
Electrocardiogram A5
Electrocardiogram A5
You might also like
- EKG Exam Study Guide PDFDocument31 pagesEKG Exam Study Guide PDFmeb100% (1)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- EKG Study GuideDocument45 pagesEKG Study GuideBrawner100% (7)
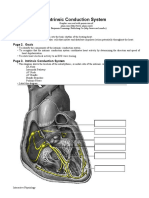
- Intrinsic Conduction System: Page 1. IntroductionDocument5 pagesIntrinsic Conduction System: Page 1. IntroductionUta Provinsiana SukmaraNo ratings yet
- ECG and Einthoven's Triangle Flashcards - QuizletDocument5 pagesECG and Einthoven's Triangle Flashcards - QuizletMr. DybalaNo ratings yet
- SPDX Electrocardiography-EcgDocument6 pagesSPDX Electrocardiography-Ecgdumppotato24No ratings yet
- ElectrocardiogramDocument2 pagesElectrocardiogramPAG-A, Daily Joy LNo ratings yet
- Lecture4 2Document34 pagesLecture4 2santhoshNo ratings yet
- The Cardiovascular System2Document2 pagesThe Cardiovascular System2John ExcaliburNo ratings yet
- N5 SampleDocument12 pagesN5 Sampleshaikhbakhtiyar3669No ratings yet
- 2300 - Module 5 - Basic Cardiovascular PathophysiologyDocument14 pages2300 - Module 5 - Basic Cardiovascular Pathophysiologymegan.abbinkNo ratings yet
- Electrocardiogram (ECG)Document53 pagesElectrocardiogram (ECG)eric100% (1)
- N5Document128 pagesN56qhx62pr42No ratings yet
- HEART SimplifiedDocument94 pagesHEART Simplifiedcloud kumoishNo ratings yet
- ECG Interpretation: Prepared byDocument16 pagesECG Interpretation: Prepared bypipoahmed51No ratings yet
- ECG Monitor and RhythmDocument9 pagesECG Monitor and Rhythmboxed juiceNo ratings yet
- Cardiovascular System - Electrical SystemDocument5 pagesCardiovascular System - Electrical SystemRashid DayaoNo ratings yet
- Student ProtocolDocument14 pagesStudent ProtocolLaura Camila Bermeo PeraltaNo ratings yet
- Clinical Demonstration: Topic: Electrocardiogram (ECG)Document24 pagesClinical Demonstration: Topic: Electrocardiogram (ECG)soniya josephNo ratings yet
- Assessing Heart and Neck VesselsDocument7 pagesAssessing Heart and Neck VesselsJae TyNo ratings yet
- The Heart BasicsDocument13 pagesThe Heart BasicsMegan DNo ratings yet
- Estimulação Transcutânea Não InvasivaDocument10 pagesEstimulação Transcutânea Não InvasivaMarcos AcioliNo ratings yet
- 321 Lecture ECGDocument38 pages321 Lecture ECGCea Mikee Mitch BartolomeNo ratings yet
- Dysrythmia Review For Pre TestDocument29 pagesDysrythmia Review For Pre TestGeena sekhonNo ratings yet
- 191 201 PDFDocument11 pages191 201 PDFDanyal ShabbirNo ratings yet
- Ecg InterpretationDocument82 pagesEcg InterpretationROMULO NU�EZ JR.No ratings yet
- Sample Transes 2Document11 pagesSample Transes 2Sophia SalamatNo ratings yet
- Fisika BioelektrikDocument50 pagesFisika BioelektrikFachriza EffendiNo ratings yet
- Unit 1Document29 pagesUnit 1SasikumarNo ratings yet
- Pacemaker Learning Package: Paula Nekic CNE Liverpool Hospital ICU January 2016Document46 pagesPacemaker Learning Package: Paula Nekic CNE Liverpool Hospital ICU January 2016Deepak BhatNo ratings yet
- DYSRHYTHMIAS AND CONDUCTION DISORDERS №1Document6 pagesDYSRHYTHMIAS AND CONDUCTION DISORDERS №1z8pwywrxf2No ratings yet
- DR Kupe - ECGDocument14 pagesDR Kupe - ECGIrfan ZiadNo ratings yet
- ECG EKG InterpretationDocument11 pagesECG EKG InterpretationGunma AkagiNo ratings yet
