Download as pdf or txt
You might also like
- Research Paper: Alzheimer's DiseaseDocument13 pagesResearch Paper: Alzheimer's DiseaseABC Four CornersNo ratings yet
- Joint Mobilization Techniques For Sacroiliac Joint DysfunctionDocument17 pagesJoint Mobilization Techniques For Sacroiliac Joint Dysfunctiongaby_spy100% (3)
- PDFDocument422 pagesPDFThuRein WinNo ratings yet
- Dolor Postop, Ligamentos Cruzados, AmbulatorioDocument7 pagesDolor Postop, Ligamentos Cruzados, AmbulatorioChurrunchaNo ratings yet
- Jurnal AnestesiDocument7 pagesJurnal AnestesiJessica GraciaNo ratings yet
- 10 1016@j Jclinane 2016 02 020 PDFDocument7 pages10 1016@j Jclinane 2016 02 020 PDFabdulNo ratings yet
- Celecoxib & Ketoprofen For Pain ManagementDocument8 pagesCelecoxib & Ketoprofen For Pain ManagementUbaidillah AfiffNo ratings yet
- Jurnal 1Document5 pagesJurnal 1Muhammad AgussalimNo ratings yet
- 2264-Article Text-5024-4-10-20151024Document6 pages2264-Article Text-5024-4-10-20151024shivamNo ratings yet
- RossDocument12 pagesRossBasith. XNo ratings yet
- High Dose Dexamethasone in Low Pain Responders UndDocument9 pagesHigh Dose Dexamethasone in Low Pain Responders UndBhavani VuppuNo ratings yet
- Analgesic Effects and Adverse Reactions of LidocaiDocument6 pagesAnalgesic Effects and Adverse Reactions of Lidocaibrendastevany23No ratings yet
- Research - Articles With Proof of Indexation For Eligibility 1 - 1655459509710 - 7016032 - 18Document10 pagesResearch - Articles With Proof of Indexation For Eligibility 1 - 1655459509710 - 7016032 - 18jitendra vaghelaNo ratings yet
- Pain Cryotherapy in Single Visit RCTDocument6 pagesPain Cryotherapy in Single Visit RCTGauri AroraNo ratings yet
- Diclofenac Injectable DYLOJECT Drug Monograph FinalDocument13 pagesDiclofenac Injectable DYLOJECT Drug Monograph Finalmennaattia912No ratings yet
- Efficacy Lidocaine Endoscopic Submucosal DissectionDocument7 pagesEfficacy Lidocaine Endoscopic Submucosal DissectionAnonymous lSWQIQNo ratings yet
- Ijca 4 (2) 183-187Document5 pagesIjca 4 (2) 183-187Rabnawaz BanGashNo ratings yet
- JURNAL2Document15 pagesJURNAL2RialNo ratings yet
- 1 s2.0 S0883540318311537 MainDocument6 pages1 s2.0 S0883540318311537 MainSavNo ratings yet
- Journal Homepage: - : IntroductionDocument6 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Effect of Intraoperative Dexmedetomidine On Post-Craniotomy PainDocument9 pagesEffect of Intraoperative Dexmedetomidine On Post-Craniotomy PainIva SantikaNo ratings yet
- I0003 3006 64 2 80Document5 pagesI0003 3006 64 2 80angienayibeNo ratings yet
- Buharan MDDocument7 pagesBuharan MDNeha MasarkarNo ratings yet
- 10.1007@s00405 020 05801 6Document6 pages10.1007@s00405 020 05801 6Leonardo GuimelNo ratings yet
- Potasium DiclofenacDocument8 pagesPotasium DiclofenacDesy YeyenNo ratings yet
- Effect of Dexamethasone On The Duration of Interscalene Nerve Blocks With Ropivacaine or BupivacaineDocument8 pagesEffect of Dexamethasone On The Duration of Interscalene Nerve Blocks With Ropivacaine or BupivacaineIda KatarinaNo ratings yet
