Download as pdf or txt
You might also like
- 489 FullDocument9 pages489 FullHellenaNo ratings yet
- Anesthesia For Robot-Assisted Radical Prostatectomy A Challenge For AnesthesiologistDocument5 pagesAnesthesia For Robot-Assisted Radical Prostatectomy A Challenge For AnesthesiologistMonse ContrerasNo ratings yet
- Clinical Effects of Pleurotomy On Patients Undergoing CABGDocument5 pagesClinical Effects of Pleurotomy On Patients Undergoing CABGBeshoy KhelaNo ratings yet
- Pda Ev Ejtcs 04Document7 pagesPda Ev Ejtcs 04emmanuel le bretNo ratings yet
- Casali 2009Document6 pagesCasali 2009Giancarlo Maruri MunarettoNo ratings yet
- JTD 13 03 1886Document13 pagesJTD 13 03 1886Nongnapat KettungmunNo ratings yet
- FCVM 09 750896Document10 pagesFCVM 09 750896S Ram KishoreNo ratings yet
- 7-Advantages of Applying Digital Chest Drainage System For Postoperative Management of Patients Following Pulmonary Resection A Systematic Review and Meta-Analysis of 12 Randomized Controlled TrialsDocument11 pages7-Advantages of Applying Digital Chest Drainage System For Postoperative Management of Patients Following Pulmonary Resection A Systematic Review and Meta-Analysis of 12 Randomized Controlled Trialszhouliying684No ratings yet
- Chronic Total OcclusionsDocument37 pagesChronic Total OcclusionsValentin CHIONCELNo ratings yet
- Faaiez VATSDocument19 pagesFaaiez VATSFaaiez FarooqNo ratings yet
- The Extracardiac Fontan Procedure Withoutncardiopulmonary BypassDocument6 pagesThe Extracardiac Fontan Procedure Withoutncardiopulmonary BypassEko SiswantoNo ratings yet
- Bmri2016 3741426Document7 pagesBmri2016 3741426MandaNo ratings yet
- Reduction of Air Leakage Using Linear Staple Device With BioabsorbableDocument7 pagesReduction of Air Leakage Using Linear Staple Device With BioabsorbableMohamed GamalNo ratings yet
- 2022 Article 1790Document7 pages2022 Article 1790juajimenez55No ratings yet
- Techniques and Outcomes of Bronchoplastic and Sleeve Resection: An 8-Year Single-Center ExperienceDocument11 pagesTechniques and Outcomes of Bronchoplastic and Sleeve Resection: An 8-Year Single-Center ExperienceJovelyn SagangNo ratings yet
- PIIS0022522311007525Document10 pagesPIIS0022522311007525Enrico SquiccimarroNo ratings yet
- Tiroidectomía VideoasistidaDocument6 pagesTiroidectomía Videoasistidadavid villamilNo ratings yet
- Video-Assisted Thoracoscopic Surgery (VATS) Lobectomy: Catastrophic Intraoperative ComplicationsDocument6 pagesVideo-Assisted Thoracoscopic Surgery (VATS) Lobectomy: Catastrophic Intraoperative ComplicationsAlin Ionut BurlacuNo ratings yet
- Prehospital Thoracotomy A Commentary-JmlphDocument3 pagesPrehospital Thoracotomy A Commentary-Jmlpheditorial.boardNo ratings yet
- A Retrospective Clinical Study: Complications of Totally Implanted Central Venous Access PortsDocument6 pagesA Retrospective Clinical Study: Complications of Totally Implanted Central Venous Access PortsAmber CarterNo ratings yet
- Minimally Invasive Perventricular Device Occlusion Versus Surgical Closure For Treating Perimembranous Ventricular Septal DefectDocument10 pagesMinimally Invasive Perventricular Device Occlusion Versus Surgical Closure For Treating Perimembranous Ventricular Septal DefectRinzyNo ratings yet
- Cardio1 PDFDocument7 pagesCardio1 PDFAyu SuprabawatiNo ratings yet
