Professional Documents
Culture Documents
Abiraterone Acetate in Combination With Prednisone in The Treatment of Prostate Cancer: Safety and Efficacy
Abiraterone Acetate in Combination With Prednisone in The Treatment of Prostate Cancer: Safety and Efficacy
Uploaded by
Yusuf RachmanOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Abiraterone Acetate in Combination With Prednisone in The Treatment of Prostate Cancer: Safety and Efficacy
Abiraterone Acetate in Combination With Prednisone in The Treatment of Prostate Cancer: Safety and Efficacy
Uploaded by
Yusuf RachmanCopyright:
Available Formats
Expert Review of Anticancer Therapy
ISSN: (Print) (Online) Journal homepage: https://www.tandfonline.com/loi/iery20
Abiraterone acetate in combination with
prednisone in the treatment of prostate cancer:
safety and efficacy
Cécile Manceau , Loic Mourey , Damien Pouessel & Guillaume Ploussard
To cite this article: Cécile Manceau , Loic Mourey , Damien Pouessel & Guillaume Ploussard
(2020): Abiraterone acetate in combination with prednisone in the treatment of prostate cancer:
safety and efficacy, Expert Review of Anticancer Therapy, DOI: 10.1080/14737140.2020.1785289
To link to this article: https://doi.org/10.1080/14737140.2020.1785289
Accepted author version posted online: 18
Jun 2020.
Submit your article to this journal
View related articles
View Crossmark data
Full Terms & Conditions of access and use can be found at
https://www.tandfonline.com/action/journalInformation?journalCode=iery20
Publisher: Taylor & Francis & Informa UK Limited, trading as Taylor & Francis Group
Journal: Expert Review of Anticancer Therapy
DOI: 10.1080/14737140.2020.1785289
Abiraterone acetate in combination with prednisone in the treatment of prostate cancer: safety
and efficacy
*Cécile Manceau 1, Loic Mourey 3, Damien Pouessel 3, Guillaume Ploussard 2
T
1. Department of Urology, CHU-IUCT Oncopole, Toulouse, France
IP
2. Department of Urology, La Croix du Sud Hospital, Quint Fonsegrives, France
3. Department of Medical Oncology, Institut Claudius Régaud, IUCT Oncopole, Toulouse, France
R
*Corresponding author: Cecile.manceau2@gmail.com
SC
U
AN
M
D
TE
EP
C
AC
Information Classification: General
Abstract
Introduction: Metastatic prostate cancer is a life-threatening disease and an important public health
concern with prevalence rates varying drastically between high- and low-income countries.
Androgen-deprivation therapy alone has been the first-line treatment option for decades,
temporarily controlling disease until invariable tumor regression. At the castration-resistant stage,
metastatic disease becomes lethal. In recent years several new treatments, including second-
T
IP
generation hormone therapies, have proven to be life-prolonging in metastatic castration-resistant
prostate cancer, and at an earlier hormone-sensitive stage. Abiraterone acetate in combination with
R
prednisone was the first approved hormone therapy demonstrating survival benefit, and represents,
SC
to date, an alternative or a second-line treatment after taxane-based chemotherapy, in addition to
androgen-deprivation therapy, in hormone sensitive and metastatic castration-resistant prostate
U
AN
cancer.
Area covered: We performed a literature review of papers from 2012 to 2020 using PubMed, Web of
M
Science, and Embase searching for the safety and efficacy of abiraterone acetate in prostate cancer
management. Search results were limited to phase III-IV trials and post-hoc analysis of Phase III trials
D
evaluated Abiraterone acetate in the English language.
TE
Expert opinion: This literature review confirms the role of abiraterone acetate in the therapeutic
EP
landscape with well-proven safety and efficacy, demonstrated in trials and post-approval studies.
C
Keywords: Abiraterone acetate, second-generation androgen receptor inhibitor, metastatic
resistant-castration prostate cancer, metastatic castration-sensitive prostate cancer; prostate cancer
AC
Information Classification: General
Article highlights
- Abiraterone acetate is a second-generation hormone therapy, orally available with a good
safety profile and overall survival benefits in metastatic prostate cancer
- Abiraterone acetate is an improvement for metastatic prostate cancer prognosis and patient
well-being
T
-
IP
Abiraterone acetate is a less aggressive alternative to taxane-based chemotherapy
R
SC
U
AN
M
D
TE
EP
C
AC
Information Classification: General
1. INTRODUCTION
Prostate cancer (PCa) is the second most common cancer worldwide and the fifth leading cause of
death from cancer among men [1]. Metastatic prostate cancer still represents a lethal disease
despite strong developments in the therapeutic arsenal during the last decade. Since the works of
Huggins and Hodges [2], androgen suppression has become the cornerstone of metastatic stage
T
IP
treatment allowing control of disease until invariable progression to the castration-resistant stage.
Recent years has seen significant changes for the treatment of advanced and metastatic prostate
R
cancer with the approval of several new drugs, including chemotherapy (docetaxel, cabazitaxel),
SC
bone-targeted therapies (radium-223), vaccination (sipuleucel-T), and new generation hormone
therapies (abiraterone acetate, enzalutamide). All these drugs have proven to be life-prolonging in
U
AN
randomized controlled trials.
Actually, abiraterone acetate (AA) in combination with prednisone and luteinizing hormone-releasing
M
hormone (LHRH) agonists or antagonists is a recommended treatment option in men with metastatic
castration-resistant prostate cancer (mCRPC) and metastatic castration-sensitive prostate cancer
D
(mCSPC).
TE
The aim of this literature review was to present strong evidence data about the efficacy and safety of
EP
abiraterone acetate including its mechanisms of action and side effects, in both CRPC and CSPC
stages.
C
AC
Information Classification: General
2. MECHANISM OF ACTION
Firstly, the androgen receptor (AR) has been known for many years to be a regulator in PCa from
disease development to progression and treatment [2]. Androgen deprivation therapy (ADT) with
LHRH analogs and anti-androgens allow a suppression of circulating testosterone levels, blocks
transcriptional activity of AR and temporary tumor regression. Then, there is an AR reactivation in
T
IP
response to ADT with new AR signaling. Multiple mechanisms have been identified to explain this
phenomenon including AR gene mutation, overexpression, AR splice variants expression and the
R
expression of transcriptional co-activators overexpressing androgen dependent genes [3]. Moreover,
SC
intraprostatic cells can be a significant source of androgen under the selective pressure of endocrine
therapy [4].
U
AN
AA is a new molecular entity for blocking AR expression [5], orally available.
AA is converted in vivo to abiraterone which is a selective and irreversible 17 α-hydroxylase/C17,20
M
lyase (CYP17A1) inhibitor.
CYP17A1 is an enzyme expressed in steroidogenic tissue like testes and adrenal cortex. It’s also
D
expressed in prostatic tumor tissue. This enzyme is involved in conversion of cholesterol to the
TE
androgen precursor and steroid hormone synthesis. The generation of glucocorticoid such as cortisol
EP
requires 17 α-hydroxylase as it converts pregnenolone and progesterone to 17-hydroxypregnenolone
and 17-hydroxyprogesterone. So, 17 α-hydroxylase deficiency impairs glucocorticoids production,
C
pregnenolone and progesterone increase. The decrease in cortisol levels includes a compensatory
AC
increase in adrenocorticotropic hormone (ACTH) and the increase in pregnenolone and progesterone
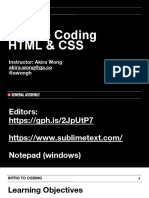
is treated to form mineralocorticoids [6]. Prednisone is associated to compensate cortisol reduction
due to 17 α-hydroxylase inhibition, therefore, decreasing the mineralocorticoid excess [6] (Fig 1).
Along with 17 α-hydroxylase, C17,20 lyase is required for the production of androgenic sex steroid.
Pregnenolone to 17-hydroxypregnenolone is converted by 17 α-hydroxylase, C17,20 lyase next
converts 17-hydroxypregnenolone to dehydroepiandrosterone (DHEA), a precursor of
Information Classification: General
dihydrotestosterone. So, abiraterone inhibits synthesis of dihydrotestosterone (DHT) and reduces
production of androgens in the tumor tissue [7].
T
IP
3. MAIN SIDE EFFECTS
R
Mechanisms of action of AA explain some adverse effects like excess mineralocorticoids and
SC
adrenocortical insufficiency, but clinical studies and post-approval studies identified other adverse
effects like hepatotoxicity and cardiac disorders. Prednisone association and glucocorticoid adverse
U
AN
effects were also studied.
