Download as pdf or txt
You might also like
- Management of Post Facial Paralysis Synkinesis 1St Edition Babak Azizzadeh MD Facs Full ChapterDocument67 pagesManagement of Post Facial Paralysis Synkinesis 1St Edition Babak Azizzadeh MD Facs Full Chaptercatherine.green419100% (6)
- Types of Microscopes Comparison Chart 4 Linear Venn Edit Answer KeyDocument2 pagesTypes of Microscopes Comparison Chart 4 Linear Venn Edit Answer KeyKLRSantosNo ratings yet
- Septoplasty Endoscopic and Open TechniquesDocument8 pagesSeptoplasty Endoscopic and Open TechniquesКонстантин БелоусNo ratings yet
- Role of Transesophageal Echocardiography in Transcatheter Occlusion of Atrial Septal DefectsDocument17 pagesRole of Transesophageal Echocardiography in Transcatheter Occlusion of Atrial Septal DefectsriniambarwatiNo ratings yet
- Ear Related IssuesDocument27 pagesEar Related IssuesJessica Alexandria WuNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument35 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsmeenakshiNo ratings yet
- Paranasal Sinus AnatomyDocument35 pagesParanasal Sinus AnatomyGeorge DaviesNo ratings yet
- Effects of Various Dentofacial Orthopedic and Orthognathic Treatment Modalities On Pharyngeal AirwayDocument13 pagesEffects of Various Dentofacial Orthopedic and Orthognathic Treatment Modalities On Pharyngeal AirwaycdentistacesarmNo ratings yet
- Functional Anatomy and Physiology of Airway PDFDocument21 pagesFunctional Anatomy and Physiology of Airway PDFCarolina Sousa DiasNo ratings yet
- Paranasal Sinus Anatomy: What The Surgeon Needs To Know: June 2017Document36 pagesParanasal Sinus Anatomy: What The Surgeon Needs To Know: June 2017StancaMihaiAlexandruNo ratings yet
- Basic and Advanced Operative Techniques in Orthognatic SurgeryDocument23 pagesBasic and Advanced Operative Techniques in Orthognatic SurgeryAndrea Cárdenas SandovalNo ratings yet
- OroantfistlkitapblmDocument22 pagesOroantfistlkitapblmshehla khanNo ratings yet
- CT of The Paranasal Sinuses: A Pictorial Review of Normal Variants and Potential PitfallsDocument23 pagesCT of The Paranasal Sinuses: A Pictorial Review of Normal Variants and Potential PitfallsYodi SetiawanNo ratings yet
- Septumplastia 2Document9 pagesSeptumplastia 2vsberraondoNo ratings yet
- 000000Document27 pages000000drahmadelrawdyNo ratings yet
- Current Approaches in Orthognathic SurgeryDocument15 pagesCurrent Approaches in Orthognathic SurgerysrinivasanNo ratings yet
- Orientation of The Premaxilla in The Origin of Septal DeviationDocument5 pagesOrientation of The Premaxilla in The Origin of Septal Deviationnisrina hanifNo ratings yet
- Diagnosis Examination - Radiology Relevant Structures That May Compromise Patient HealthDocument31 pagesDiagnosis Examination - Radiology Relevant Structures That May Compromise Patient HealthCathleen LiNo ratings yet
- Atlas of Paranasal Sinus SurgeryDocument81 pagesAtlas of Paranasal Sinus SurgeryNemer Al-KhtoumNo ratings yet
- Vestibular Schwannomas Diagnosis and Surgical TreaDocument10 pagesVestibular Schwannomas Diagnosis and Surgical TreaTimothy CaldwellNo ratings yet
- Ecr2017 C-2117Document66 pagesEcr2017 C-2117Ezekiel ArtetaNo ratings yet
- Anatomy and Evaluation in RhinoplastyDocument20 pagesAnatomy and Evaluation in RhinoplastyLaureano FilhoNo ratings yet
- Airway Management in The Adult - Miller's Anesthesia 2009Document38 pagesAirway Management in The Adult - Miller's Anesthesia 2009UrgenciasCol FoamNo ratings yet
- CT Scan Sinus ParanasalDocument21 pagesCT Scan Sinus ParanasalDewi BoedhiyonoNo ratings yet
- Maxillofacial Fractures From Diagnosis To TreatmenDocument21 pagesMaxillofacial Fractures From Diagnosis To TreatmenChristine TanNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument25 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsKanchit SuwanswadNo ratings yet
- CT PNSDocument22 pagesCT PNSHany85No ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument15 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsRui FonteNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument21 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For Scientistsnevin shawky Prof. Oral SurgeryNo ratings yet