- Swanson 2007Document5 pagesSwanson 2007Giancarlo Maruri MunarettoNo ratings yet
- 2022 Respiron Ressecao Pulmonar Revisao Com MetanaliseDocument8 pages2022 Respiron Ressecao Pulmonar Revisao Com MetanaliseFrederico GarciaNo ratings yet
- AnnCardAnaesth15154-6423638 175036Document10 pagesAnnCardAnaesth15154-6423638 175036ElenaCondratscribdNo ratings yet
- Early and Long-Term Outcomes of Minimally Invasive Mitral Valve Surgery Through Right Minithoracotomy: A 10-Year Experience in 1604 PatientsDocument9 pagesEarly and Long-Term Outcomes of Minimally Invasive Mitral Valve Surgery Through Right Minithoracotomy: A 10-Year Experience in 1604 PatientsEnrico SquiccimarroNo ratings yet
- J Thromb Thrombolysis 2020 Sep 14 Smith DDocument8 pagesJ Thromb Thrombolysis 2020 Sep 14 Smith DFernando SousaNo ratings yet
- Percutaneous Aortic Valve Implantation: The Anesthesiologist PerspectiveDocument11 pagesPercutaneous Aortic Valve Implantation: The Anesthesiologist Perspectiveserena7205No ratings yet
- Deep Breath & SpirometerDocument7 pagesDeep Breath & SpirometerAsmaa GamalNo ratings yet
- Modified 2 CM Super Single Port vs. The Traditional 3 CM Single Port For Video Assisted Thoracoscopic Surgery LobectomyDocument8 pagesModified 2 CM Super Single Port vs. The Traditional 3 CM Single Port For Video Assisted Thoracoscopic Surgery LobectomyAlin Ionut BurlacuNo ratings yet
- s12872 019 1096 1Document9 pagess12872 019 1096 1sarahNo ratings yet
- 2017 Ultrasound-Guided Central Venous CatheterizationDocument14 pages2017 Ultrasound-Guided Central Venous Catheterizationeswin yoelNo ratings yet
- Role of Spirometry in Post CABG PtsDocument11 pagesRole of Spirometry in Post CABG PtsBeshoy KhelaNo ratings yet
- Medicine: Observational StudyDocument8 pagesMedicine: Observational StudyAlin Ionut BurlacuNo ratings yet
- Anesthesia For Major Urologic Surgery: James O.B. Cockcroft,, Colin B. Berry,, John S. Mcgrath,, Mark O. DaughertyDocument8 pagesAnesthesia For Major Urologic Surgery: James O.B. Cockcroft,, Colin B. Berry,, John S. Mcgrath,, Mark O. DaughertyJEFFERSON MUÑOZNo ratings yet
- FormosJSurg51250-7751411 213154Document8 pagesFormosJSurg51250-7751411 213154Deddy WidjajaNo ratings yet
- Tavi SurgeryDocument10 pagesTavi Surgeryapi-683799701No ratings yet
- Risk Model DialysiddssssDocument7 pagesRisk Model DialysiddssssDumitru GrozaNo ratings yet
- Video-Assisted Thoracoscopic Surgery For Early Evacuation of Traumatic Clotted HemothoracesDocument6 pagesVideo-Assisted Thoracoscopic Surgery For Early Evacuation of Traumatic Clotted Hemothoracesdella oktavianiNo ratings yet
- Resuscitative Endovascular Balloon Occlusion of The Aorta (REBOA) : An Updated ReviewDocument9 pagesResuscitative Endovascular Balloon Occlusion of The Aorta (REBOA) : An Updated ReviewLuis-alfredo Perez Bolde HernandezNo ratings yet
- Systematic Review Go WakaDocument8 pagesSystematic Review Go WakaNoemi Di FucciaNo ratings yet
- Tracheostomy in The Intensive Care Unit A University Hospital in A Developing Country StudyDocument5 pagesTracheostomy in The Intensive Care Unit A University Hospital in A Developing Country StudycendyjulianaNo ratings yet
- Gaudet 2016Document11 pagesGaudet 2016Giancarlo Maruri MunarettoNo ratings yet
