Download as pdf or txt
You might also like
- AHM 540 - TestsDocument67 pagesAHM 540 - Testspraveen1510No ratings yet
- MHA-FPX5006 - Assessment 1-1Document10 pagesMHA-FPX5006 - Assessment 1-1RuthNo ratings yet
- Saving Lives Averting CostsDocument79 pagesSaving Lives Averting CostsAbhishek DebNo ratings yet
- Mercer - Proposal RFP ResponseDocument46 pagesMercer - Proposal RFP ResponseAleeza KhanNo ratings yet
- Time To Surgery and Survival in Breast Cancer: Research Open AccessDocument8 pagesTime To Surgery and Survival in Breast Cancer: Research Open AccessTatianaPadillaNo ratings yet
- Dos 516 Radiation Safety PaperDocument4 pagesDos 516 Radiation Safety Paperapi-530270156No ratings yet
- Final Draft-Muna 1Document4 pagesFinal Draft-Muna 1api-693187588No ratings yet
- Radiology Aco Whitepaper 11-18-14Document9 pagesRadiology Aco Whitepaper 11-18-14api-271257796No ratings yet
- 3855 DownDocument16 pages3855 DownpakhadkikarNo ratings yet
- Wilms 09protocolDocument15 pagesWilms 09protocolSyed Ali Akbar BokhariNo ratings yet
- Safety EssayDocument4 pagesSafety Essayapi-329968843No ratings yet
- Recist 1Document11 pagesRecist 1Kelik WagiyantoNo ratings yet
- Radiation Oncology Incident Learning System (ROILS) Cast StudyDocument4 pagesRadiation Oncology Incident Learning System (ROILS) Cast Studyapi-481226212No ratings yet
- Principles of Cancer StagingDocument28 pagesPrinciples of Cancer StagingAnonymous PKE8zOXNo ratings yet
- Delays in Diagnosis and Bladder Cancer Mortality: NearlyDocument8 pagesDelays in Diagnosis and Bladder Cancer Mortality: NearlyMuhammad FaisalNo ratings yet
- Electronic Systems For Patients To Report and Manage Side Effects of Cancer Treatment: Systematic ReviewDocument27 pagesElectronic Systems For Patients To Report and Manage Side Effects of Cancer Treatment: Systematic ReviewValerie LascauxNo ratings yet
- Oncology ValueDocument6 pagesOncology ValueTom BiusoNo ratings yet
- Prostate 12protocol 3200Document22 pagesProstate 12protocol 3200mella garciaNo ratings yet
- Running Head: Microsystem Assessment 1Document17 pagesRunning Head: Microsystem Assessment 1api-354204098No ratings yet
- ASCO EOM Fact SheetDocument11 pagesASCO EOM Fact SheetTom BiusoNo ratings yet
- Research Open AccessDocument8 pagesResearch Open AccessAlexander GraystonNo ratings yet
- 018 Breast CancerDocument2 pages018 Breast Cancerjim912100% (1)
- Surgery JournalDocument7 pagesSurgery JournalJane Arian BerzabalNo ratings yet
- s12876 022 02492 7Document13 pagess12876 022 02492 7ppdsipd2019No ratings yet
- Prognostic Value of The Systemic Immune-Inflammation Index in Patients With Breast Cancer: A Meta-AnalysisDocument12 pagesPrognostic Value of The Systemic Immune-Inflammation Index in Patients With Breast Cancer: A Meta-AnalysisJuliana SanjayaNo ratings yet
- Radiation Oncology Patient Safety FinalDocument4 pagesRadiation Oncology Patient Safety Finalapi-645453685No ratings yet
- Principles Cancer StagingDocument28 pagesPrinciples Cancer Stagingcheatingw995No ratings yet
- Orp 3 CombDocument8 pagesOrp 3 CombControl de Equipos InternosNo ratings yet
- The Clinical Significance of Remnant Thyroid Tissue in Thyroidectomized Differentiated Thyroid Cancer Patients OnDocument9 pagesThe Clinical Significance of Remnant Thyroid Tissue in Thyroidectomized Differentiated Thyroid Cancer Patients Onarifudin_achmadNo ratings yet
- Saving Lives Averting CostsDocument79 pagesSaving Lives Averting CostsMedCR1987No ratings yet
- Bladder Post Neoadj ChemoTx Resection40644 - 2023 - Article - 632Document11 pagesBladder Post Neoadj ChemoTx Resection40644 - 2023 - Article - 632Mariana UsatiiNo ratings yet
- Acumen Medicare MedicaidDocument184 pagesAcumen Medicare MedicaidAgeNo ratings yet
- CAM ToolkitDocument81 pagesCAM ToolkitEdwin WijayaNo ratings yet
- RFP 10th Edition FINAL 1Document16 pagesRFP 10th Edition FINAL 1hafidisara05No ratings yet
