Download as pdf or txt
You might also like
- VMC Series Vertical Machining Centers: Operator'S ManualDocument176 pagesVMC Series Vertical Machining Centers: Operator'S Manualcafetux100% (2)
- Managing Risk of Complications at Femoral Vascular Access Sites in Percutaneous Coronary InterventionDocument16 pagesManaging Risk of Complications at Femoral Vascular Access Sites in Percutaneous Coronary InterventionydtrgnNo ratings yet
- Advances in Tunneled CVCDsDocument12 pagesAdvances in Tunneled CVCDsroykelumendekNo ratings yet
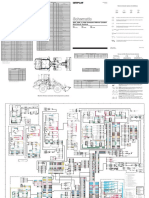
- 902, 906, & 908 Compact Wheel Loader Electrical System: Machine Harness Connector and Component LocationsDocument2 pages902, 906, & 908 Compact Wheel Loader Electrical System: Machine Harness Connector and Component Locationsait mimouneNo ratings yet
- Stress - The Different Kinds of StressDocument4 pagesStress - The Different Kinds of StressbogdanNo ratings yet
- Ultrasound-Guided Vascular AccessDocument15 pagesUltrasound-Guided Vascular AccessYulieth VanessaNo ratings yet
- Arterial Trauma During Central Venous Catheter Insertion: Case Series, Review and Proposed AlgorithmDocument8 pagesArterial Trauma During Central Venous Catheter Insertion: Case Series, Review and Proposed AlgorithmJuan Jose Velasquez GutierrezNo ratings yet
- Arterial Puncture and CannulationDocument19 pagesArterial Puncture and CannulationAzizah Rahawarin100% (1)
- Reconstructive Endovascular Treatment For Basilar Artery Trunk Aneurysms: Complications and Clinical and Angiography OutcomesDocument7 pagesReconstructive Endovascular Treatment For Basilar Artery Trunk Aneurysms: Complications and Clinical and Angiography OutcomesRafika Ayu NadiaNo ratings yet
- Role of and Indications For Bypass Surgery After Carotid Occlusion Surgery Study (COSS) ?Document9 pagesRole of and Indications For Bypass Surgery After Carotid Occlusion Surgery Study (COSS) ?osve91No ratings yet
- Article - Sequential Bypass Grafting On The Beating Heart - Blood Flow CharacteristicsDocument4 pagesArticle - Sequential Bypass Grafting On The Beating Heart - Blood Flow Characteristicsfluid_man_brazilNo ratings yet
- Complicated Course of Late Patient's Survival After The Classic Bentall Procedure With The Cabrol ShuntDocument3 pagesComplicated Course of Late Patient's Survival After The Classic Bentall Procedure With The Cabrol ShuntDonatas AustysNo ratings yet
- 11 Caring For Patients Post PCI Emil 2019Document3 pages11 Caring For Patients Post PCI Emil 2019ameliajamirusNo ratings yet
- Preparing A Patient For Cardiac Catheterization.4Document1 pagePreparing A Patient For Cardiac Catheterization.4Quality PmnhNo ratings yet
- Catheter Ablation of Intramural Outflow Tract Premature Ventricular Complexes - A Multicentre StudyDocument9 pagesCatheter Ablation of Intramural Outflow Tract Premature Ventricular Complexes - A Multicentre Studyahmed mostafaNo ratings yet
- White 2015Document6 pagesWhite 2015Muhammad AdithiaNo ratings yet
- Multimodal Tretment of Intracranial Aneurysm: A. Chiriac, I. Poeata, J. Baldauf, H.W. SchroederDocument10 pagesMultimodal Tretment of Intracranial Aneurysm: A. Chiriac, I. Poeata, J. Baldauf, H.W. SchroederApryana Damayanti ARNo ratings yet
- Guidelines For Vascular AccessDocument14 pagesGuidelines For Vascular AccessFikran SiddikNo ratings yet
- Central Venous Access - 2019 (Gen, Ind-Contr)Document6 pagesCentral Venous Access - 2019 (Gen, Ind-Contr)Carlos NoronaNo ratings yet
- Access For DialysisDocument7 pagesAccess For DialysisDeshan AdikariNo ratings yet
- Use of Intracoronary ImagingDocument11 pagesUse of Intracoronary ImagingPhyoNyeinChanNo ratings yet
- Recognizing, Preventing, and Troubleshooting Central-Line ComplicationsDocument7 pagesRecognizing, Preventing, and Troubleshooting Central-Line ComplicationsFauziaNo ratings yet
- Feliciano Trauma SurgeryDocument8 pagesFeliciano Trauma SurgeryMilitanisa ZamzaraNo ratings yet
- Anesthesia For Infrainguinal RevascularizationDocument23 pagesAnesthesia For Infrainguinal RevascularizationVignesh VenkatesanNo ratings yet