- Case Report: Percutaneous Punctured Transcatheter Device Closure of Residual Shunt After Ventricular Septal Defect RepairDocument4 pagesCase Report: Percutaneous Punctured Transcatheter Device Closure of Residual Shunt After Ventricular Septal Defect Repairyayu latifahNo ratings yet
- Planning For Minimally Invasive Aortic Valve Replacement - Key Steps For Patient AssessmentDocument6 pagesPlanning For Minimally Invasive Aortic Valve Replacement - Key Steps For Patient AssessmentlkulacogluNo ratings yet
- Lung BiopsyDocument8 pagesLung BiopsySiya PatilNo ratings yet
- Jurnal 5Document7 pagesJurnal 5nskhldNo ratings yet
- 2.8.2 Pulmonary SurgeryDocument11 pages2.8.2 Pulmonary SurgeryZayan SyedNo ratings yet
- Midterm Outcomes of Minimally Invasive Mitral Valve Surgery in A Heterogeneous Valve Pathology Cohort: Respect or Resect?Document12 pagesMidterm Outcomes of Minimally Invasive Mitral Valve Surgery in A Heterogeneous Valve Pathology Cohort: Respect or Resect?mony saNo ratings yet
- Ijerph 17 01205 v2 PDFDocument10 pagesIjerph 17 01205 v2 PDFMuhammad Ricky RamadhianNo ratings yet
- Mitral Durability After Robotic Mitral Valve Repair: Analysis of 200 Consecutive Mitral Regurgitation RepairsDocument7 pagesMitral Durability After Robotic Mitral Valve Repair: Analysis of 200 Consecutive Mitral Regurgitation RepairsEnrico SquiccimarroNo ratings yet
- 1 s2.0 S2468294221000605 MainDocument7 pages1 s2.0 S2468294221000605 MainVishal BasuNo ratings yet
- Anesthesia For Carotid Endarterectomy: Where Do We Stand at Present?Document12 pagesAnesthesia For Carotid Endarterectomy: Where Do We Stand at Present?Lil_QuinceNo ratings yet
- GJHS 6 221Document5 pagesGJHS 6 221Teuku FaisalNo ratings yet
- TMP 99 BADocument6 pagesTMP 99 BAFrontiersNo ratings yet
- Does Pleurotomy Affects Respiratory FunctionsDocument7 pagesDoes Pleurotomy Affects Respiratory FunctionsBeshoy KhelaNo ratings yet
- Single-Incision Thoracoscopic Surgery For Primary Spontaneous PneumothoraxDocument4 pagesSingle-Incision Thoracoscopic Surgery For Primary Spontaneous PneumothoraxRiani NazilaNo ratings yet
- Pneumothorax As A Complication of Central Venous Catheter InsertionDocument10 pagesPneumothorax As A Complication of Central Venous Catheter Insertionnanang hidayatullohNo ratings yet
- 096 - EIJ E 24 00008 - AliDocument3 pages096 - EIJ E 24 00008 - AliFrancisco Javier Robles OrtizNo ratings yet
- Atlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosFrom EverandAtlas of 3D Transesophageal Echocardiography in Structural Heart Disease Interventions: Cases and VideosNo ratings yet
- 2021 Article 1401Document13 pages2021 Article 1401Apotik ApotekNo ratings yet
- Epidemiology, Phenotype, and Genetics of The Polycystic Ovary Syndrome in AdultsDocument23 pagesEpidemiology, Phenotype, and Genetics of The Polycystic Ovary Syndrome in AdultsApotik ApotekNo ratings yet
- Abbas 2014Document6 pagesAbbas 2014Apotik ApotekNo ratings yet
- Few Complications After Paracentesis in Patients With Cirrhosis and Refractory AscitesDocument5 pagesFew Complications After Paracentesis in Patients With Cirrhosis and Refractory AscitesApotik ApotekNo ratings yet
- Snakebite Envenoming: A Strategy For Prevention and ControlDocument70 pagesSnakebite Envenoming: A Strategy For Prevention and ControlApotik ApotekNo ratings yet