- Belajar Ekg YukDocument35 pagesBelajar Ekg Yukannisamuti10No ratings yet
- SB0024 Transport in Animals and Plant (DFN)Document80 pagesSB0024 Transport in Animals and Plant (DFN)jmyphjmrdnNo ratings yet
- (PDF.3) Management of Heart AttackDocument33 pages(PDF.3) Management of Heart AttackTheany Be SmilerNo ratings yet
- EKG - Premature Ventricular Contractions (PVCS)Document8 pagesEKG - Premature Ventricular Contractions (PVCS)SAM dabombdigNo ratings yet
- Cardiac Conduction System Power Point PresentationDocument30 pagesCardiac Conduction System Power Point PresentationAaya AdelNo ratings yet
- Cardiovascular SystemDocument74 pagesCardiovascular Systemاسامة محمد السيد رمضانNo ratings yet
- HPP Lec Cvs2Document4 pagesHPP Lec Cvs2carlo baculiNo ratings yet
- CV 2 PHDocument22 pagesCV 2 PHaya najemNo ratings yet
- Cardiac Ana & DxticsDocument3 pagesCardiac Ana & Dxticsjames garciaNo ratings yet
- 2 - Cardiac Electrical ActivityyytyyDocument31 pages2 - Cardiac Electrical ActivityyytyyTausif ChNo ratings yet
- Phys 4.1 CV Heart Electrical NOTESDocument5 pagesPhys 4.1 CV Heart Electrical NOTESEsther RaniNo ratings yet
- CardiovascularDocument16 pagesCardiovascularMilena VargasNo ratings yet
- ElectrocardiographyDocument11 pagesElectrocardiographysohan.ghosh23-25No ratings yet
- Basic ECGDocument14 pagesBasic ECGDexter TurlaNo ratings yet
- DYSRHYTMIASDocument13 pagesDYSRHYTMIASApple Mae AlmoniaNo ratings yet
- Understanding EKG's: Avant Healthcare ProfessionalsDocument20 pagesUnderstanding EKG's: Avant Healthcare ProfessionalsmarshaNo ratings yet
- Physiology Seminar: ElectrocardiographyDocument42 pagesPhysiology Seminar: ElectrocardiographyRajesh SharmaNo ratings yet
- Edenspiekermann Whitepaper Rethinking-Design-ThinkingDocument17 pagesEdenspiekermann Whitepaper Rethinking-Design-ThinkingnameNo ratings yet
- Cardiac Markers-It Is An Enzyme That Increases If You Have Cardiac Muscle Injury. We NeedDocument5 pagesCardiac Markers-It Is An Enzyme That Increases If You Have Cardiac Muscle Injury. We Needcamile buhanginNo ratings yet
- Sistem Konduksi Jantung (Pembekalan) - DR PUT&DrHARDocument32 pagesSistem Konduksi Jantung (Pembekalan) - DR PUT&DrHARNur FarinahNo ratings yet
- Electrical Conduction System of The HeartDocument27 pagesElectrical Conduction System of The HeartAnonymous gUjimJKNo ratings yet
- Physiology Worksheet Chapter Five: Cardiovascular SystemDocument2 pagesPhysiology Worksheet Chapter Five: Cardiovascular SystemTalya DannawiNo ratings yet
- Cardiac NursingDocument26 pagesCardiac Nursingjgcriste95% (20)
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- Inflammatory Disorders A5Document5 pagesInflammatory Disorders A5FrancheskaNo ratings yet
- Theories On Healthy Aging A5Document4 pagesTheories On Healthy Aging A5FrancheskaNo ratings yet
- Geriatric Nursing Introduction A5Document6 pagesGeriatric Nursing Introduction A5FrancheskaNo ratings yet
- Fluids and Electrolytes A5Document4 pagesFluids and Electrolytes A5FrancheskaNo ratings yet
- Cancer NursingDocument11 pagesCancer NursingFrancheskaNo ratings yet
- Fluids and Electrolytes A5Document70 pagesFluids and Electrolytes A5FrancheskaNo ratings yet
- Immune System DisordersDocument9 pagesImmune System DisordersFrancheskaNo ratings yet

































