- Keywords:-Anaesthetics, Bupivacaine, Impaction, InferiorDocument8 pagesKeywords:-Anaesthetics, Bupivacaine, Impaction, InferiorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- KetamineDocument7 pagesKetamineAshiyan IrfanNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Article ComparisonOfIPACKAndPeriarticuDocument11 pagesArticle ComparisonOfIPACKAndPeriarticuRafly SuwandhiNo ratings yet
- Effect of Anti Inflammatory Regimen On Early.8Document9 pagesEffect of Anti Inflammatory Regimen On Early.8ririen refrina sariNo ratings yet
- Diclofenac From Administration To Adverse Effect A Mini-ReviewDocument5 pagesDiclofenac From Administration To Adverse Effect A Mini-ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jurnal 2Document9 pagesJurnal 2Muhammad AgussalimNo ratings yet
- Journal Homepage: - : IntroductionDocument4 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Analgesic Effects of Maxillary and Inferior AlveolDocument8 pagesAnalgesic Effects of Maxillary and Inferior Alveolmarina stroeNo ratings yet
- Analgesia en PTRDocument7 pagesAnalgesia en PTRGuillermo Ferrer BalartNo ratings yet
- Lavand'hommeDocument6 pagesLavand'hommeVan DaoNo ratings yet
- Bamgbose2005 Article EffectsOfCo-administeredDexameDocument6 pagesBamgbose2005 Article EffectsOfCo-administeredDexameDesy YeyenNo ratings yet
- Oh 2017Document8 pagesOh 2017翁嘉聰No ratings yet
- Lidocain and BuvipacainDocument6 pagesLidocain and BuvipacaintinahermantoNo ratings yet
- Books Binding BodyDocument71 pagesBooks Binding BodyToufique KhanNo ratings yet
- Impact of Intravenous Lidocaine Infusion On Postoperative Analgesia and Recovery From SurgeryDocument15 pagesImpact of Intravenous Lidocaine Infusion On Postoperative Analgesia and Recovery From SurgeryAbiChuelaNo ratings yet
- Comparison of The Effect of Intra-Articular, Periarticular, and Combined Injection of Analgesic On Pain Following Total Knee ArthroplastyDocument8 pagesComparison of The Effect of Intra-Articular, Periarticular, and Combined Injection of Analgesic On Pain Following Total Knee ArthroplastyFredivb1993hotmail.comNo ratings yet
- Which One Is More Effective For Analgesia in Infratentorial Craniotomy The Scalp Block or Local Anesthetic InfiltrationDocument6 pagesWhich One Is More Effective For Analgesia in Infratentorial Craniotomy The Scalp Block or Local Anesthetic InfiltrationEstivalis RiveraNo ratings yet
- Journal of Clinical Anesthesia: CorrespondenceDocument2 pagesJournal of Clinical Anesthesia: CorrespondenceSwati SinghNo ratings yet
- 与扑热息痛联用增效Document5 pages与扑热息痛联用增效zhuangemrysNo ratings yet
- Journal Homepage: - : IntroductionDocument10 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- 1 s2.0 S1743919120304568 MainDocument6 pages1 s2.0 S1743919120304568 MainIvanGómezNo ratings yet
- Atbaei 2010Document5 pagesAtbaei 2010sagita putriNo ratings yet
- Jcrs 48 1242Document6 pagesJcrs 48 1242ririen refrina sariNo ratings yet
- TNF TreatmentDocument9 pagesTNF Treatmentachal12No ratings yet
- Cataract JournalDocument9 pagesCataract Journalmonica_gallardo_24No ratings yet
- Sustained-Release Lidocaine Sheet For Pain FollowiDocument19 pagesSustained-Release Lidocaine Sheet For Pain FollowiArianny PerazaNo ratings yet
