Download as pdf or txt
You might also like
- Compre Prob Set 4Document42 pagesCompre Prob Set 4Aira Isahmay Galope Carpio0% (1)
- Bodkin - Time Between RTP Assessments To Achieve Strength Gains post-ACLR - 2019Document8 pagesBodkin - Time Between RTP Assessments To Achieve Strength Gains post-ACLR - 2019krayfieldNo ratings yet
- Anterior Cruciate Ligament Reconstruction Rehabilitation: MOON GuidelinesDocument5 pagesAnterior Cruciate Ligament Reconstruction Rehabilitation: MOON GuidelinesSilvy OktavianaNo ratings yet
- 1 s2.0 S1440244021000554 Main PDFDocument9 pages1 s2.0 S1440244021000554 Main PDFEvelyn MalaguttiNo ratings yet
- NIH Public AccessDocument33 pagesNIH Public AccessAulida Arum MNo ratings yet
- ¿Es La Fuerza Preoperatoria Del Cuádriceps Un Factor Predictivo de Los Resultados de Las Reconstrucciones Del Ligamento Cruzado Anterior.Document9 pages¿Es La Fuerza Preoperatoria Del Cuádriceps Un Factor Predictivo de Los Resultados de Las Reconstrucciones Del Ligamento Cruzado Anterior.contact.movementsiteNo ratings yet
- Muller Et Al 2023 Favorable Patient Reported Clinical and Functional Outcomes 2 Years After Acl Repair andDocument11 pagesMuller Et Al 2023 Favorable Patient Reported Clinical and Functional Outcomes 2 Years After Acl Repair andDeivisonNo ratings yet
- ManskeProhaskaLucas CRMM ACL2012Document16 pagesManskeProhaskaLucas CRMM ACL2012Dr.upendra goudNo ratings yet
- Bregenhof 2018Document13 pagesBregenhof 2018Rizal612No ratings yet
- ACL WorkloadDocument9 pagesACL WorkloadniekoNo ratings yet
- 荷兰2016 循证临床实践指南:前交叉韧带康复Document14 pages荷兰2016 循证临床实践指南:前交叉韧带康复Roger PanNo ratings yet
- Journal AldhitaDocument7 pagesJournal Aldhitaussi27No ratings yet
- Best Practice & Research Clinical RheumatologyDocument15 pagesBest Practice & Research Clinical RheumatologyKristi Natalia PesireronNo ratings yet
- Expectations For Return To Preinjury Sport Before and After Anterior Cruciate Ligament ReconstructionDocument6 pagesExpectations For Return To Preinjury Sport Before and After Anterior Cruciate Ligament ReconstructionYusufa ArdyNo ratings yet
- Best Practice & Research Clinical Rheumatology: Stephanie R. Filbay, Hege GrindemDocument15 pagesBest Practice & Research Clinical Rheumatology: Stephanie R. Filbay, Hege GrindemEduardo Santana SuárezNo ratings yet
- Ptpii - Inservice Final 2Document3 pagesPtpii - Inservice Final 2api-640939939No ratings yet
- American Journal of Sports Medicine, 38, 2201-2210Document31 pagesAmerican Journal of Sports Medicine, 38, 2201-2210randocalNo ratings yet
- Effect of Whole-Body Vibration On Sagittal Plane in ACLRDocument8 pagesEffect of Whole-Body Vibration On Sagittal Plane in ACLRhasma azisNo ratings yet
- ACL Return To Sport Guidelines and CriteriaDocument8 pagesACL Return To Sport Guidelines and CriteriaCamila Nicole Madrid GonzalezNo ratings yet
- Guideline LCADocument13 pagesGuideline LCAluccanicheleNo ratings yet
- Physical Therapy in Sport: Ryan Lobb, Steve Tumilty, Leica S. ClaydonDocument9 pagesPhysical Therapy in Sport: Ryan Lobb, Steve Tumilty, Leica S. Claydonilona ilincaNo ratings yet
- Rehabilitation and Return To Sports After Acl ReconstructionDocument5 pagesRehabilitation and Return To Sports After Acl ReconstructionjasonoytumandukNo ratings yet