M
a. Mineralocorticoid excess
As pregnenolone and progesterone increase, so does mineralocorticoids which may cause
D
hypertension, hypokalemia, and fluid retention. This is why patients must be monitored at least once
TE
a month. Hypertension control and hypokalemia correction should be used, if necessary, during
EP
treatment.
For mCRPC, patients received AA with prednisone at a dose of 5 mg orally twice daily [8]. For mCSPC,
C
STAMPEDE and LATITUDE studies were designed with prednisone at a dose of 5 mg orally once a day
AC
[9,10]. Mineralocorticoid side effects were more frequent compared to COU301 and COU302 trials
(with prednisone at a dose of 5 mg twice a day) but this increase could be explained by lower steroid
doses but also longer exposure to AA.
Grade 3-4 hypertension were observed in 2 to 10% of patients grade 3-4 hypokalemia in 3-10%, and
fluid retention in 1-3% [9–12]. Tension, hypokalemia and fluid retention have to be monitored at
Information Classification: General
least once a month. These adverse events can easily be managed medically by patient monitoring.
For example, oral potassium supplementation, anti-hypertensive agent.
b. Adrenocortical insufficiency
Prednisone is associated with AA to compensate cortisol reduction due to 17 α-hydroxylase
inhibition. However, steroid interruption or stress or infection could lead to an adrenocortical
T
IP
insufficiency. Adrenocortical insufficiency has rarely occurred (0,3% in clinical studies according to
the prescribing information) highlighted by two cases in literature [13]. It was reported when
R
patient interrupted prednisone along with abnormal stress or infection. During AA treatment in
SC
combination with prednisone, special monitoring is not recommended, increased dosage of
corticosteroids may be indicated before, during and after stressful situations.
U
AN
c. Hepatotoxicity
M
AA can be associated with hepatic toxicity and aminotransferase level elevation. In clinical trials 6%
of patients were reported to have grade 3-4 hepatic disorders without deaths but patients displayed
D
fulminant hepatitis, acute liver failure and deaths in post-approval studies. These disorders appeared
TE
typically during the first 3 months after starting treatment. Aminotransferase and bilirubin levels
EP
have to be measured prior to starting treatment and every two weeks for the first three months of
treatment and monthly after. Hepatotoxicity may lead to interruption, reduced dose level, or, to
C
permanently discontinued treatment.
AC
d. Cardiac disorders
Cardiac disorder in AA plus prednisone versus prednisone-only groups were rare. The most
frequently observed cardiac events were grade 1 and 2 tachycardia events and grade 3 or lower
atrial fibrillation events. Moreover, hypokalemia can lead to heart rhythm disorders. Recent meta-
analysis included prospective studies and showed that use of new hormonal agents was associated
Information Classification: General
with an increased risk of all-grade (Risk Ratio (RR), 1.36) and high-grade (RR, 1.84) cardiac toxicity
[14].
Patients with severe heart failure NYHA III-IV or with left ventricular ejection fraction <50% were
excluded from clinical trial, so can’t safety be defined. Post-approval studies identified torsade de
pointe and QT prolongation in patients with hypokalemia or had underlying cardiovascular condition.
T
IP
e. Glucocorticoid adverse effects
The use of glucocorticoid replacement therapy with prednisone low dose, may restore normal
R
physiology while minimizing adverse effects. It compensates for the abiraterone-induced reduction
SC
in serum cortisol, normalizes the abiraterone-induced rise in ACTH [6,12]. With this low dose
compared with the dose used to treat autoimmune or cancer disorders, the mineralocorticoid
U
AN
activity of prednisone is minimal. The two most common any-grade corticoid adverse effect were
hyperglycemia (7.8%), and weight increase 3,9%. Other any-grade AEs occurred in 1% of patients
M
[15].The cumulative dose over a prolonged treatment period may alter bone metabolism,
hyperglycemia, diabetes, immunosuppression, muscle sickness, negative effect on mood and
D
cognitive function.
TE
EP
f. Abiraterone in elderly (≥75 Years)
C
In clinical trial, elderly patient in both arms of the study (with and without AA) had higher rates of
AC
fluid retention and cardiac disorder, specific adverse effect were similar between age subgroup
[16,17].
A recent, multicentre, phase IV study has confirmed the safety of abiraterone acetate in mCRPC [18].
In this study, adverse effects and impacts on quality-of-life have been prospectively assessed in
comparison with enzalutamide, another new generation hormone therapy. Patient-reported
Information Classification: General
outcome items such as cognitive impairments and fatigue were significantly in favour of abiraterone
versus enzalutamide without any treatment-related death. Thus, real-world, post-approval studies
confirmed the mid-term safety of abiraterone acetate and its potential advantages compared with
other hormonal therapies.
AA is well tolerated with adverse effects being predominantly grade 1 or 2. Principal toxicities can be
T
IP
successfully medically managed with patient monitoring and were generally reversible. AA was not
associated to any adverse hematological events.
R
Good tolerance was an important point for using this molecular entity for pathologies that were
SC
previously treated with cytotoxic chemotherapy only.
U
AN
M
D
TE
EP
C
AC
Information Classification: General
5. DRUG INTERACTION
AA involves hepatic metabolism and liver enzymes belonging to the cytochrome P450 (CYP450)
family. In vitro studies showed that CYP1A2, CYP2C8, CYP2D6 are mainly inhibited by AA and CYP2C9;
CYP2C19 moderately. These enzymes play a role in metabolism of other drug classes like analgesics,
antidepressants, antidiabetics, lipid-lowering drug and cardiovascular drugs (beta blockers) [19].
CYP2D6 and CYP2C8 inhibition was shown in clinical studies [20,21], but CYP1A2 substrates were not
T
IP
increased [20]. CYP2D6 inhibition can decrease analgesic effect of codeine, antidepressant drugs
(paroxetine and tricyclic antidepressant) and amitriptyline. Additionally, CYP2C8 inhibition can
R
increase insulinotropic agent activity and AA increases the AUC of pioglitazone in healthy volunteers
SC
[21]. Yet no direct evidence has been provided between AA and repaglinide so this co-administration
should be monitored and switched to alternative recommended drugs in case of hypoglycemia.
U
AN
Abiraterone is metabolized in the liver in inactive compounds by CYP3A4. CYP3A4 inducers (like
rifampicine) decrease AA exposure by half [22]. In contrast, CYP3A4 inhibitors (like ketoconazole)
M
have no clinically significant impact on abiraterone exposure.
Post-approval studies didn’t report major problems but co-administration with analgesics,
D
antidepressants, antidiabetics, lipid-lowering drug and cardiovascular drugs should be closely
TE
monitored specifically for codeine, tricyclic antidepressant, pioglitazone, repaglinide, and CYP28
EP
statin substrate. These co-administrations must be considered when choosing among the different
new generation hormonal agents.
C
AC
Information Classification: General
6. METASTATIC CASTRATION-RESISTANT PROSTATE CANCER
AA in combination with prednisone is indicated for the treatment of patient with metastatic
castration-resistant prostate cancer (mCRPC).
Such recommendations have been based on two randomized, placebo-controlled, multinational,
phase 3 studies, the COU-AA-301 and the COU-AA-302 studies.
T
IP
COU-AA-301 was a multinational, randomized, double-blind, placebo-controlled, phase 3 study
including patients with mCRPC progression previously treated with docetaxel, with an Eastern
R
Cooperative Oncology Group (ECOG) between 0 and 2 (post-docetaxel setting).
SC
COU-AA-302 was a multinational, placebo-controlled, double-blind, randomized phase 3 study
including patients with asymptomatic or mildly symptomatic mCRPC who had not received previous
U
AN
chemotherapy and belonging to ECOG 0 or 1 (pre-docetaxel setting).
Both trials randomized patients to receive AA + prednisone twice a day, or placebo + prednisone
M
twice a day. Both studies showed an improvement in overall survival (OS) with AA independent of
the chemotherapy status.
D
In the final analysis of COU-AA-301 including 1195 patients. With a median follow-up of 20.2 months
TE
[11], median overall survival for the abiraterone group was longer than in the placebo group with a
EP
median OS increasing of 4.6 months for patients with mCRPC who had progressed post-docetaxel.