- Acta Obstet Gynecol Scand - 2019 - Litwinska - Ventriculo Amniotic Shunting For Severe Fetal VentriculomegalyDocument6 pagesActa Obstet Gynecol Scand - 2019 - Litwinska - Ventriculo Amniotic Shunting For Severe Fetal VentriculomegalyApotik ApotekNo ratings yet
- Acta Obstet Gynecol Scand - 2013 - Matsubara - Intrauterine Balloon Occlusion During Cesarean Hysterectomy For PlacentaDocument2 pagesActa Obstet Gynecol Scand - 2013 - Matsubara - Intrauterine Balloon Occlusion During Cesarean Hysterectomy For PlacentaApotik ApotekNo ratings yet
- Accuracy of Real-Time Shear Wave Elastography in SDocument10 pagesAccuracy of Real-Time Shear Wave Elastography in SApotik ApotekNo ratings yet
- Archive of SIDDocument6 pagesArchive of SIDApotik ApotekNo ratings yet
- Ventilator-Associated Pneumonia in Neonates and Children: A Systematic Analysis of Diagnostic Methods and PreventionDocument16 pagesVentilator-Associated Pneumonia in Neonates and Children: A Systematic Analysis of Diagnostic Methods and PreventionApotik ApotekNo ratings yet
- Abdelkhalekabdelrazek 2021Document8 pagesAbdelkhalekabdelrazek 2021Apotik ApotekNo ratings yet
- Cryotherapy STING OSA Clinical TrialDocument4 pagesCryotherapy STING OSA Clinical TrialApotik ApotekNo ratings yet
- A3 FullDocument2 pagesA3 FullApotik ApotekNo ratings yet
- Davis 2003Document9 pagesDavis 2003Apotik ApotekNo ratings yet
- Depression Among Dialysis Patients: National Kidney Foundation Journal of Nephrology Social Work, Volume 40, Issue 2Document4 pagesDepression Among Dialysis Patients: National Kidney Foundation Journal of Nephrology Social Work, Volume 40, Issue 2Apotik ApotekNo ratings yet
- 528-Article Text-2283-1-10-20220418Document9 pages528-Article Text-2283-1-10-20220418Apotik ApotekNo ratings yet
- Identification of Precipitating Factors in Hepatic Encephalopathy Patients at Liaquat University Hospital JamshoroDocument6 pagesIdentification of Precipitating Factors in Hepatic Encephalopathy Patients at Liaquat University Hospital JamshoroApotik ApotekNo ratings yet
- 1 s2.0 S109037980870268X MainDocument1 page1 s2.0 S109037980870268X MainApotik ApotekNo ratings yet
- 10 1089@lap 2020 0179Document7 pages10 1089@lap 2020 0179Apotik ApotekNo ratings yet
- Addis Ababa University: College of Business and Economics Department of Accounting and FinanceDocument5 pagesAddis Ababa University: College of Business and Economics Department of Accounting and FinanceAsteway MesfinNo ratings yet
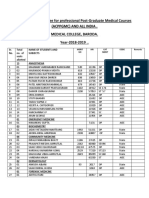
- Admission Committee For Professional Post-Graduate Medical Courses (Acppgmc) and All India - Medical College, Baroda. Year-2018-2019 .Document5 pagesAdmission Committee For Professional Post-Graduate Medical Courses (Acppgmc) and All India - Medical College, Baroda. Year-2018-2019 .Abhishek JoshiNo ratings yet
- Mobilna Protetika-PriručnikDocument150 pagesMobilna Protetika-PriručnikAleksandar Vukosav100% (1)
- Workplace ViolenceDocument383 pagesWorkplace ViolenceAmeni Hlioui ChokriNo ratings yet
- Carter Procession Closure MapDocument1 pageCarter Procession Closure Mapcookiespiffey21No ratings yet
- Human Resource Management - AMRI MKPDocument123 pagesHuman Resource Management - AMRI MKPSayantan MandalNo ratings yet
- Modern Technology of Food Processing & Agro Based Industries (2nd Edn.)Document8 pagesModern Technology of Food Processing & Agro Based Industries (2nd Edn.)Bala Ratnakar KoneruNo ratings yet