- Evidence Based Clinical Practice Update PracticeDocument14 pagesEvidence Based Clinical Practice Update PracticeYoni ZarkhNo ratings yet
- Best Practice & Research Clinical Rheumatology: Stephanie R. Filbay, Hege GrindemDocument15 pagesBest Practice & Research Clinical Rheumatology: Stephanie R. Filbay, Hege GrindemKristi Natalia PesireronNo ratings yet
- 1506 FullDocument13 pages1506 FullCARLOS FRANCISCO CAMPOVERDE CALLENo ratings yet
- Coper Classification After ACL Rupture (Thoma Et Al 2019)Document8 pagesCoper Classification After ACL Rupture (Thoma Et Al 2019)nsboyadzhievNo ratings yet
- 1506 FullDocument13 pages1506 FullAugusto ManoelNo ratings yet
- Anterior Cruciate Ligament Injury-Who Succeeds WitDocument9 pagesAnterior Cruciate Ligament Injury-Who Succeeds WitNura Eky VNo ratings yet
- Evidence-Based Clinical Practice Update: Practice Guidelines For Anterior Cruciate Ligament Rehabilitation Based On A Systematic Review and Multidisciplinary ConsensusDocument13 pagesEvidence-Based Clinical Practice Update: Practice Guidelines For Anterior Cruciate Ligament Rehabilitation Based On A Systematic Review and Multidisciplinary ConsensusluigiNo ratings yet
- Acl Reconstruction With Bone Tendon Bone Allografts Improved With Bmac InjectionDocument10 pagesAcl Reconstruction With Bone Tendon Bone Allografts Improved With Bmac InjectionFer JorgeNo ratings yet
- Anterior Cruciate Ligament Reconstruction, Rehabilitation, and Return To Play: 2015 UpdateDocument12 pagesAnterior Cruciate Ligament Reconstruction, Rehabilitation, and Return To Play: 2015 UpdateAulida Arum MNo ratings yet
- Cartilage Sports16Document19 pagesCartilage Sports16scribidubiduNo ratings yet
- Isokinetic Testing Why It Is More Important TodayDocument7 pagesIsokinetic Testing Why It Is More Important TodayChristina LushchynskaNo ratings yet
- Avances LCA WilkDocument19 pagesAvances LCA WilkCarlos Martín De RosasNo ratings yet
- Post-Operative Criterion Based Rehabilitation of Acl Repairs: A Clinical CommentaryDocument14 pagesPost-Operative Criterion Based Rehabilitation of Acl Repairs: A Clinical CommentaryferryNo ratings yet
- Kraus 2021Document7 pagesKraus 2021翁嘉聰No ratings yet
- Aclr GuidelinesDocument15 pagesAclr GuidelinesMohamed GamalNo ratings yet
- 2016 The American Society of Shoulder and ElbowDocument15 pages2016 The American Society of Shoulder and ElbowDiego De Farias Diehl100% (1)
- 10 1016@j Arthro 2019 08 047Document5 pages10 1016@j Arthro 2019 08 047David CamposNo ratings yet
- Simple Decision Rules Can Reduce Reinjury Risk by 84% After ACL Reconstruction: The Delaware-Oslo ACL Cohort StudyDocument6 pagesSimple Decision Rules Can Reduce Reinjury Risk by 84% After ACL Reconstruction: The Delaware-Oslo ACL Cohort StudyTiago EstevesNo ratings yet
- Rehabilitation and Return To Sport Testing After ADocument6 pagesRehabilitation and Return To Sport Testing After ATotti DevaNo ratings yet
- The Influence, Barriers to and Facilitators of Anterior Cruciate Ligament Rehabilitation Adherence and Participation a Scoping ReviewDocument22 pagesThe Influence, Barriers to and Facilitators of Anterior Cruciate Ligament Rehabilitation Adherence and Participation a Scoping ReviewTamas KalmarNo ratings yet