- 0 Aet484Document7 pages0 Aet484UsbahNo ratings yet
- EpinephrineDocument5 pagesEpinephrinesheynnaNo ratings yet
- Early Postoperative ComplicationsDocument6 pagesEarly Postoperative Complications49hr84j7spNo ratings yet
- Pain Control and Reduction of Opioid Use.3Document6 pagesPain Control and Reduction of Opioid Use.3Danty IndriastutyNo ratings yet
- The Prophylactic Effect of Rectal Diclofenac Versus Intravenous Pethidine On Postoperative Pain After Tonsillectomy in ChildrenDocument7 pagesThe Prophylactic Effect of Rectal Diclofenac Versus Intravenous Pethidine On Postoperative Pain After Tonsillectomy in ChildrenNi Komang Suryani DewiNo ratings yet
- Anasthesia 1Document7 pagesAnasthesia 1Rionald SitompulNo ratings yet
- EtoricoxibDocument15 pagesEtoricoxibSree BanNo ratings yet
- Steroids and Antiobiotics in TonsillectomyDocument9 pagesSteroids and Antiobiotics in TonsillectomyjulianasanjayaNo ratings yet
- Dexmedetomidine Vs Clonidine in IVRADocument5 pagesDexmedetomidine Vs Clonidine in IVRArandomaeiou7273No ratings yet
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYFrom EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYNo ratings yet
- 4 GoutDocument23 pages4 GoutMuhammad AgussalimNo ratings yet
- 2 Allergic DiseasesDocument27 pages2 Allergic DiseasesMuhammad AgussalimNo ratings yet
- Guidence Ipoi Operation SuccesDocument1 pageGuidence Ipoi Operation SuccesMuhammad AgussalimNo ratings yet
- Diabetes Prevention Knowledge and Perception of Risk AmongDocument7 pagesDiabetes Prevention Knowledge and Perception of Risk AmongMuhammad AgussalimNo ratings yet
- 5 CancerDocument57 pages5 CancerMuhammad AgussalimNo ratings yet
- Risk of Etylen GlicolDocument1 pageRisk of Etylen GlicolMuhammad AgussalimNo ratings yet
- Ethylene Glycol Toxicosis in Animals - Toxicology - MSD Veterinary ManualDocument6 pagesEthylene Glycol Toxicosis in Animals - Toxicology - MSD Veterinary ManualMuhammad AgussalimNo ratings yet
- Jurnal 2Document9 pagesJurnal 2Muhammad AgussalimNo ratings yet
- Jurnal 1Document5 pagesJurnal 1Muhammad AgussalimNo ratings yet
- Jurnal 3Document21 pagesJurnal 3Muhammad AgussalimNo ratings yet
- 1 s2.0 S2667147621000996 MainDocument5 pages1 s2.0 S2667147621000996 MainMuhammad AgussalimNo ratings yet
- Jurnal 5Document13 pagesJurnal 5Muhammad AgussalimNo ratings yet
- Jurnal 6Document9 pagesJurnal 6Muhammad AgussalimNo ratings yet
- Lipid Profile of Cholelithiasis Patients at Dr. Mohammad Hoesin Central General Hospital, PalembangDocument6 pagesLipid Profile of Cholelithiasis Patients at Dr. Mohammad Hoesin Central General Hospital, PalembangMuhammad AgussalimNo ratings yet
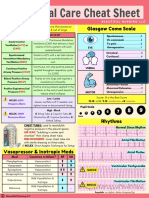
- Critical Care Cheat Sheet FreebieDocument2 pagesCritical Care Cheat Sheet FreebieJeshan Yanong Beltran100% (1)
- CTH Food and Safety Practices Research, FinalDocument12 pagesCTH Food and Safety Practices Research, FinalAlexis OrganisNo ratings yet
- A-Line Complication PDFDocument8 pagesA-Line Complication PDFaeagesNo ratings yet
- Oral Systemic ConnectionDocument37 pagesOral Systemic Connectionchrisdina puspita sari100% (1)