Median time to prostate specific antigen (PSA) progression increased to 1.9 months, with median
C
radiologic progression free survival (rPFS) set at 2 months. The survival benefit seen with abiraterone
AC
was consistent for the majority of subgroups but not for ECOG 2 patients, for patients who received
docetaxel for 3 months or less, and for patients who received 2 prior lines of chemotherapy at study
entry. In the subset of visceral diseases, the small sample size does not allow to conclude for the
primary endpoint but median OS was 12.9 months with AA and 8.3 months with prednisone alone
and rPFS, showing a statistical significance [23].
Information Classification: General
Secondary analysis observed an improvement in patient-reported fatigue intensity [24] and benefits
in patient-reported health-related quality of life (HRQoL) along with increasing delay in HRQoL
deterioration [25]. Bone-related symptoms (patient-reported pain palliation, delay in pain
progression, and delayed time to skeletal-related events) were favorably affected by AA treatment
[26].
Elderly patients derived clinical benefits similar to younger patients with increased hypertension,
T
IP
hypokalemia and cardiac disorders yet these observations were similar in the placebo group [16].
In the final analysis of COU-AA-302 including 1088 patients with mCRPC who had not received
R
previous chemotherapy and with a larger median follow up of 49.2 months, median OS for the
SC
abiraterone group was longer than in the placebo group with a median OS increasing by 4.4 months
[27]. Intermediary analysis with median follow up of 22.2 months did not find significant difference in
U
AN
OS while there was a significant difference in rPFS [28]. Subgroups analysis in intention to treat
population didn’t find significant difference in OS for patients ECOG 1, pain (brief pain inventory-
M
short form ≥2), age <65 years or presenting a high baseline PSA. Qualitatively, we conclude that
patients initially receiving prednisone alone subsequently received AA plus prednisone as crossover
D
per protocol (17%) or as a subsequent therapy (27%). Moreover, baseline serum PSA, bone
TE
metastases at baseline, and age were all significant prognostic factors for overall survival in
EP
multivariate analysis, only ECOG performance status score was not.
Regarding the co-primary endpoint, rPFS, with median follow up of 27.1 months, AA doubled time to
C
progression from 8.2 to 16.5 months [29]. Secondary analysis confirmed this rPFS improvement in all
AC
subgroups. Patients with mCRPC who had not received previous chemotherapy treated by AA also
reported statistically significant improvements in pain interference and functional status [29]. As
COU-AA-302, OS benefit were persistently for older patients [17].
Information Classification: General
To conclude, AA is a recommended, life-prolonging, well-tolerated, treatment option in mCRPC
patients before or after taxane-based chemotherapy. These encouraging results led to study AA at an
earlier stage for metastatic high-risk castration-sensitive prostate cancer.
T
IP
R
SC
U
AN
M
D
TE
EP
C
AC
Information Classification: General
7. METASTATIC HIGH-RISK CASTRATION-SENSITIVE PROSTATE CANCER
The benefit of AA in combination with prednisone was then investigated in two phase III trials for
patients with metastatic castration-sensitive prostate cancer (mCSPC).
LATITUDE is a randomly, double-blind, placebo-controlled, phase 3 trial [30]. Patients included were
newly diagnosed mCSPC patients with two of the three following high-risk factors associated with
T
IP
poor prognosis (a Gleason score of 8 or more, at least three bone lesions and the presence of
measurable visceral metastasis) and ECOG 0-2. A total of 1199 patients were randomly assigned in a
R
1:1 ratio to receive ADT + AA + prednisone once a day versus ADT + dual placebo.
SC
Final analysis with median follow-up of 51.8 months, showed a significantly longer OS (53.3% vs
36.5%) in the AA plus prednisone group with the median length of rPFS (the second primary
U
AN
endpoint) being 33 months in the abiraterone group and 14.8 months in the placebo group. This
benefit was consistent for the majority of subgroups.
M
Secondary analysis reported an improvement regarding time to pain progression (47.4 vs 16.6
months) and time to skeletal related events. The addition of abiraterone acetate delayed subsequent
D
prostate cancer therapy as well as the time of chemotherapy initiation. An exploratory analysis
TE
assessing the progression-free survival on subsequent treatment (named PFS2) also showed a
EP
significant PFS improvement in the abiraterone arm suggesting an advantage for early abiraterone
treatment.
C
Health-related quality of life (HRQOL), progression of pain, prostate cancer symptoms, fatigue and
AC
functional decline were also evaluated. There were improvements of pain, fatigue symptoms and
overall HRQOL by using abiraterone acetate. Patients in the abiraterone group had longer median
time to worst pain intensity progression, worst fatigue intensity progression and functional
deterioration status [20].
STAMPEDE is a randomly, open label, multi-arm, multistage controlled trial including locally
advanced or metastatic prostate cancer patients who initiated for the first time ADT [31]. The
Information Classification: General
primary aim of this multi-arm trial was to test the benefit of the addition of further treatment with
ADT to improve OS. Concerning the abiraterone acetate study in CSPC patients, 1917 patients were
randomized, including newly diagnosed high-risk patients with at least two of the three high-risk
factors (T3-T4 stage, PSA ≥40 ng/mL, Gleason grade ≥ 8), nodal disease, metastatic prostate cancer
and previously treated relapsing patients (surgery or radiotherapy with <12 months of hormone
therapy) with at least one of the four high-risk factors (PSA ≥4 ng/mL and increasing with a doubling
T
IP
time of <6 months; PSA ≥20 ng/mL; nodal invasion or, metastatic disease). Local radiotherapy was
mandated for patients with node-negative, nonmetastatic disease and encouraged for those with
R
positive nodes. A total of 95% of patients had newly diagnosed disease and 52% had metastatic
SC
disease.
With a median follow up of 40 months, there was an overall survival advantage for the AA + ADT
U
AN
group compared with ADT alone, with a hazard ratio of 0.63 (0.75 in patients with nonmetastatic
disease and 0.61 in those with metastatic disease).
M
The benefit was the same for the intermediate primary outcome and failure-free survival (including
death and progression) where there were less treatment failure events in the AA group compared
D
with those reported in the ADT alone group (hazard ratio 0.29). The latter included patients from the
TE
whole cohort in both metastatic and nonmetastatic subgroups [32]. However, differences were more
EP
important in the metastatic subgroup.
Important differences of patient selection have to be highlighted between STAMPEDE and LATITUDE
C
trials. The LATITUDE trial only included de novo, metastatic CSPC patients who exhibited high-risk
AC
cancer, as defined by Gleason score, site and number of metastases. The STAMPEDE trial was
dedicated to every patient candidate for ADT, including those with high-risk but nonmetastatic
cancer and those with low-risk mCSPC. Sub-group analyses in the STAMPEDE trial tended to support
the benefit of AA, even in the non-LATITUDE-like patients [33]. These main studies are summarized in
Table 1.
Information Classification: General
8. CURRENT RECOMMENDATIONS
With strong evidence, national and international guidelines currently recommend AA plus
prednisone as treatment options for mCRPC and mCSPC patients.
The European EAU-ESTRO-SIOG guidelines [34] recommend AA plus prednisone with castration for
the first line treatment of metastatic prostate cancer to all patients whose first presentation is M1
T
IP
disease and who are fit enough to receive this treatment (Level A). For mCRPC, AA can be offered as
first and second line treatments. Physician’s choices should be based on performance status,
R
symptoms, comorbidities, location, extent of disease, patient preference and previous treatment.
SC
French national committee guidelines [35] recommend that with grade A, a combination of evidence
level AA, prednisone and castration be used as first line treatment of metastatic prostate cancer,
U
AN
especially in high risk populations. For first line mCRPC, no predictive factors have been identified to
recommend second generation hormonotherapy rather than taxanes. With a grade B level of
M
evidence, second generation hormonotherapy is recommended for asymptomatic or mildly
symptomatic patients without visceral metastasis.
D
American urological association (AUA) guidelines [36] extended the AA recommendation (grade C) to
TE
non-metastatic CRPC patients at high risk of developing metastatic disease who do not want, or
EP
cannot have one of the standard therapies (enzalutamide or apalutamide) and are unwilling to
accept surveillance. This recommendation based on superior survival benefits was shown in
C
metastatic CRPC and metastatic high-risk castration-sensitive prostate cancer but is not FDA-
AC
approved for non-metastatic patients due to a lack of significant long-term data in this specific
population.