- KNEE Early Outc Kinematic Retain TKR MCPS Knee 2022 HarveyDocument9 pagesKNEE Early Outc Kinematic Retain TKR MCPS Knee 2022 HarveyPrabhjeet singhNo ratings yet
- The Relationship of Knee-Related Quality of - Life With Function, Psychological Factors, - Strength, Performance, and Postural - Stability After ACL Reconstruction - A Cross-Sectional StudyDocument7 pagesThe Relationship of Knee-Related Quality of - Life With Function, Psychological Factors, - Strength, Performance, and Postural - Stability After ACL Reconstruction - A Cross-Sectional StudyThyago AraujoNo ratings yet
- Is Reconstruction The Best Management Strategy For Anterior CruciateDocument9 pagesIs Reconstruction The Best Management Strategy For Anterior CruciateItai IzhakNo ratings yet
- Hop Testing Provides A Reliable and Valid Outcome Measure During Rehabilitation After Anterior Cruciate Ligament Reconstruction PDFDocument13 pagesHop Testing Provides A Reliable and Valid Outcome Measure During Rehabilitation After Anterior Cruciate Ligament Reconstruction PDFCleber PimentaNo ratings yet
- The Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalDocument4 pagesThe Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalEditor IJTSRDNo ratings yet
- Nihms782171 PDFDocument15 pagesNihms782171 PDFjacknatalieNo ratings yet
- A Systematic Review of Evidence For Anterior Cruciate Ligament Rehabilitation How Much and What TDocument21 pagesA Systematic Review of Evidence For Anterior Cruciate Ligament Rehabilitation How Much and What TRuben CapelaNo ratings yet
- Exercise-Based ApproachDocument4 pagesExercise-Based Approachfederico BiettiNo ratings yet
- 2018 Mejoras en La Biomecánica Del Aterrizaje Después de La Reconstrucción Del Ligamento Cruzado Anterior en Atletas Adolescentes.Document13 pages2018 Mejoras en La Biomecánica Del Aterrizaje Después de La Reconstrucción Del Ligamento Cruzado Anterior en Atletas Adolescentes.contact.movementsiteNo ratings yet
- Clinical Orthopaedics and Related Research: A Publication of The Association of Bone and Joint Surgeons®Document12 pagesClinical Orthopaedics and Related Research: A Publication of The Association of Bone and Joint Surgeons®Ira AdventiaNo ratings yet
- LCA Psicologico 2Document6 pagesLCA Psicologico 2MarianoNo ratings yet
- Miller 2016Document9 pagesMiller 2016Dario GerpeNo ratings yet
- Pre and Post-Operative Rehabilitation of Anterior Cruciate Ligament Reconstruction in Young AthletesDocument11 pagesPre and Post-Operative Rehabilitation of Anterior Cruciate Ligament Reconstruction in Young AthletesferryNo ratings yet
- Knee LigDocument48 pagesKnee LiglizNo ratings yet
- ACL Surgery Necessity in Non-Acute Patients (ACL SNNAP) : A Statistical Analysis Plan For A Randomised Controlled TrialDocument9 pagesACL Surgery Necessity in Non-Acute Patients (ACL SNNAP) : A Statistical Analysis Plan For A Randomised Controlled Trialchan kyoNo ratings yet
- Rhim 2020Document9 pagesRhim 2020MatkoNo ratings yet
- Return To Sport Following Anterior Cruciate Ligament Reconstruction Surgery: A Systematic Review and Meta-Analysis of The State of PlayDocument11 pagesReturn To Sport Following Anterior Cruciate Ligament Reconstruction Surgery: A Systematic Review and Meta-Analysis of The State of Playjuanpablo.ramon20No ratings yet