- Cis Self-Study Lesson Plan: Vascular and Cardiovascular Surgical InstrumentsDocument4 pagesCis Self-Study Lesson Plan: Vascular and Cardiovascular Surgical Instrumentsjerimiah_manzonNo ratings yet
- Williams, MC Dweck, MR Newby, DE - Coronary Computed TomographyDocument4 pagesWilliams, MC Dweck, MR Newby, DE - Coronary Computed TomographyMohammed AlkhairiNo ratings yet
- Okada and ShenoyDocument5 pagesOkada and Shenoyvaibhav vinkareNo ratings yet
- Placement of Vascular Access Catheters For Haemodialysis in The Innominate Vein: A Little-Used ApproachDocument4 pagesPlacement of Vascular Access Catheters For Haemodialysis in The Innominate Vein: A Little-Used ApproachCandátNo ratings yet
- Chaganti Joga Black Blood Imaging of IntracranialDocument8 pagesChaganti Joga Black Blood Imaging of IntracranialGUSTAVO ALEJANDRO AVERANGA TICONANo ratings yet
- Mischinger1999 PDFDocument5 pagesMischinger1999 PDFCiprian SebastianNo ratings yet
- Unclogging The Effects of The Angiojet Thrombectomy System On Kidney Function: A Case ReportDocument6 pagesUnclogging The Effects of The Angiojet Thrombectomy System On Kidney Function: A Case ReportBruno CoutinhoNo ratings yet
- Stroke Program Education May2022Document22 pagesStroke Program Education May2022Laura VelaNo ratings yet
- Stenosis AV Fistulas: Obobku Sayang SemangaaaatttttDocument17 pagesStenosis AV Fistulas: Obobku Sayang SemangaaaatttttraissaNo ratings yet
- Advpub tn.2019-0162 PDFDocument6 pagesAdvpub tn.2019-0162 PDFAlvhiesBiruUlfiahAzisNo ratings yet
- Aula SP 3-3 Caso 2Document13 pagesAula SP 3-3 Caso 2Wagner SoaresNo ratings yet
- IVUS OCT Guidance of IVL 2020 Mateissi, Mamas Et Al.Document7 pagesIVUS OCT Guidance of IVL 2020 Mateissi, Mamas Et Al.PraveenVeeraNo ratings yet
- Pseudo AneurysmDocument7 pagesPseudo AneurysmNgurah AndhikaNo ratings yet
- Ch 228 Gen i to Urinary TraumaDocument7 pagesCh 228 Gen i to Urinary TraumaDali KochalidzeNo ratings yet
- Pci 1Document24 pagesPci 1shejila c hNo ratings yet
- Strokeaha 117 019020Document4 pagesStrokeaha 117 019020camille chiranoNo ratings yet
- 489 FullDocument9 pages489 FullHellenaNo ratings yet
- Perioperative Management of Oral Antithrombotics in Dentistry and Oral Surgery: Part 2Document12 pagesPerioperative Management of Oral Antithrombotics in Dentistry and Oral Surgery: Part 2mariajnavarro2505No ratings yet
- Khairy 2017Document7 pagesKhairy 2017Beby Dwi Lestari BajryNo ratings yet
- Management of Blunt Liver Injury: What Is New?: J. Ward L. Alarcon A. B. PeitzmanDocument9 pagesManagement of Blunt Liver Injury: What Is New?: J. Ward L. Alarcon A. B. PeitzmanCamilla CristinaNo ratings yet
- (10920684 - Neurosurgical Focus) Transvenous Embolization of Brain Arteriovenous Malformations - A Review of Techniques, Indications, and OutcomesDocument7 pages(10920684 - Neurosurgical Focus) Transvenous Embolization of Brain Arteriovenous Malformations - A Review of Techniques, Indications, and Outcomesns52h22pvzNo ratings yet
- Current Percutaneous Recanalization of Coronary Chronic Total OcclusionDocument13 pagesCurrent Percutaneous Recanalization of Coronary Chronic Total OcclusionNader NURESNo ratings yet
- Trauma de CuelloDocument8 pagesTrauma de Cuellolilym.alvarez.lNo ratings yet
- Umana2019 PDFDocument4 pagesUmana2019 PDFIgor PiresNo ratings yet
- Anesthesia For Endovascular Therapy For Acute IschemicDocument36 pagesAnesthesia For Endovascular Therapy For Acute IschemicPietro DamoNo ratings yet
- Eau Guidelines On Urological Trauma: (Limited Text Update March 2017)Document18 pagesEau Guidelines On Urological Trauma: (Limited Text Update March 2017)Peri HidayatNo ratings yet
- Clinical Review - Full PDFDocument5 pagesClinical Review - Full PDFsitikhumaironiNo ratings yet
- Sullivan 2015Document11 pagesSullivan 2015Karoline Pascoal Ilidio PeruchiNo ratings yet
- Write Up WGL PressmeetDocument2 pagesWrite Up WGL Pressmeetvijju006No ratings yet