In first line mCRPC treatment, AA is recommended for asymptomatic or mildly symptomatic mCRPC
(grade A), symptomatic with good performance status (grade A) and with grade C for poor
performance status. After docetaxel, AA can be used for patients with good performance status
Information Classification: General
(grade A). Expert opinion presents AA as an alternative for selected patients with poor performance
status who are not eligible for supportive care only.
Thus, consensus has been reached between different guidelines regarding the use of AA plus
prednisone in metastatic prostate, with strongest evidences pointing to asymptomatic or mildly
symptomatic mCRPC and high-risk mCSPC.
T
IP
R
SC
U
AN
M
D
TE
EP
C
AC
Information Classification: General
9. RESISTANCE MECHANISMS
The natural evolution of the metastatic prostate cancer is often marked by an initial response phase
to abiraterone followed by relapsed disease progression in long term patients and ultimately results
in a disease non-responsive to abiraterone. However, some CRPC patients exhibit primary resistance
where commencement of AA treatment is not associated with decreasing PSA, other clinical and/or
T
IP
imaging progression. This phenomenon was reported in less than 10% of chemotherapy naïve
patients with mCRPC [27] and less than 40% of patients with mCRPC after chemotherapy [8]. As
R
resistance mechanisms to CYP17A1 inhibitor are still poorly understood, AR activity appears to be
SC
restored. Animal models, tumor biopsy mRNA or liquid biopsy of patients who had developed
resistance to CYP17A1 inhibitor were studied. A few mechanisms were suspected; progesterone
U
AN
driven mutation, AR mutation, amplification, AR enhancer mutations, AR splice variants [37], AR
activation by exogenous corticosteroids and steroids precursors upstream of CYP17A1, androgen
M
biosynthesis pathway upregulation, glucocorticoids and glucocorticoid receptor overexpression [3].
Mutations in the binding domain of the AR ligand might be one of these mechanisms, resulting in
D
permanent activation of the AR without the ligand [38]. One of the most important examples of AR
TE
permanent activation is the AR splice variant 7 (AR-V7) which is prevalent in CRPC. This splice variant
EP
is the result of an abnormal splicing of intronic sequences and encodes a truncated AR protein
[39,40]. The latter has a transactivating domain and lacks a ligand binding domain. So, the AR is
C
unable to bind ligand and is permanently activated. Amplification of this variant is one cause for the
AC
abiraterone escape mechanism. AR-V7 messenger RNA can be detected reliably from circulating
tumor cells (CTC) and different methods can be used to detect AR-V7. A clinical study showed, upon
performing a RT PCR for mRNA detection of this splice variant in CTC, that AR-V7 was associated with
resistance to abiraterone and enzalutamide. AR-V7 positive patients had no, or less PSA responses
and no any appreciable clinical benefits [41,42]. However, this AR splice variant does not explain all
Information Classification: General
of the mechanisms of resistance as patients negative for AR-V7 did not respond to abiraterone and
enzalutamide [43].
T
IP
R
SC
U
AN
M
D
TE
EP
C
AC
Information Classification: General
10. ONGOING STUDIES
Numerous studies are ongoing to keep on evaluating efficacy, safety, and tolerability of AA, alone or
in combination, in special populations.
Other studies have been designed to explore biomarkers predictive for abiraterone response. In
addition, combinations with chemotherapy, olaparib (PROpel trial), radiotherapy (ARTO trial),
T
IP
different sequences and re-challenge are being tested for metastatic prostate cancer.
Studies are underway to extend the indication to advanced non-metastatic prostate diseases
R
including a prospective, multicenter, phase II trial in men with non-metastatic, castration-resistant
SC
prostate cancer (IMAAGEN trial), or neo-adjuvant use for patients diagnosed with localized high-risk
prostate cancer prior to radical prostatectomy or radiotherapy.
U
AN
Given the availability of other drugs targeting the androgen-receptor pathways such as
enzalutamide, apalutamide, and darolutamide, the debate concerning the ideal sequence and the
M
potential usefulness of combination therapies remains. Few studies are currently available exploring
these two questions. The phase II PLATO study has evaluated the interest of combining abiraterone
D
acetate with enzalutamide as mCRPC second-line hormonal therapy in patients experiencing
TE
progression after enzalutamide as first-line treatment [44]. The same study showed that switching
EP
enzalutamide with abiraterone did not produce a significant difference in disease control. No benefit
was provided by combining new generation therapy.
C
Another combination trial is ongoing, the ACIS trial, assessing the potential benefit of the association
AC
apalutamide plus abiraterone (compared with abiraterone acetate alone) in terms of rPFS in
chemonaive mCRPC patients. Results are pending and expected in 2021.
The difference of efficacy between abiraterone acetate then enzalutamide versus enzalutamide then
abiraterone has been assessed in a phase II trial in mCRPC patients (Khalaf, Lancet Oncol 2019).
Findings tended to support the use of abiraterone acetate for first line treatment, as the second PSA
Information Classification: General
progression was reached after a greater delay for the sequence of abiraterone followed by
enzalutamide than with the opposite treatment sequence.
Different approaches attempting to delay acquired resistance to AA are also being studied including
combination therapies and ideal sequences, but a potential strategy after resistance would be to
supplement patients with testosterone (RESTORE study).
T
IP
Main studies used Zytiga ©, but generic versions of AA have been approved by the FDA after
bioequivalence demonstration [45] and Zytiga’s exclusivity expires on February, 2021.
R
SC
Other conditions could be targeted. This is the case in preliminary studies regarding the management
of Cushing's syndrome in patients with adrenocortical Carcinoma (ABACUS), the molecular apocrine
U
AN
breast cancer (AMA) treatment and the androgen reduction in congenital adrenal hyperplasia.
M
D
TE
EP
C
AC
Information Classification: General
11. CONCLUSION
AA is a second-generation hormone treatment which is a standard molecular entity for blocking
androgen receptor expression, acting as a selective and irreversible CYP17A1 inhibitor. AA inhibits
the conversion of cholesterol to an androgen precursor and steroid hormone synthesis in
steroidogenic tissue. Its mechanism of action explains the decrease in cortisol levels and the
T
IP
necessity of concomitant prednisone supplementation to reduce adverse effects. AA presents a good
safety profile with the main serious side effects including hepatotoxicity and cardiotoxicity, requiring
R
close monitoring upon treatment initiation.
SC
Several large-scale phase III trials showed significant overall survival benefits in mCRPC and mCSPC
patients leading to a recent change in prostate cancer treatment recommendations. Future studies
U
AN
should focus on the identification of predictive biomarkers of disease response and early resistance,
at late stages with the potential for combination therapy.
M
D
TE
EP
C
AC
Information Classification: General
12. EXPERT OPINION
Prostate cancer remains an important life-threatening public health issue given its prevalence and its
related mortality. At a metastatic stage, disease is not curable and androgen suppression has proven,
for decades, its importance in the castration sensitivity of prostate cancer. Androgen suppression by
orchiectomy or first-generation hormone treatments (LHRH agonists and antagonists, anti-
T
IP
androgens) was the only treatment at both CRPC and CSPC until the beginning of our century. This
means that no survival benefit has been gained and no convincing research has been confirmed in
R
patients for years. Nevertheless, the last 15 years of research including the first docetaxel studies,
SC
taxane-specific chemotherapy and new generation hormone therapies have shown life prolongation
in mCRPC and at earlier stages of mCSPC. Abiraterone acetate has been the first new generation
U
AN
hormone therapy to be approved in post-chemotherapy mCRPC stage, then in pre-chemotherapy
stage, and finally in mCSPC disease. It has strongly participated in the improvement of metastatic
M
prostate cancer prognosis.
When lowering the extracellular level of testosterone by castration becomes insufficient, AA
D
demonstrates that the tumor cell is still sensitive to steroid derivates and that the androgen receptor
TE
still drives important intracellular pathways, guiding tumor growth and progression.
EP
Oral route treatment may be efficient even after docetaxel failure, and well tolerated. This hormone
therapy has to date a strong impact within a real-world setting and is realistically implemented into
C
clinical practice with the inclusion of AA in international guidelines.
AC
Studies at the mCSPC show that the earlier, the better. In high-risk metastatic prostate cancer, the
early initiation of AA improves overall survival, as well as the time to progression after subsequent
therapy lines. The intensification of hormonal treatment since the diagnosis of metastases will
undoubtedly become the standard of care in upcoming months and beyond. Androgen deprivation
alone will take a step back and become an option only in unfit and older patients with a short life
expectancy.