- Root Canal Morphology and AnatomyDocument10 pagesRoot Canal Morphology and Anatomylee suk moNo ratings yet
- Buccal Fat PadDocument21 pagesBuccal Fat PadPranave PNo ratings yet
- Internet Scientific PublicationsDocument12 pagesInternet Scientific PublicationsAnonymous h0DxuJTNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument15 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For Scientistsvenkatesh chowdaryNo ratings yet
- Maxillary Sinus in Dental Implantology PDFDocument27 pagesMaxillary Sinus in Dental Implantology PDFAlejandro MejiaNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument18 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsAfnan MoeNo ratings yet
- SINONASAL Pres TariDocument127 pagesSINONASAL Pres TariPradhana FwNo ratings yet
- Papadopoulos15 5Document28 pagesPapadopoulos15 5Ellizabeth LilantiNo ratings yet
- Discovering Middle Ear Anatomy by Transcanal Endoscopic Ear Surgery: A Dissection ManualDocument8 pagesDiscovering Middle Ear Anatomy by Transcanal Endoscopic Ear Surgery: A Dissection ManualGuillermo Castro ContardoNo ratings yet
- Principles of Anesthesia and Airway Management in Head and Neck Surgery - IntechOpenDocument29 pagesPrinciples of Anesthesia and Airway Management in Head and Neck Surgery - IntechOpenClarithq LengguNo ratings yet
- The Preoperative Sinus CT: Avoiding A "Close" Call With Surgical ComplicationDocument28 pagesThe Preoperative Sinus CT: Avoiding A "Close" Call With Surgical ComplicationArief FakhrizalNo ratings yet
- MGRUniv UGMar07Document32 pagesMGRUniv UGMar07Dr. T. BalasubramanianNo ratings yet
- Airway and Anesthetic Management of The Traumatized PatientDocument126 pagesAirway and Anesthetic Management of The Traumatized PatientdanocprexoidNo ratings yet
- The Case For Environmental Etiology of Malocclusion in Modern Civilizations-Airway Morphology and Facial GrowthDocument26 pagesThe Case For Environmental Etiology of Malocclusion in Modern Civilizations-Airway Morphology and Facial GrowthMoises Adriano Pulido GuimarãesNo ratings yet
- 16 Clinically Significant Variation of Paranasal Sinuses On CT ScanDocument6 pages16 Clinically Significant Variation of Paranasal Sinuses On CT ScanAjeng Salsabila PawestriNo ratings yet
- Cephalometric Evaluation and Measurement of The Upper Airway PDFDocument13 pagesCephalometric Evaluation and Measurement of The Upper Airway PDFSoe San KyawNo ratings yet
- Radiologic Evaluation, Principles of Management, Treatment Modalities and Complications of Orofacial InfectionsDocument15 pagesRadiologic Evaluation, Principles of Management, Treatment Modalities and Complications of Orofacial InfectionsAndrés Faúndez TeránNo ratings yet
- Upper Nasal AirwayDocument23 pagesUpper Nasal AirwayKapil ThakerNo ratings yet
- Chapterpdf Download635476105037 4Document20 pagesChapterpdf Download635476105037 4Abhishek JhaNo ratings yet
- Otoplasty For The Protruded EarDocument8 pagesOtoplasty For The Protruded EarroyvillafrancaNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument19 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsFlaviu Ionuț FaurNo ratings yet
- Anatomy and Physiology of The Maxillary Sinus: Harold A. Dehaven, JRDocument8 pagesAnatomy and Physiology of The Maxillary Sinus: Harold A. Dehaven, JRkhanhlinhNo ratings yet
- Antrochoanal Polyp in Pediatric Age Group PDFDocument5 pagesAntrochoanal Polyp in Pediatric Age Group PDFCut Nanda FitriNo ratings yet
- Considerations For The Spread Od Odontogenic Infections - Diagnosis Ans TreatmentDocument19 pagesConsiderations For The Spread Od Odontogenic Infections - Diagnosis Ans TreatmentAndrés Faúndez TeránNo ratings yet
- Nasal ObstructionDocument6 pagesNasal Obstructionjoal510No ratings yet
- HN9 Pharynx 03Document12 pagesHN9 Pharynx 03Farhan HasbiNo ratings yet
- Cannula Versus Needle in Medical Rhinoplasty - The Nose KnowsDocument24 pagesCannula Versus Needle in Medical Rhinoplasty - The Nose KnowsKerlida SantosNo ratings yet
- Trans-Septal Suture Method Versus Intranasal Silicone Splint in SeptoplastyDocument7 pagesTrans-Septal Suture Method Versus Intranasal Silicone Splint in SeptoplastyInternational Jpurnal Of Technical Research And ApplicationsNo ratings yet
- Planning and Sizing With OsiriXHorosDocument23 pagesPlanning and Sizing With OsiriXHorosJanineNo ratings yet