- Cristobal, Rocelyn P. MS Lec Post Task Triage FinalDocument10 pagesCristobal, Rocelyn P. MS Lec Post Task Triage FinalRocelyn CristobalNo ratings yet
- Competent Supervision-Emerging PracticesDocument17 pagesCompetent Supervision-Emerging Practicesapi-626136134No ratings yet
- ReportDocument24 pagesReportSugu GohainNo ratings yet
- Pancreatic Cancer StagingDocument1 pagePancreatic Cancer StagingShashankNo ratings yet
- D Unit Male Result 2019 20Document9 pagesD Unit Male Result 2019 20asifhlc026No ratings yet
- Đáp Án ReadingDocument2 pagesĐáp Án ReadingLanAnhNo ratings yet
- Factors Affecting The Travel and Tourism Industry 2Document9 pagesFactors Affecting The Travel and Tourism Industry 2thapar1teenaNo ratings yet
- CE Laws 4140 Phil Labor Code 2Document5 pagesCE Laws 4140 Phil Labor Code 2jun junNo ratings yet
- Author: JANET C. TAER 0 School/Station: Taligaman National High School Division: BUTUAN CITY Email Address: Janet - Taer@deped - Gov.phDocument11 pagesAuthor: JANET C. TAER 0 School/Station: Taligaman National High School Division: BUTUAN CITY Email Address: Janet - Taer@deped - Gov.phShekaina Faith Cuizon LozadaNo ratings yet
- Key Partner Types: Pharm-Bio Technology and Traditional Medicine Centre (PHARMBIOTRAC)Document2 pagesKey Partner Types: Pharm-Bio Technology and Traditional Medicine Centre (PHARMBIOTRAC)anke2009weisheitNo ratings yet
- Makadia J.J. 52670Document174 pagesMakadia J.J. 52670umaNo ratings yet
- Hema Nclex Q'SDocument6 pagesHema Nclex Q'SFarmisa MannanNo ratings yet
- Efektivitas Intervensi Colek Dalam Peningkatan Perilaku Patient SafetyDocument7 pagesEfektivitas Intervensi Colek Dalam Peningkatan Perilaku Patient SafetyFaidh AhmadNo ratings yet
- JournalofPeriodontology 2022 Chambrone EfficacyofbiologicsinrootcoverageandgingivalaugmentationtherapyAnDocument33 pagesJournalofPeriodontology 2022 Chambrone EfficacyofbiologicsinrootcoverageandgingivalaugmentationtherapyAn安西 泰規No ratings yet
- AstraZeneca AB Et. Al. v. Mylan Laboratories Et. Al.Document16 pagesAstraZeneca AB Et. Al. v. Mylan Laboratories Et. Al.PriorSmartNo ratings yet
- Union Civil Protection Mechanism: More Effective, Efficient and Coherent Disaster ManagementDocument23 pagesUnion Civil Protection Mechanism: More Effective, Efficient and Coherent Disaster ManagementCătălin Marian IvanNo ratings yet
- Nazarita - Concept of Community and Envi HealthDocument37 pagesNazarita - Concept of Community and Envi HealthCess NazaritaNo ratings yet
- Bio-Psychosocial Demara Final AssessmentDocument8 pagesBio-Psychosocial Demara Final Assessmentapi-311012291No ratings yet
- Irb DocumentsDocument17 pagesIrb Documentsapi-486275760No ratings yet
- Diagnosed With Low Sodium in The BloodDocument2 pagesDiagnosed With Low Sodium in The BloodShweta KhannaNo ratings yet
- Intellicare - Orientation DeckDocument54 pagesIntellicare - Orientation DeckLeinad Edino CruzNo ratings yet
- Module 1 Road To TheRight Choice - Jan7Document68 pagesModule 1 Road To TheRight Choice - Jan7Man Havvy100% (15)
- Structural Basis For GLP-1 Receptor Activation by LY3502970, An Orally Active Nonpeptide AgonistDocument9 pagesStructural Basis For GLP-1 Receptor Activation by LY3502970, An Orally Active Nonpeptide AgonistClay GranerNo ratings yet