Information Classification: General
Cancer treatment decision-making is mainly based on survival benefits. Given the large panel of
available life-prolonging agents, future studies should also focus on quality-of-life and patient-
reported outcomes. AA has proven to improve or at least not to alter quality-of-life of patients, even
at early mCSPC when disease-related symptoms are not frequent. Post-approval and phase IV studies
could be clinically relevant to guide treatment choice between two, three, or four new generation
hormone therapies. This choice should also be shared with patient (short-term IV chemotherapy
T
IP
versus long-term oral route hormone treatment?) who can be actively involved in treatment
decision-making given the safety profile of each drug and the patient comorbidities.
R
Several questions remain open to debate. Is there a place for combination therapy? In other words,
SC
the stronger, the better? Some studies are ongoing but preliminary findings do not strongly support
this hypothesis for combined new generation hormone treatments.
U
AN
The sequential use of new drugs has improved the overall survival of patients with metastatic
prostate cancer. However, few studies, mainly retrospective, have assessed the impact of the order
M
of administration.
The ideal sequence at an individual basis remains poorly known. Recent studies have suggested that
D
the sequential use of drugs with different mechanisms of action improved the cumulative survival
TE
and have supported the high risk of cross-resistance between the two new generation hormone
EP
therapies [46]. The place of AA and other intensification strategies in recurrent, low-volume
metastatic prostate cancer remains debatable. Metastasis-directed therapy by stereotactic body
C
radiotherapy or surgery could play a role by postponing the initiation of systemic treatment and
AC
could challenge intensified combination treatment in that setting.
Last, but not least, the quest for the ideal biomarker, capable to predict prognosis (prognostic
biomarker) or AA treatment response (theranostic biomarker), remains open. Several targets have
been suggested such as AR slice variants or multiple gene signature, none of which are currently used
in routine practice. Research efforts in this field are tremendous. And for that purpose, a simple
Information Classification: General
blood test, able to quantify tumor burden and to characterize mutations spectrum, could be more
efficient than tumor biopsy on primary or metastatic sites.
T
IP
R
SC
U
AN
M
D
TE
EP
C
AC
Information Classification: General
Funding
This paper received no funding.
Declaration of interest
G Ploussard, L Mourey and D Pouessel have received congress invitations, and have served as
consultants and on the advisory board for Janssen. The authors have no other relevant
affiliations or financial involvement with any organization or entity with a financial interest in or
financial conflict with the subject matter or materials discussed in the manuscript apart from
T
those disclosed.
IP
Reviewer disclosures
R
A reviewer on this paper has conducted research and/or served as a consultant for; Astellas,
Bayer, Janssen, Pfizer, and Sanofi-Genzyme. Peer reviewers on this manuscript have no other
SC
relevant financial relationships or otherwise to disclose.
Acknowledgement
U
The authors would like to thank Charlotte Somes for English editing of the manuscript.
AN
M
D
TE
EP
C
AC
Information Classification: General
References
Papers of special note have been highlighted as either of interest (*) or of considerable interest
(**) to readers.
[1] Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide:
Sources, methods and major patterns in GLOBOCAN 2012 - Ferlay - 2015 - International Journal of
Cancer - Wiley Online Library [Internet]. [cited 2019 Jul 6]. Available from:
https://onlinelibrary.wiley.com/doi/epdf/10.1002/ijc.29210.
[2] Huggins C, Hodges CV. Studies on Prostatic Cancer: I. The Effect of Castration, Of Estrogen
T
and of Androgen Injection on Serum Phosphatases in Metastatic Carcinoma of the Prostate. CA: A
IP
Cancer Journal for Clinicians. 1972;22:232–240.
[3] Buttigliero C, Tucci M, Bertaglia V, et al. Understanding and overcoming the mechanisms of
primary and acquired resistance to abiraterone and enzalutamide in castration resistant prostate
R
cancer. Cancer Treatment Reviews. 2015;41:884–892.
[4] Cai C, Balk SP. Intratumoral androgen biosynthesis in prostate cancer pathogenesis and
SC
response to therapy. Endocrine-Related Cancer. 2011;18:R175–R182.
[5] Chaturvedi AP, Dehm SM. Androgen Receptor Dependence. In: Dehm SM, Tindall DJ, editors.
Prostate Cancer: Cellular and Genetic Mechanisms of Disease Development and Progression
[Internet]. Cham: Springer International Publishing; 2019 [cited 2020 Jan 10]. p. 333–350. Available
U
from: https://doi.org/10.1007/978-3-030-32656-2_15.
AN
[6] Auchus RJ, Yu MK, Nguyen S, et al. Use of Prednisone With Abiraterone Acetate in Metastatic
Castration-Resistant Prostate Cancer. The Oncologist. 2014;19:1231–1240.
[7] DeVore NM, Scott EE. Structures of cytochrome P450 17A1 with prostate cancer drugs
abiraterone and TOK-001. Nature. 2012;482:116–119.
M
[8] de Bono JS, North S, Saad F, et al. Abiraterone and Increased Survival in Metastatic Prostate
Cancer. n engl j med. 2011;11.
[9] Fizazi K, Tran N, Fein L, et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive
D
Prostate Cancer. New England Journal of Medicine. 2017;377:352–360.
[10] James ND, de Bono JS, Spears MR, et al. Abiraterone for Prostate Cancer Not Previously
TE
Treated with Hormone Therapy. New England Journal of Medicine. 2017;377:338–351.
[11] * Fizazi K, Scher HI, Molina A, et al. Abiraterone acetate for treatment of metastatic
castration-resistant prostate cancer: final overall survival analysis of the COU-AA-301 randomised,
EP
double-blind, placebo-controlled phase 3 study. The Lancet Oncology. 2012;13:983–992.
These four references present the main phase III studies showing abiraterone acetate efficacity and
toxicity for metastatic prostate cancer.
C
AC
[12] Attard G, Reid AHM, Auchus RJ, et al. Clinical and Biochemical Consequences of CYP17A1
Inhibition with Abiraterone Given with and without Exogenous Glucocorticoids in Castrate Men with
Advanced Prostate Cancer. The Journal of Clinical Endocrinology & Metabolism. 2012;97:507–516.
[13] Baloch HM, Grice-Patil ZJ, Selig DJ, et al. Recognition and Treatment of Adrenal Insufficiency
Secondary to Abiraterone: A Case Report and Literature Review. Oncology. 2019;97:301–305.
[14] Iacovelli R, Ciccarese C, Bria E, et al. The Cardiovascular Toxicity of Abiraterone and
Enzalutamide in Prostate Cancer. Clinical Genitourinary Cancer. 2018;16:e645–e653.
[15] Fizazi K, Chi KN, de Bono JS, et al. Low Incidence of Corticosteroid-associated Adverse Events
on Long-term Exposure to Low-dose Prednisone Given with Abiraterone Acetate to Patients with
Metastatic Castration-resistant Prostate Cancer. European Urology. 2016;70:438–444.
[16] Mulders PFA, Molina A, Marberger M, et al. Efficacy and Safety of Abiraterone Acetate in an
Elderly Patient Subgroup (Aged 75 and Older) with Metastatic Castration-resistant Prostate Cancer
Information Classification: General
After Docetaxel-based Chemotherapy. European Urology. 2014;65:875–883.
[17] Smith MR, Rathkopf DE, Mulders PFA, et al. Efficacy and Safety of Abiraterone Acetate in
Elderly (75 Years or Older) Chemotherapy Naïve Patients with Metastatic Castration Resistant
Prostate Cancer. Journal of Urology. 2015;194:1277–1284.
[18] Thiery-Vuillemin A, Poulsen MH, Lagneau E, et al. Impact of Abiraterone Acetate plus
Prednisone or Enzalutamide on Patient-reported Outcomes in Patients with Metastatic Castration-
resistant Prostate Cancer: Final 12-mo Analysis from the Observational AQUARiUS Study. European
Urology. 2020;77:380–387.
[19] Del Re M, Fogli S, Derosa L, et al. The role of drug-drug interactions in prostate cancer
treatment: Focus on abiraterone acetate/prednisone and enzalutamide. Cancer Treatment Reviews.
2017;55:71–82.
T
[20] Chi KN, Protheroe A, Rodríguez-Antolín A, et al. Patient-reported outcomes following
IP
abiraterone acetate plus prednisone added to androgen deprivation therapy in patients with newly
diagnosed metastatic castration-naive prostate cancer (LATITUDE): an international, randomised
phase 3 trial. The Lancet Oncology. 2018;19:194–206.