- Cardiovascular DisordersDocument15 pagesCardiovascular DisordersAzielle Joyce RosquetaNo ratings yet
- Anaesthesia For Off Pump Cardiac SurgeryDocument3 pagesAnaesthesia For Off Pump Cardiac SurgeryhkdawnwongNo ratings yet
- 7 24 1 PBDocument2 pages7 24 1 PBForminte MarianNo ratings yet
- Pseudoanuerysms Made EasyDocument15 pagesPseudoanuerysms Made EasyFooffscribdNo ratings yet
- 1067 FullDocument6 pages1067 FullJEAN GEMNo ratings yet
- Post PCNL Hemorrhage: Presenter: DR Sumit KabraDocument30 pagesPost PCNL Hemorrhage: Presenter: DR Sumit KabraGaurav GuptaNo ratings yet
- Bacaan PPT RebleedingDocument61 pagesBacaan PPT RebleedingseliNo ratings yet
- Feliciano 1989Document12 pagesFeliciano 1989Ciprian SebastianNo ratings yet
- Outcomes of Regular-Dose dŚĞƌĂƉĞƵƟĐ Barium Enema As An ŶŝƟĂů Treatment ForDocument6 pagesOutcomes of Regular-Dose dŚĞƌĂƉĞƵƟĐ Barium Enema As An ŶŝƟĂů Treatment ForElifastianiNo ratings yet
- Aortic RegurgitationFrom EverandAortic RegurgitationJan VojacekNo ratings yet
- Introduction To Privatisation and Liberalisation in India: by Anmol SharmaDocument10 pagesIntroduction To Privatisation and Liberalisation in India: by Anmol SharmaAnmol SharmaNo ratings yet
- Guidelines To An Informal LetterDocument3 pagesGuidelines To An Informal LetterNik Syahina0% (1)
- 5 MuscleDocument3 pages5 MuscleNicolePorsueloNo ratings yet
- Tech Mahindra Antonyms and QuestionsDocument27 pagesTech Mahindra Antonyms and QuestionsNehaNo ratings yet
- Light and ShadowDocument5 pagesLight and ShadowLisa Lipsett50% (2)
- STAAD - Pro Plates and Solid Elements (FAQ) - RAM - STAAD Wiki - RAM - STAAD - Bentley CommunitiesDocument15 pagesSTAAD - Pro Plates and Solid Elements (FAQ) - RAM - STAAD Wiki - RAM - STAAD - Bentley CommunitiesKamal RaoNo ratings yet
- The Blessed TrinityDocument2 pagesThe Blessed TrinityPatNo ratings yet
- 42pt250b Manual ServicioDocument63 pages42pt250b Manual ServicioLuis Carlos Bonilla AldanaNo ratings yet
- TAS Product Catalog 2020 01Document210 pagesTAS Product Catalog 2020 01ct0720054858No ratings yet
- Lesson 6 Solving Rational Equations and InequalitiesDocument80 pagesLesson 6 Solving Rational Equations and InequalitiesCarbon Copy0% (1)
- Pathophysiology Cardiac ArrestDocument1 pagePathophysiology Cardiac ArrestPATHOSHOPPE100% (2)
- Audi s6 2007 5.2l ManualDocument374 pagesAudi s6 2007 5.2l ManualMisael EspañaNo ratings yet
- eHYDRO SERIESDocument6 pageseHYDRO SERIESBanupriya BalasubramanianNo ratings yet
- Pdf&rendition 1Document61 pagesPdf&rendition 1Dulce DeNo ratings yet
- Avago HLCP j100, HDSP 48xxDocument7 pagesAvago HLCP j100, HDSP 48xxvelizarkoNo ratings yet
- MUSIC Quarter 3Document13 pagesMUSIC Quarter 3RaeNo ratings yet
- Soft Computing Module IDocument161 pagesSoft Computing Module INatarajanSubramanyamNo ratings yet
- Prepared by - Snehal ChintalaDocument78 pagesPrepared by - Snehal ChintalaSnehal ChintalaNo ratings yet
- Dynalene PG FG (Heat Transfer Fluid) : 1. Product and Company IdentificationDocument5 pagesDynalene PG FG (Heat Transfer Fluid) : 1. Product and Company IdentificationIvan DumontNo ratings yet
- Cold Agglutinin DiseaseDocument4 pagesCold Agglutinin Diseasenavneet21usNo ratings yet
- Aquaculture Aeration ModulesDocument7 pagesAquaculture Aeration ModulesecosafeNo ratings yet
- Detection Limits of Chemical Sensors: Applications and MisapplicationsDocument7 pagesDetection Limits of Chemical Sensors: Applications and MisapplicationsElbahi DjaalabNo ratings yet
- RABE - Sexual Imagery On The Phantasmagorical Castles at KhajurahoDocument30 pagesRABE - Sexual Imagery On The Phantasmagorical Castles at KhajurahoMarco PassavantiNo ratings yet
- Johor-Answer Physics P3-Trial SPM 2007Document6 pagesJohor-Answer Physics P3-Trial SPM 2007kamalharmozaNo ratings yet
- The Bromination of Acetone Lab ReportDocument4 pagesThe Bromination of Acetone Lab ReportSammy Njenga KhanNo ratings yet
- Polynomial FunctionDocument36 pagesPolynomial FunctionfaithreignNo ratings yet
- Homework 2 SolutionDocument5 pagesHomework 2 SolutiongretabunciNo ratings yet