- Radiation Oncology Incident Learning System Case StudyDocument4 pagesRadiation Oncology Incident Learning System Case Studyapi-527613255No ratings yet
- Alvarado ScoreDocument8 pagesAlvarado ScoreAkbar TabletNo ratings yet
- Roils 1Document4 pagesRoils 1api-574059920No ratings yet
- SSC SkinDocument16 pagesSSC SkinNandaNo ratings yet
- Radiation Planning Assistant - A Streamlined, Fully Automated Radiotherapy Treatment Planning SystemDocument9 pagesRadiation Planning Assistant - A Streamlined, Fully Automated Radiotherapy Treatment Planning Systemdrrajeshb77No ratings yet
- Tiroides ArticuloDocument9 pagesTiroides Articulojuan sebaastianNo ratings yet
- DSML PROJECT REPORt HarshitDocument6 pagesDSML PROJECT REPORt HarshitharshitsharmaindNo ratings yet
- Impact of The Affordable Care Act On Insurance Status of Patients Newly Diagnosed With Kaposi SarcomaDocument6 pagesImpact of The Affordable Care Act On Insurance Status of Patients Newly Diagnosed With Kaposi SarcomaAthenaeum Scientific PublishersNo ratings yet
- A Randomized Trial of Robot-Assisted Laparoscopic Radical CystectomyDocument2 pagesA Randomized Trial of Robot-Assisted Laparoscopic Radical CystectomyCarmePonsNo ratings yet
- 1Document10 pages1vivek15012004No ratings yet
- Artificial Intelligence and Machine Learning On Diagnosis and Classification of Hip Fracture: Systematic ReviewDocument13 pagesArtificial Intelligence and Machine Learning On Diagnosis and Classification of Hip Fracture: Systematic ReviewMEHDI JAHANIRADNo ratings yet
- Sensor WorkingDocument17 pagesSensor WorkingEngr Kashi YousafzaiNo ratings yet
- Jurnal DMDocument8 pagesJurnal DMMalisa LukmanNo ratings yet
- Radiation Oncologyinthe Eraof Big Dataand MLfor Precision MedicineDocument31 pagesRadiation Oncologyinthe Eraof Big Dataand MLfor Precision MedicinetourariNo ratings yet
- Radiation SafetyDocument3 pagesRadiation Safetyapi-484027891No ratings yet
- Research Proposal DaxelleDocument6 pagesResearch Proposal DaxellenkuepdisignerNo ratings yet
- Utilidad de Los Metodos de Segmentacion HepaticaDocument17 pagesUtilidad de Los Metodos de Segmentacion HepaticaJardeli MerinoNo ratings yet
- Birads Score For Mammographic Images: Parveen Jaseela Regina .O. MDocument8 pagesBirads Score For Mammographic Images: Parveen Jaseela Regina .O. MInternational Journal of computational Engineering research (IJCER)No ratings yet
- Radiation Oncology Incident Learning System (ROILS) Case StudyDocument3 pagesRadiation Oncology Incident Learning System (ROILS) Case Studyapi-450246598No ratings yet
- ABSTRACTDocument22 pagesABSTRACTPhalguni ShenoyNo ratings yet
- Convolutional Neural NetworksDocument28 pagesConvolutional Neural NetworksGOLDEN AGE FARMSNo ratings yet
- Report Adil'12Document6 pagesReport Adil'12adilhusain1710465482No ratings yet
- Time To Surgery and Breast Cancer Survival in The United StatesDocument68 pagesTime To Surgery and Breast Cancer Survival in The United StatesShiela BulosNo ratings yet
- Journal Presentation - BreastDocument55 pagesJournal Presentation - BreastShiela BulosNo ratings yet
- SRI ReportDocument7 pagesSRI ReportDANI DJNo ratings yet
- Ational Uality Orum: Population Health: Prevention ProjectDocument16 pagesAtional Uality Orum: Population Health: Prevention ProjectPiperNo ratings yet
- Ann Rev Balic Et Al FinalDocument14 pagesAnn Rev Balic Et Al FinalFreddy A. ManayayNo ratings yet
- Ref 4Document30 pagesRef 4Aashish KalikaNo ratings yet
- Minimal Residual Disease and Circulating Tumor Cells in Breast CancerFrom EverandMinimal Residual Disease and Circulating Tumor Cells in Breast CancerNo ratings yet
- Ptak 2021Document20 pagesPtak 2021Angel1331331No ratings yet
- Review of The Research Report 2011 0Document170 pagesReview of The Research Report 2011 0Angel1331331No ratings yet