Download as docx, pdf, or txt
You might also like
- EKG Exam Study Guide PDFDocument31 pagesEKG Exam Study Guide PDFmeb100% (1)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- EKG Study GuideDocument45 pagesEKG Study GuideBrawner100% (7)
- Intrinsic Conduction System: Page 1. IntroductionDocument5 pagesIntrinsic Conduction System: Page 1. IntroductionUta Provinsiana SukmaraNo ratings yet
- ECG and Einthoven's Triangle Flashcards - QuizletDocument5 pagesECG and Einthoven's Triangle Flashcards - QuizletMr. DybalaNo ratings yet
- SPDX Electrocardiography-EcgDocument6 pagesSPDX Electrocardiography-Ecgdumppotato24No ratings yet
- ElectrocardiogramDocument2 pagesElectrocardiogramPAG-A, Daily Joy LNo ratings yet
- Lecture4 2Document34 pagesLecture4 2santhoshNo ratings yet
- The Cardiovascular System2Document2 pagesThe Cardiovascular System2John ExcaliburNo ratings yet
- N5 SampleDocument12 pagesN5 Sampleshaikhbakhtiyar3669No ratings yet
- 2300 - Module 5 - Basic Cardiovascular PathophysiologyDocument14 pages2300 - Module 5 - Basic Cardiovascular Pathophysiologymegan.abbinkNo ratings yet
- Electrocardiogram (ECG)Document53 pagesElectrocardiogram (ECG)eric100% (1)
- N5Document128 pagesN56qhx62pr42No ratings yet
- HEART SimplifiedDocument94 pagesHEART Simplifiedcloud kumoishNo ratings yet
- ECG Interpretation: Prepared byDocument16 pagesECG Interpretation: Prepared bypipoahmed51No ratings yet
- ECG Monitor and RhythmDocument9 pagesECG Monitor and Rhythmboxed juiceNo ratings yet
- Cardiovascular System - Electrical SystemDocument5 pagesCardiovascular System - Electrical SystemRashid DayaoNo ratings yet
- Student ProtocolDocument14 pagesStudent ProtocolLaura Camila Bermeo PeraltaNo ratings yet
- Clinical Demonstration: Topic: Electrocardiogram (ECG)Document24 pagesClinical Demonstration: Topic: Electrocardiogram (ECG)soniya josephNo ratings yet
- Assessing Heart and Neck VesselsDocument7 pagesAssessing Heart and Neck VesselsJae TyNo ratings yet
- The Heart BasicsDocument13 pagesThe Heart BasicsMegan DNo ratings yet
- Estimulação Transcutânea Não InvasivaDocument10 pagesEstimulação Transcutânea Não InvasivaMarcos AcioliNo ratings yet
- 321 Lecture ECGDocument38 pages321 Lecture ECGCea Mikee Mitch BartolomeNo ratings yet
- Dysrythmia Review For Pre TestDocument29 pagesDysrythmia Review For Pre TestGeena sekhonNo ratings yet
- 191 201 PDFDocument11 pages191 201 PDFDanyal ShabbirNo ratings yet
- Ecg InterpretationDocument82 pagesEcg InterpretationROMULO NU�EZ JR.No ratings yet
- Sample Transes 2Document11 pagesSample Transes 2Sophia SalamatNo ratings yet
- Fisika BioelektrikDocument50 pagesFisika BioelektrikFachriza EffendiNo ratings yet
- Unit 1Document29 pagesUnit 1SasikumarNo ratings yet
- Pacemaker Learning Package: Paula Nekic CNE Liverpool Hospital ICU January 2016Document46 pagesPacemaker Learning Package: Paula Nekic CNE Liverpool Hospital ICU January 2016Deepak BhatNo ratings yet
- DYSRHYTHMIAS AND CONDUCTION DISORDERS №1Document6 pagesDYSRHYTHMIAS AND CONDUCTION DISORDERS №1z8pwywrxf2No ratings yet
- DR Kupe - ECGDocument14 pagesDR Kupe - ECGIrfan ZiadNo ratings yet
- ECG EKG InterpretationDocument11 pagesECG EKG InterpretationGunma AkagiNo ratings yet