R
[21] Monbaliu J, Gonzalez M, Bernard A, et al. In Vitro and In Vivo Drug-Drug Interaction Studies
to Assess the Effect of Abiraterone Acetate, Abiraterone, and Metabolites of Abiraterone on CYP2C8
SC
Activity. Drug Metabolism and Disposition. 2016;44:1682–1691.
[22] Bernard A, Vaccaro N, Acharya M, et al. Impact on abiraterone pharmacokinetics and safety:
Open-label drug-drug interaction studies with ketoconazole and rifampicin: Clinical Pharmacology in
Drug Development. Clinical Pharmacology in Drug Development. 2015;4:63–73.
[23]
U
Goodman OB, Flaig TW, Molina A, et al. Exploratory analysis of the visceral disease subgroup
AN
in a phase III study of abiraterone acetate in metastatic castration-resistant prostate cancer. Prostate
Cancer and Prostatic Diseases. 2014;17:34–39.
[24] Sternberg CN, Molina A, North S, et al. Effect of abiraterone acetate on fatigue in patients
with metastatic castration-resistant prostate cancer after docetaxel chemotherapy. Annals of
M
Oncology. 2013;24:1017–1025.
[25] Harland S, Staffurth J, Molina A, et al. Effect of abiraterone acetate treatment on the quality
of life of patients with metastatic castration-resistant prostate cancer after failure of docetaxel
D
chemotherapy. European Journal of Cancer. 2013;49:3648–3657.
[26] Logothetis CJ, Basch E, Molina A, et al. Effect of abiraterone acetate and prednisone
TE
compared with placebo and prednisone on pain control and skeletal-related events in patients with
metastatic castration-resistant prostate cancer: exploratory analysis of data from the COU-AA-301
randomised trial. The Lancet Oncology. 2012;13:1210–1217.
EP
[27] * Ryan CJ, Smith MR, Fizazi K, et al. Abiraterone acetate plus prednisone versus placebo plus
prednisone in chemotherapy-naive men with metastatic castration-resistant prostate cancer (COU-
AA-302): final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3
study. The Lancet Oncology. 2015;16:152–160.
C
These four references present the main phase III studies showing abiraterone acetate efficacity and
AC
toxicity for metastatic prostate cancer.
[28] Ryan CJ, Smith MR, de Bono JS, et al. Abiraterone in Metastatic Prostate Cancer without
Previous Chemotherapy. New England Journal of Medicine. 2013;368:138–148.
[29] Rathkopf DE, Smith MR, de Bono JS, et al. Updated Interim Efficacy Analysis and Long-term
Safety of Abiraterone Acetate in Metastatic Castration-resistant Prostate Cancer Patients Without
Prior Chemotherapy (COU-AA-302). European Urology. 2014;66:815–825.
[30] * Fizazi K, Tran N, Fein L, et al. Abiraterone acetate plus prednisone in patients with newly
diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): final overall survival
analysis of a randomised, double-blind, phase 3 trial. The Lancet Oncology. 2019;20:686–700.
These four references present the main phase III studies showing abiraterone acetate efficacity and
Information Classification: General
toxicity for metastatic prostate cancer.
[31] James ND, Sydes MR, Clarke NW, et al. Systemic therapy for advancing or metastatic prostate
cancer (STAMPEDE): a multi-arm, multistage randomized controlled trial. BJU International.
2009;103:464–469.
[32] Hoyle AP, Ali SA, James ND, et al. LBA4Effects of abiraterone acetate plus
prednisone/prednisolone in high and low risk metastatic hormone sensitive prostate cancer. Annals
of Oncology [Internet]. 2018 [cited 2020 Jan 10];29. Available from:
https://academic.oup.com/annonc/article/doi/10.1093/annonc/mdy424.033/5141727.
[33] * Hoyle AP, Ali A, James ND, et al. Abiraterone in “High-” and “Low-risk” Metastatic
T
Hormone-sensitive Prostate Cancer. European Urology. 2019;76:719–728.
IP
These four references present the main phase III studies showing abiraterone acetate efficacity and
toxicity for metastatic prostate cancer.
R
SC
[34] Cornford P, Bellmunt J, Bolla M, et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part II:
Treatment of Relapsing, Metastatic, and Castration-Resistant Prostate Cancer. European Urology.
2017;71:630–642.
[35] Rozet F, Hennequin C, Beauval J-B, et al. Recommandations françaises du Comité de
U
Cancérologie de l’AFU – Actualisation 2018–2020 : cancer de la prostate. Progrès en Urologie.
AN
2018;28:S79–S130.
[36] Lowrance WT, Murad MH, Oh WK, et al. Castration-Resistant Prostate Cancer: AUA Guideline
Amendment 2018. Journal of Urology. 2018;200:1264–1272.
[37] Liu C, Yang JC, Armstrong CM. AKR1C3 Promotes AR-V7 Protein Stabilization and Confers
M
Resistance to AR-Targeted Therapies in Advanced Prostate Cancer | Molecular Cancer Therapeutics.
2019 [cited 2020 Feb 1];18. Available from: https://mct.aacrjournals.org/content/18/10/1875.long.
[38] Han D, Gao S, Valencia K, et al. A novel nonsense mutation in androgen receptor confers
D
resistance to CYP17 inhibitor treatment in prostate cancer. Oncotarget [Internet]. 2017 [cited 2020
Jan 31];8. Available from: http://www.oncotarget.com/fulltext/14296.
TE
[39] Dehm SM, Schmidt LJ, Heemers HV, et al. Splicing of a Novel Androgen Receptor Exon
Generates a Constitutively Active Androgen Receptor that Mediates Prostate Cancer Therapy
Resistance. Cancer Research. 2008;68:5469–5477.
EP
[40] Hu R, Dunn TA, Wei S, et al. Ligand-Independent Androgen Receptor Variants Derived from
Splicing of Cryptic Exons Signify Hormone-Refractory Prostate Cancer. Cancer Research. 2009;69:16–
22.
[41] Antonarakis ES, Lu C, Wang H, et al. AR-V7 and Resistance to Enzalutamide and Abiraterone
C
in Prostate Cancer. New England Journal of Medicine. 2014;371:1028–1038.
[42] Antonarakis ES, Lu C, Luber B, et al. Clinical Significance of Androgen Receptor Splice Variant-
AC
7 mRNA Detection in Circulating Tumor Cells of Men With Metastatic Castration-Resistant Prostate
Cancer Treated With First- and Second-Line Abiraterone and Enzalutamide. Journal of Clinical
Oncology. 2017;35:2149–2156.
[43] Cattrini C, Rubagotti A, Zinoli L, et al. Role of Circulating Tumor Cells (CTC), Androgen
Receptor Full Length (AR-FL) and Androgen Receptor Splice Variant 7 (AR-V7) in a Prospective Cohort
of Castration-Resistant Metastatic Prostate Cancer Patients. Cancers. 2019;11:1365.
[44] Attard G, Borre M, Gurney H, et al. Abiraterone Alone or in Combination With Enzalutamide
in Metastatic Castration-Resistant Prostate Cancer With Rising Prostate-Specific Antigen During
Enzalutamide Treatment. Journal of Clinical Oncology. 2018;36:2639–2646.
[45] Wang C, Hu C, Gao D, et al. Pharmacokinetics and bioequivalence of generic and branded
abiraterone acetate tablet: a single-dose, open-label, and replicate designed study in healthy Chinese
male volunteers. Cancer Chemotherapy and Pharmacology. 2019;83:509–517.
Information Classification: General
[46] Caffo O, Wissing M, Bianchini D, et al. Survival Outcomes From a Cumulative Analysis of
Worldwide Observational Studies on Sequential Use of New Agents in Metastatic Castration-
Resistant Prostate Cancer. Clinical Genitourinary Cancer. 2020;18:69-76.e4.
