw-Hill/IrwinDocument17 pagesBusiness Unit Performance Measurement: Mcgraw-Hill/Irwinimran_chaudhryNo ratings yet
- Parallelizing Partial Digest Problem On Multicore System PDFDocument10 pagesParallelizing Partial Digest Problem On Multicore System PDFnazibNo ratings yet
- Salen WWE Offer LetterDocument3 pagesSalen WWE Offer LetterHeel By NatureNo ratings yet
- Nguyễn Triệu Anh: Education And Degree Work ExperiencesDocument1 pageNguyễn Triệu Anh: Education And Degree Work ExperiencesQuach Manh ThuongNo ratings yet
- Manual de Usuario Motor Fuera de Borda.Document68 pagesManual de Usuario Motor Fuera de Borda.Carlos GallardoNo ratings yet
- 2 BHK Price List & Floor PlanDocument1 page2 BHK Price List & Floor PlanRajesh K SinghNo ratings yet
- Music and Me Instructions 2021Document3 pagesMusic and Me Instructions 2021api-497020000No ratings yet
- Final Report (NTCC) IoTDocument11 pagesFinal Report (NTCC) IoTSyed MehsherNo ratings yet