- Belajar Ekg YukDocument35 pagesBelajar Ekg Yukannisamuti10No ratings yet
- SB0024 Transport in Animals and Plant (DFN)Document80 pagesSB0024 Transport in Animals and Plant (DFN)jmyphjmrdnNo ratings yet
- (PDF.3) Management of Heart AttackDocument33 pages(PDF.3) Management of Heart AttackTheany Be SmilerNo ratings yet
- EKG - Premature Ventricular Contractions (PVCS)Document8 pagesEKG - Premature Ventricular Contractions (PVCS)SAM dabombdigNo ratings yet
- Cardiac Conduction System Power Point PresentationDocument30 pagesCardiac Conduction System Power Point PresentationAaya AdelNo ratings yet
- Cardiovascular SystemDocument74 pagesCardiovascular Systemاسامة محمد السيد رمضانNo ratings yet
- HPP Lec Cvs2Document4 pagesHPP Lec Cvs2carlo baculiNo ratings yet
- CV 2 PHDocument22 pagesCV 2 PHaya najemNo ratings yet
- Cardiac Ana & DxticsDocument3 pagesCardiac Ana & Dxticsjames garciaNo ratings yet
- 2 - Cardiac Electrical ActivityyytyyDocument31 pages2 - Cardiac Electrical ActivityyytyyTausif ChNo ratings yet
- Phys 4.1 CV Heart Electrical NOTESDocument5 pagesPhys 4.1 CV Heart Electrical NOTESEsther RaniNo ratings yet
- CardiovascularDocument16 pagesCardiovascularMilena VargasNo ratings yet
- ElectrocardiographyDocument11 pagesElectrocardiographysohan.ghosh23-25No ratings yet
- Basic ECGDocument14 pagesBasic ECGDexter TurlaNo ratings yet
- DYSRHYTMIASDocument13 pagesDYSRHYTMIASApple Mae AlmoniaNo ratings yet
- Understanding EKG's: Avant Healthcare ProfessionalsDocument20 pagesUnderstanding EKG's: Avant Healthcare ProfessionalsmarshaNo ratings yet
- Physiology Seminar: ElectrocardiographyDocument42 pagesPhysiology Seminar: ElectrocardiographyRajesh SharmaNo ratings yet
- Edenspiekermann Whitepaper Rethinking-Design-ThinkingDocument17 pagesEdenspiekermann Whitepaper Rethinking-Design-ThinkingnameNo ratings yet
- Cardiac Markers-It Is An Enzyme That Increases If You Have Cardiac Muscle Injury. We NeedDocument5 pagesCardiac Markers-It Is An Enzyme That Increases If You Have Cardiac Muscle Injury. We Needcamile buhanginNo ratings yet
- Sistem Konduksi Jantung (Pembekalan) - DR PUT&DrHARDocument32 pagesSistem Konduksi Jantung (Pembekalan) - DR PUT&DrHARNur FarinahNo ratings yet
- Electrical Conduction System of The HeartDocument27 pagesElectrical Conduction System of The HeartAnonymous gUjimJKNo ratings yet
- Physiology Worksheet Chapter Five: Cardiovascular SystemDocument2 pagesPhysiology Worksheet Chapter Five: Cardiovascular SystemTalya DannawiNo ratings yet
- Cardiac NursingDocument26 pagesCardiac Nursingjgcriste95% (20)
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- Inflammatory Disorders A5Document5 pagesInflammatory Disorders A5FrancheskaNo ratings yet
- Theories On Healthy Aging A5Document4 pagesTheories On Healthy Aging A5FrancheskaNo ratings yet
- Geriatric Nursing Introduction A5Document6 pagesGeriatric Nursing Introduction A5FrancheskaNo ratings yet
- Fluids and Electrolytes A5Document4 pagesFluids and Electrolytes A5FrancheskaNo ratings yet
- Cancer NursingDocument11 pagesCancer NursingFrancheskaNo ratings yet
- Fluids and Electrolytes A5Document70 pagesFluids and Electrolytes A5FrancheskaNo ratings yet
- Immune System DisordersDocument9 pagesImmune System DisordersFrancheskaNo ratings yet