- Khan Et Al-2017-Phytotherapy ResearchDocument12 pagesKhan Et Al-2017-Phytotherapy ResearchsanthiyasandyNo ratings yet
- Electric Field Distribution in Biological Tissues For Various Electrode Configurations - A FEMLAB StudyDocument5 pagesElectric Field Distribution in Biological Tissues For Various Electrode Configurations - A FEMLAB StudyxlippyfingersNo ratings yet
- Case StudyDocument2 pagesCase Studyapi-244739669No ratings yet
- Uncertainty in MedicineDocument4 pagesUncertainty in MedicineShahidil SarilNo ratings yet
- Bahasa Inggris ReadingDocument5 pagesBahasa Inggris ReadingAgita Jeni INo ratings yet
- Parkinson'S Diseases (PD) : by Dr. Rommanah Azmi PM 013/09Document17 pagesParkinson'S Diseases (PD) : by Dr. Rommanah Azmi PM 013/09Rommanah AzmiNo ratings yet
- ISSTD Commentary.2013Document9 pagesISSTD Commentary.2013Bognár ErzsébetNo ratings yet
- Competency-Based Training in Basic Emergency Obstetric and Newborn Care (BEmONC) Improves Provider's Performance in TanzaniaDocument16 pagesCompetency-Based Training in Basic Emergency Obstetric and Newborn Care (BEmONC) Improves Provider's Performance in TanzaniaJhpiego100% (2)
- Journal of Medical Ethics and History of Medicine: Is Dissection Humane?Document4 pagesJournal of Medical Ethics and History of Medicine: Is Dissection Humane?Rahmat SatriadiNo ratings yet
- Performance Improvement Plan 2011-2012Document7 pagesPerformance Improvement Plan 2011-2012psynpNo ratings yet
- Hallmarks of Cancer: The Next Generation: ReviewDocument29 pagesHallmarks of Cancer: The Next Generation: Review122307403No ratings yet
- Liste Des Medicaments Classes en V e I Couverts Par Le Regime de Base23-08-2021Document178 pagesListe Des Medicaments Classes en V e I Couverts Par Le Regime de Base23-08-2021Elayeb MaherNo ratings yet
- Outcomes of Crowding in Emergency Departments A SyDocument10 pagesOutcomes of Crowding in Emergency Departments A SyPatricio Marcos CasazzaNo ratings yet
- Nurse Dialogues, Vocabulary and VideosDocument6 pagesNurse Dialogues, Vocabulary and VideosGastón LeeNo ratings yet
- Discontinuing An Intravenous InfusionDocument2 pagesDiscontinuing An Intravenous InfusionAgustin TrinaNo ratings yet
- Schedule JHDocument4 pagesSchedule JHlisa filiNo ratings yet
- Ringworm Bush (Akapulko) - Cassia AlataDocument21 pagesRingworm Bush (Akapulko) - Cassia AlataJingky SallicopNo ratings yet
- AidillahMayuda 22010113120001 Lap - KTI BAB VIIDocument42 pagesAidillahMayuda 22010113120001 Lap - KTI BAB VIINengsih SekarwangiNo ratings yet
- Rebecca M. Kluchin. "Sterilizing "Unfit" Women". Fit To Be Tied: Sterilization andDocument8 pagesRebecca M. Kluchin. "Sterilizing "Unfit" Women". Fit To Be Tied: Sterilization andapi-349123871No ratings yet
- M Sandamela Salivary Gland SandamelaDocument45 pagesM Sandamela Salivary Gland SandamelaRockson SamuelNo ratings yet
- Nursing Care in ECTDocument3 pagesNursing Care in ECTRawan KhateebNo ratings yet
- 2nd Peroxisome Metabolism 20760414Document56 pages2nd Peroxisome Metabolism 20760414Rawbeena RamtelNo ratings yet
- Vital Signs: Sheila Arelli Garcia-Safra, PRTP, MhpedDocument26 pagesVital Signs: Sheila Arelli Garcia-Safra, PRTP, MhpedSheila SafraNo ratings yet