- Recent Advances in The Rehabilitation LCADocument19 pagesRecent Advances in The Rehabilitation LCAMiguel Andres Sepulveda CastroNo ratings yet
- XdealSkin Vitamins Tiktok ProposalDocument4 pagesXdealSkin Vitamins Tiktok ProposalElixia KiteNo ratings yet
- 0068 NehaDocument1 page0068 Nehang.neha8990No ratings yet
- SPAR International Annual Report 2018 PDFDocument56 pagesSPAR International Annual Report 2018 PDFCristian Cucos CucosNo ratings yet
- 1 120623 DAP产品价格目录文档 (Grosir)Document21 pages1 120623 DAP产品价格目录文档 (Grosir)Friska AyuNo ratings yet
- GT 1 Paper 2 SolutionsDocument12 pagesGT 1 Paper 2 SolutionsAnand MurugananthamNo ratings yet
- 003.ladders - Rev. 0Document25 pages003.ladders - Rev. 0narasimhamurthy414No ratings yet
- The Golden Fish Keeps A Promise StoryDocument2 pagesThe Golden Fish Keeps A Promise StoryDe Guzman Diane Marie B.No ratings yet
- ANT332 Answer Key 6Document3 pagesANT332 Answer Key 6mariefmuntheNo ratings yet
- Chart For Contraception:: PreventsDocument1 pageChart For Contraception:: PreventsAngelica May ClaritoNo ratings yet
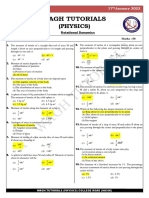
- Mock Test - 98 (17 Jan 2023) Rotational DynamicsDocument1 pageMock Test - 98 (17 Jan 2023) Rotational DynamicsparamNo ratings yet
- A Proposal On Reusable Sanitary PADSDocument16 pagesA Proposal On Reusable Sanitary PADSMike AbbeyNo ratings yet
- CSRDocument16 pagesCSRAnkit YadavNo ratings yet
- Lectures On The Comparative Grammar of The Semitic LanguagesDocument308 pagesLectures On The Comparative Grammar of The Semitic LanguagesRob Cordopatri100% (1)
- Technology of Apple Compote Production For Baby FoDocument6 pagesTechnology of Apple Compote Production For Baby FoMaria Elena CueltanNo ratings yet
- CAD Sales Request 16053-0 Scope of Supply Preview: DEUTZ Engine DocumentationDocument4 pagesCAD Sales Request 16053-0 Scope of Supply Preview: DEUTZ Engine DocumentationEric ChuNo ratings yet
- Electrical Resistance Lecture 2Document5 pagesElectrical Resistance Lecture 2bigbang0% (1)
- Msds Aceite de Sacha Inchi Indice de RefracciónDocument5 pagesMsds Aceite de Sacha Inchi Indice de Refraccióngabriela_moron_aNo ratings yet
- Second Order Runge-Kutta Method: ExampleDocument9 pagesSecond Order Runge-Kutta Method: ExampleAhmed MobarkiNo ratings yet
- KPI FormulaDocument3 pagesKPI FormulaSrikant GuptaNo ratings yet
- Chapter 8 v8.1Document113 pagesChapter 8 v8.1ANTONYNo ratings yet
- DD RhinosinusitisDocument9 pagesDD RhinosinusitisZuhal Darwis100% (1)
- Bed and Bathroom Linen - 29.12.2020Document2 pagesBed and Bathroom Linen - 29.12.2020Eden Led LightingNo ratings yet
- Mindfulness Based Cognitive Therapy For Children Results of A Pilot StudyDocument12 pagesMindfulness Based Cognitive Therapy For Children Results of A Pilot StudyAcong KentutNo ratings yet
- Anita Longley's LegacyDocument4 pagesAnita Longley's LegacyJill TietjenNo ratings yet
- Module 7Document5 pagesModule 7marleteNo ratings yet
- PowerDB Uninstall Guide PDFDocument4 pagesPowerDB Uninstall Guide PDFMarco C. PumaNo ratings yet
- Industrial Visit ReportDocument3 pagesIndustrial Visit ReportBarzeen Mehr AfareenNo ratings yet
- Applied Economics ReportDocument16 pagesApplied Economics ReportJoyce Ann Agdippa Barcelona100% (1)
- AbanDocument12 pagesAbanIsmar MorenoNo ratings yet