T
IP
R
SC
U
AN
M
D
TE
EP
C
AC
Information Classification: General
mCRPC mCSPC
Study COU-AA-301 COU-AA-302 LATITUDE
ra
Design randomly, double-blind randomly, double-blind randomly, double-blind a
Treatment arm AA + ADT + prednisone AA + ADT + prednisone AA + ADT+ prednisone
T
Control arm ADT + prednisone + placebo ADT + prednisone + placebo ADT + dual placebo
Randomization 2:1 1:1 1:1
IP
Enrollment number 1 195 1088 1 199
Metastatic? 100% 100% 100% de novo
R
5% liver
Visceral metastasis 29% 0%
SC
12% lung
Only High risk patients No No Yes
Previous treatment for
Allowed Allowed No
localized PCa
Prior ADT? Yes
U Yes ≤ 3 months
AN
Previous docetaxel? 100% 0% 0%
PS > 1 10% 0%
Median PSA 128.8 42 23.85
M
Follow-up (months) 20.2 49.2 51.8
OS : 0,66 (0,56-0,78)
OS: 0.74 ( 0.64–0.86) 53,3 vs 36,5
D
Primary endpoint HR (IC) OS: 0.81 (0.70–0.93)
5.8 vs 11.2 rPFS : 0,47 (0,39-0,55)
Duration (months) 34,7 vs 30,3
TE
33,0 vs 14,8
Study arm duration treatment
13.8 24 21.8
EP
median (months)
Table 1: Main Abiraterone Acetate Phase III studies. ADT: Androgen deprivation therapy; CI: confidence interval ;
C
mCSPC: metastatic castration-sensitive prostate cancer ;mCRPC: metastatic castration resistant prostate cancer; OS: overall
survival; PCa: prostate cancer; PSA: prostate specific antigen ; rPFS: radiologic progression free survival ; HR: hazard ratio
AC
Information Classification: General
T
IP
R
SC
Fig 1 : CYP17A1, 17 α-hydro
metaboliism
oxylase/C17,,20 lyase activity
a
U
in pregnenolone
p e and prog
gesterone
AN
Legend: 17 α-hydroxylase
e converts preg
gnenolone and p
progesterone to
o 17-hydroxypre
egnenolone andd 17-hydroxypro
ogesterone.
C17,20 Lyyase convert 17--hydroxypregnenolone to dehyd
droepiandrosterrone.
M
Pregnenollone and progessterone can be treated
t to form m
mineralocortico
oids.
17-hydroxyypregnenolone and 17-hydroxy
yprogesterone ccan be treated for
fo the generatio
on of glucocorticcoid such as corrtisol.
17-hydroxyyprogesterone can
c be treated for
f the generatio
on of testosterone.
D
Abirateron
ne is an irreversiible 17 α-hydrox
xylase/C17,20 ly
lyase inhibitor and
a decreases glucocorticoid
g annd testosterone
e production
and increa
ases mineraloco
orticoids producttion.
TE
EP
C
AC
Informattion Classifica
ation: Genera
al
You might also like
- Astm A370 2020Document50 pagesAstm A370 2020امين100% (1)
- Quarter 3 - Module 1-W1&W2: Computer Systems Servicing (CSS)Document18 pagesQuarter 3 - Module 1-W1&W2: Computer Systems Servicing (CSS)AC Balio100% (5)
- Second-Generation Antiandrogens: From Discovery To Standard of Care in Castration Resistant Prostate CancerDocument12 pagesSecond-Generation Antiandrogens: From Discovery To Standard of Care in Castration Resistant Prostate CancernadalNo ratings yet
- Advanced Prostate Cancer: Treatment Advances and Future DirectionsDocument14 pagesAdvanced Prostate Cancer: Treatment Advances and Future DirectionsMishel Rodriguez GuzmanNo ratings yet
- J Eururo 2020 09 046Document20 pagesJ Eururo 2020 09 046Ivor Wiguna Hartanto WilopoNo ratings yet
- Nanomedicinal Strategies To Treat Multidrug-Resistant Tumors: Current ProgressDocument19 pagesNanomedicinal Strategies To Treat Multidrug-Resistant Tumors: Current ProgressCarolina CamerinNo ratings yet
- 1-Abiraterone and Spironolactone in Prostate Cancer - A Combination To AvoidDocument7 pages1-Abiraterone and Spironolactone in Prostate Cancer - A Combination To Avoidonco learnNo ratings yet
- 7992 FullDocument12 pages7992 FullHector Javier BurgosNo ratings yet
- Enzalutamida arches-JCO.19.00799Document15 pagesEnzalutamida arches-JCO.19.00799Raul BarcellonaNo ratings yet
- Jco 19 00799Document15 pagesJco 19 00799Residentes urologiaNo ratings yet
- Cisplatin-Based Chemoradiation Plus Cetuximab in Head and Neck Cancer Ann Oncol-2010-Merlano-annonc - mdq412Document6 pagesCisplatin-Based Chemoradiation Plus Cetuximab in Head and Neck Cancer Ann Oncol-2010-Merlano-annonc - mdq412ZuriNo ratings yet
- Update On Radiotherapy in Gynaecological Malignancies: ReviewDocument8 pagesUpdate On Radiotherapy in Gynaecological Malignancies: ReviewDesrha TangdiseruNo ratings yet
- An Updated Analysis of The Survival Endpoints of Ascende-Rt: Clinical InvestigationDocument10 pagesAn Updated Analysis of The Survival Endpoints of Ascende-Rt: Clinical InvestigationfumadelabuenaNo ratings yet
- Reirradiation For Head and NeckDocument8 pagesReirradiation For Head and NeckAlvaro Rodrigo Oporto CauzlarichNo ratings yet
- Results of Proton ReirradiationDocument9 pagesResults of Proton ReirradiationJesse Helmut Hansen-BartelNo ratings yet
- Intensity-Modulated Radiation Therapy (Imrt) in The Treatment of Anal Cancer - Toxicity and Clinical OutcomeDocument8 pagesIntensity-Modulated Radiation Therapy (Imrt) in The Treatment of Anal Cancer - Toxicity and Clinical OutcomejunfangokuNo ratings yet
- Retinol 2Document12 pagesRetinol 2Tiên PhạmNo ratings yet
- 1 s2.0 S0167814022044991 MainDocument9 pages1 s2.0 S0167814022044991 MainFeras OskanNo ratings yet
- Towards Personalized Treatment For Prostate CancerDocument202 pagesTowards Personalized Treatment For Prostate CancerEduar Antonio Landazuri IdroboNo ratings yet
- Fonc 07 00177Document13 pagesFonc 07 00177Ihenanacho HappinessNo ratings yet
- Landmark Trials Genitourinary CompilationDocument55 pagesLandmark Trials Genitourinary CompilationBhanuNo ratings yet
- The Addition of Pelvic Lymph Node Treatment To Pro - 9Document2 pagesThe Addition of Pelvic Lymph Node Treatment To Pro - 9gascarteziniNo ratings yet
- Aro 96-02auo Ap 0995Document8 pagesAro 96-02auo Ap 0995yingming zhuNo ratings yet
- Jco 20 03282Document10 pagesJco 20 03282AKNo ratings yet
- 660ijrobp2011y90 Model-Based Radiation Dose Correction For Yttrium-90 Microsphere Treatment of Liver Tumors With Central Necrosis - CsliuDocument9 pages660ijrobp2011y90 Model-Based Radiation Dose Correction For Yttrium-90 Microsphere Treatment of Liver Tumors With Central Necrosis - Csliu劉晉昇No ratings yet
- Radiotherapy and Oncology: Original ArticleDocument10 pagesRadiotherapy and Oncology: Original ArticleAKNo ratings yet
- Use of Androgen Deprivation Therapy (ADT) and Radiotherapy in Post-Operative Prostate Cancer PatientsDocument2 pagesUse of Androgen Deprivation Therapy (ADT) and Radiotherapy in Post-Operative Prostate Cancer PatientsDr Rajiv DahiyaNo ratings yet
- Biblio 13Document6 pagesBiblio 13ManganusNo ratings yet
- Swog 8794Document7 pagesSwog 8794yingming zhuNo ratings yet
- Pi Is 2405456923001992Document6 pagesPi Is 2405456923001992Joy IsmailNo ratings yet
- Cancers 15 02552Document17 pagesCancers 15 02552NIrmalya SenguptaNo ratings yet
- Nuhn 2018Document12 pagesNuhn 2018Evelynππ θσυNo ratings yet
- Lenvatinib in Thyroid CancerDocument9 pagesLenvatinib in Thyroid Cancerstepanus massoraNo ratings yet