- 1990 Perceived Temperamental Characteristics and Regulation of Physiological Stress. A Study of Wheezy BabiesDocument13 pages1990 Perceived Temperamental Characteristics and Regulation of Physiological Stress. A Study of Wheezy BabiesAngel1331331No ratings yet
- Vygotski, L. (2009) - El Desarrollo de Los Procesos Psicológicos SuperioresDocument230 pagesVygotski, L. (2009) - El Desarrollo de Los Procesos Psicológicos SuperioresAngel1331331No ratings yet
- Wage Type Request Form Overview 102011vs2Document2 pagesWage Type Request Form Overview 102011vs2Singh 10No ratings yet
- Niall Ferguson Is Full of Shit With No Friggin Facts To Back Up His BsDocument9 pagesNiall Ferguson Is Full of Shit With No Friggin Facts To Back Up His Bsmsf3153840% (5)
- Sbcasol Commrev 4b Insurance DigestsDocument59 pagesSbcasol Commrev 4b Insurance DigestsMariel MarielNo ratings yet
- Customer Information Sheet: Title Description Refer To Policy Clause Number Product Name Tata Aig Medicare Plus Top-UpDocument4 pagesCustomer Information Sheet: Title Description Refer To Policy Clause Number Product Name Tata Aig Medicare Plus Top-UpSankyBoy06No ratings yet
- Medicaid and Medicare Savings Program 65+ (New York Health Access)Document3 pagesMedicaid and Medicare Savings Program 65+ (New York Health Access)philip198No ratings yet
- 22-23 Employee Insurance Guide Liberty Assistance - Cat 1 (B)Document32 pages22-23 Employee Insurance Guide Liberty Assistance - Cat 1 (B)Nelson RichardNo ratings yet
- NTPC Emoulments & AllowancesDocument2 pagesNTPC Emoulments & AllowancesPrathamesh GangalNo ratings yet
- CSFLC SurveyDocument12 pagesCSFLC SurveyDebasish Pahi100% (1)
- ScriptDocument2 pagesScriptPaul jeffersonNo ratings yet
- Parent Medical CoverageDocument9 pagesParent Medical CoveragecampeonNo ratings yet
- Fortune Care v. AmorinDocument2 pagesFortune Care v. AmorinKaren Joy MasapolNo ratings yet
- Ethical Dilemma - Case Scenario PDFDocument4 pagesEthical Dilemma - Case Scenario PDFrohanNo ratings yet
- International Business Model Competition Booklet 2017Document34 pagesInternational Business Model Competition Booklet 2017Rollins Center at BYUNo ratings yet
- DOH AuditDocument25 pagesDOH AuditNews10NBC100% (1)
- HHS OIG - Offshore Outsourcing OEI-09-12-00530Document13 pagesHHS OIG - Offshore Outsourcing OEI-09-12-00530Michael BarbereNo ratings yet
- 2019 W-2 Gregorio MartinezDocument2 pages2019 W-2 Gregorio Martinezporhj perraNo ratings yet
- 15 S 16Document23 pages15 S 16Nick ReismanNo ratings yet
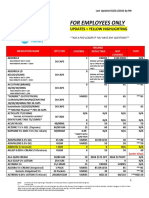
- Employee Only Pricing Sheet 02.11.22Document10 pagesEmployee Only Pricing Sheet 02.11.22rickyNo ratings yet
- 2007 Bookmatter DrugAndBiologicalDevelopmentDocument33 pages2007 Bookmatter DrugAndBiologicalDevelopmentGeorgiana CristeaNo ratings yet
- Obama Health Care Plan - Lyndon LaRoucheDocument16 pagesObama Health Care Plan - Lyndon LaRouchepaulpaul100% (2)
- The The Practice of Clinical Neuropsychology Studies On Neuropsychology Development and CognitionDocument392 pagesThe The Practice of Clinical Neuropsychology Studies On Neuropsychology Development and CognitionJelena Jovanovic100% (6)
- HSC Core 1: Health Priorities in AustraliaDocument33 pagesHSC Core 1: Health Priorities in AustraliaDivesh SinghNo ratings yet
- 'Who Will Care For Mom & Dad' Audit of Pa. Nursing Home StaffingDocument32 pages'Who Will Care For Mom & Dad' Audit of Pa. Nursing Home StaffingjmicekNo ratings yet
- Contemporary Nursing 8th Edition Cherry Test Bank 1Document212 pagesContemporary Nursing 8th Edition Cherry Test Bank 1mary011danielNo ratings yet
- COURSE ASSIGNMENTS Course AssignmentDocument4 pagesCOURSE ASSIGNMENTS Course AssignmentElly NuñezNo ratings yet
- TATA AIG Medicare - BrochureDocument2 pagesTATA AIG Medicare - Brochureonline accountNo ratings yet
- GeroDocument7 pagesGeroJehanie LukmanNo ratings yet