- Three-Dimensional Analysis of The Airway With Cone-Beam Computed TomographyDocument9 pagesThree-Dimensional Analysis of The Airway With Cone-Beam Computed TomographySoe San KyawNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument18 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For Scientistsnurul indah shalsabilaNo ratings yet
- CBCT Variants of Sinonasal Cavity What ODocument8 pagesCBCT Variants of Sinonasal Cavity What Oerik albarranNo ratings yet
- Skin Aging Fitz 9Document13 pagesSkin Aging Fitz 9Jhauharina RfNo ratings yet
- Understanding Nutrition 13th Edition Whitney Test Bank DownloadDocument18 pagesUnderstanding Nutrition 13th Edition Whitney Test Bank DownloadMichael Lozano100% (19)
- IIB Sant Pau 2020 WebDocument336 pagesIIB Sant Pau 2020 WebAinhoa GaNo ratings yet
- VPH 83.43 Rev.1Document60 pagesVPH 83.43 Rev.1jubatus.libroNo ratings yet
- Choosing The Raw Materials For FPJ: Agricultural Training Institute Managing Editor and Layout Artist EditorsDocument2 pagesChoosing The Raw Materials For FPJ: Agricultural Training Institute Managing Editor and Layout Artist EditorsRONALD PACOLNo ratings yet
- Umbilical Cord Prolapse: Green-Top Guideline No. 50Document13 pagesUmbilical Cord Prolapse: Green-Top Guideline No. 50Nurul Aimi Abdul RahmanNo ratings yet
- Determination of Ibuprofen and Paraben in Pharmaceutical Formulations Using Flowinjection and Derivative SpectrophotometryDocument2 pagesDetermination of Ibuprofen and Paraben in Pharmaceutical Formulations Using Flowinjection and Derivative Spectrophotometrycamelia_ioana_14No ratings yet
- Teal Sheets Addendum 02 - 2008Document2 pagesTeal Sheets Addendum 02 - 2008joséNo ratings yet
- Anticancer DrugsDocument6 pagesAnticancer DrugsmidhunNo ratings yet
- Effectiveness of Rhizobium Strains On Faba Bean Vicia Fabae L at Gumer District Highland Area of Southern EthiopiaDocument6 pagesEffectiveness of Rhizobium Strains On Faba Bean Vicia Fabae L at Gumer District Highland Area of Southern EthiopiaTarekegn TeferaNo ratings yet
- 8725-300 Psa Xs Accubind Elisa Rev 0Document2 pages8725-300 Psa Xs Accubind Elisa Rev 0dr madhusudhan reddyNo ratings yet
- Introduction To Medical Mycology: by Prof Ashraf MOGAHEDDocument61 pagesIntroduction To Medical Mycology: by Prof Ashraf MOGAHEDlianazulak100% (2)
- Natural Regeneration: Don Minore Robert J. LaackeDocument26 pagesNatural Regeneration: Don Minore Robert J. LaackeAngela Marie AlducenteNo ratings yet
- Psychic DevelopmentDocument13 pagesPsychic DevelopmentCult of Amon Ra100% (2)
- Kidney Structure and FunctionDocument68 pagesKidney Structure and FunctionAsmara Syed100% (1)
- Advances in Prostaglandin, Leukotriene, and Other Bioactive Lipid ResearchDocument243 pagesAdvances in Prostaglandin, Leukotriene, and Other Bioactive Lipid ResearchCarmen PopaNo ratings yet
- Shilajit A Panacea For CancerDocument9 pagesShilajit A Panacea For CancerRakeshKumarNo ratings yet
- Case Study 7B For HS 103 Week 8Document7 pagesCase Study 7B For HS 103 Week 8Rijane Tabonoc OmlangNo ratings yet
- CLS Aipmt-15-16 XI Zoo Study-Package-1 SET-1 Chapter-2A PDFDocument16 pagesCLS Aipmt-15-16 XI Zoo Study-Package-1 SET-1 Chapter-2A PDFAnonymous Too8UuiNo ratings yet
- Lecture2 GranulopoiesisDocument9 pagesLecture2 GranulopoiesisAfifa Prima GittaNo ratings yet
- CVS 217 QaDocument125 pagesCVS 217 QaDoaa Zakaria AliNo ratings yet
- Pex 08 01Document4 pagesPex 08 01Rafi SalimNo ratings yet
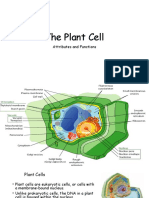
- The Plant CellDocument30 pagesThe Plant CellMichael GentilesNo ratings yet
- Speaking Test Avcn 1: Unit 1: Hospital StaffDocument5 pagesSpeaking Test Avcn 1: Unit 1: Hospital StaffHoàng Huy NguyễnNo ratings yet
- Streptococcus Pneumonae: Pathophysiology of CopdDocument1 pageStreptococcus Pneumonae: Pathophysiology of CopdDimpal ChoudharyNo ratings yet
- 2014 MBAA Chris White Yeast ManagementDocument30 pages2014 MBAA Chris White Yeast ManagementAdrián LampazziNo ratings yet
- HomeostasisDocument3 pagesHomeostasisAffie SaikolNo ratings yet
- Blank2021 Article MarkerAllergensInHymenopteraVeDocument13 pagesBlank2021 Article MarkerAllergensInHymenopteraVeAna-Maria DuMiNo ratings yet