- H.E. Sartori - Nutrients and Cancer - An Introduction To Cesium TherapyDocument4 pagesH.E. Sartori - Nutrients and Cancer - An Introduction To Cesium TherapywxcvbnnbvcxwNo ratings yet
- Proton Beam Therapy For Prostate Cancer An OverviewDocument3 pagesProton Beam Therapy For Prostate Cancer An OverviewEditor IJTSRDNo ratings yet
- 1 s2.0 S1051044322011903 MainDocument30 pages1 s2.0 S1051044322011903 MainEsmaeel Jafargholi RangrazNo ratings yet
- EBRT in DTCDocument7 pagesEBRT in DTCElena FlorentinaNo ratings yet
- Ournal of Linical Ncology: PurposeDocument7 pagesOurnal of Linical Ncology: PurposeNelson William UsnayoNo ratings yet
- Lectura 2Document10 pagesLectura 2Ricardo Huaman QuirozNo ratings yet
- Article LCA ConfCycle2 1617fevrier2023Document9 pagesArticle LCA ConfCycle2 1617fevrier2023parasite myNo ratings yet
- Hepatectomy Versus Stereotactic Body Radiotherapy For Primary Early Hepatocellular Carcinoma A Propensity-Matched Analysis in A Single InstitutionDocument8 pagesHepatectomy Versus Stereotactic Body Radiotherapy For Primary Early Hepatocellular Carcinoma A Propensity-Matched Analysis in A Single Institutiondongjun daiNo ratings yet
- Accepted Manuscript: Seminars in Colon & Rectal SurgeryDocument21 pagesAccepted Manuscript: Seminars in Colon & Rectal Surgerynaylul farohahNo ratings yet
- Mrna Vaccine cv9103 and cv9104 For The Treatment of Prostate CancerDocument8 pagesMrna Vaccine cv9103 and cv9104 For The Treatment of Prostate Cancerapi-675909478No ratings yet
- Recent Advances With Topotecan in The Treatment of Lung CancerDocument13 pagesRecent Advances With Topotecan in The Treatment of Lung Cancerapi-3821924No ratings yet
- Fimmu 11 577869Document18 pagesFimmu 11 577869nataliaNo ratings yet
- TouijerDocument7 pagesTouijerVinko GrubišićNo ratings yet
- BJR 20180494Document14 pagesBJR 20180494Gonzalo NunezNo ratings yet
- 1 s2.0 S1470204520306665 MainDocument11 pages1 s2.0 S1470204520306665 MainshangrilaNo ratings yet
- YUAN Et Al., 2020Document11 pagesYUAN Et Al., 2020Thaís MesequeNo ratings yet
- A Systematic Review and Meta Analysis 1625134013Document13 pagesA Systematic Review and Meta Analysis 1625134013bannour_No ratings yet
- Arsene Henry2017Document2 pagesArsene Henry2017Gabriela Silva MartinsNo ratings yet
- Jurnal OnkologiDocument9 pagesJurnal OnkologiIrham HasbiNo ratings yet
- RT Versus Carbo 2011Document6 pagesRT Versus Carbo 2011Bruno AlanNo ratings yet
- Down-Staging of Early Stage Prostate Can PDFDocument9 pagesDown-Staging of Early Stage Prostate Can PDFNelma TuiranNo ratings yet
- 2020 POUT Adj Pt+Gem in UrothelialDocument10 pages2020 POUT Adj Pt+Gem in UrothelialFilip IonescuNo ratings yet
- Brachytherapy Boost (BT-boost) or Stereotactic Body Radiation Therapy Boost (SBRT-boost) For High-Risk Prostate Cancer (HR-PCa)Document10 pagesBrachytherapy Boost (BT-boost) or Stereotactic Body Radiation Therapy Boost (SBRT-boost) For High-Risk Prostate Cancer (HR-PCa)Oncología CdsNo ratings yet
- Fonc 13 1162683Document2 pagesFonc 13 1162683vinadata01No ratings yet
- Accepted Manuscript: Colloids and Surfaces B: BiointerfacesDocument33 pagesAccepted Manuscript: Colloids and Surfaces B: BiointerfacesPrity DafdeNo ratings yet
- Role of Apalutamide in The Treatment Landscape For Patients With Advanced Prostate Cancer: An Expert Opinion Statement of European Clinical PracticeDocument9 pagesRole of Apalutamide in The Treatment Landscape For Patients With Advanced Prostate Cancer: An Expert Opinion Statement of European Clinical Practicesid sidNo ratings yet
- 2021 Molecular Basis of Prostate Cancer. FixDocument40 pages2021 Molecular Basis of Prostate Cancer. FixIrfandi AmiruddinNo ratings yet
- Soton - Ac.uk Ude Personalfiles Users Sjc7 Mydesktop Art 10.1186 s13148-016-0264-8Document24 pagesSoton - Ac.uk Ude Personalfiles Users Sjc7 Mydesktop Art 10.1186 s13148-016-0264-8Eduardo Jorge pintoNo ratings yet
- The-Impact-On-Load-balancing-In-Cloud-Computing 2020Document5 pagesThe-Impact-On-Load-balancing-In-Cloud-Computing 2020Nikola JovanovicNo ratings yet
- Springer Nature Latex TemplateDocument13 pagesSpringer Nature Latex TemplateAndres FloresNo ratings yet
- Organic Halides Introduction Class-1 NotesDocument15 pagesOrganic Halides Introduction Class-1 Notessiddhartha singhNo ratings yet
- Tut Sheet7Document2 pagesTut Sheet7Ekta SharmaNo ratings yet
- CentrifugationDocument10 pagesCentrifugationBk FNo ratings yet
- Ged Test Accom App AdhdDocument7 pagesGed Test Accom App AdhdJeannette DorfmanNo ratings yet
- 12feb Quickref Views enDocument148 pages12feb Quickref Views enprakash2709No ratings yet
- SkillsDocument7 pagesSkillsRufus RajNo ratings yet
- Analysis of StructureDocument4 pagesAnalysis of StructureCarlson CaliwanNo ratings yet
- Hayden Esterak Resume 1Document1 pageHayden Esterak Resume 1api-666885986No ratings yet
- Create Database Taller-AdalbertoDocument2 pagesCreate Database Taller-AdalbertoAdalberto GonzalezNo ratings yet
- Akira - GA - Intro-To-Coding-Html-CssDocument46 pagesAkira - GA - Intro-To-Coding-Html-CssVinoth JayaprakasamNo ratings yet
- Web Lab PDFDocument6 pagesWeb Lab PDFDevesh PandeyNo ratings yet
- EXOS Quick Guide - Cheat SheetDocument19 pagesEXOS Quick Guide - Cheat Sheetmaverick2689No ratings yet
- Design of Stair CaseDocument2 pagesDesign of Stair Casepathan is khanNo ratings yet
- Person To PersonDocument126 pagesPerson To PersonYalmi AdiNo ratings yet
- Power Electronics: Thyristor Controlled Power For Electric MotorsDocument10 pagesPower Electronics: Thyristor Controlled Power For Electric Motorsshahab moinNo ratings yet
- Grade 7 Lesson: ReproductionDocument4 pagesGrade 7 Lesson: ReproductionJoedelyn Wagas100% (2)
- Thrift Banks ActDocument25 pagesThrift Banks ActMadelle Pineda100% (1)
- Gl04 FM Tam 019 FsefDocument4 pagesGl04 FM Tam 019 FsefManish TiwariNo ratings yet
- 10 Science NcertSolutions Chapter 8 ExercisesDocument4 pages10 Science NcertSolutions Chapter 8 ExercisesAnita GargNo ratings yet
- MT2OL-Ia6 2 1Document136 pagesMT2OL-Ia6 2 1QUILIOPE, JUSTINE JAY S.No ratings yet
- Hot Cool 3 2012Document32 pagesHot Cool 3 2012thermosol5416No ratings yet
- Plastic and Paper PDFDocument12 pagesPlastic and Paper PDFBhanu Pratap SolankiNo ratings yet
- World's No.1 LCD/LED Solution Designer World's Leading Interactive & Collaboration Solution BrandDocument3 pagesWorld's No.1 LCD/LED Solution Designer World's Leading Interactive & Collaboration Solution BrandINTELL WAVESNo ratings yet
- 9de13c0f0c009828f703d0103efa820b.xlsDocument70 pages9de13c0f0c009828f703d0103efa820b.xlsPreeti JaiswalNo ratings yet
- General Revision For Treasury Management (Please See That You Can Answer The Following 32 Questions and The MCQS)Document14 pagesGeneral Revision For Treasury Management (Please See That You Can Answer The Following 32 Questions and The MCQS)RoelienNo ratings yet
- Chemical Fume Hood HandbookDocument11 pagesChemical Fume Hood Handbookkumar123rajuNo ratings yet