Download as pdf or txt
You might also like
- RX-900-4 Parts Manual Rev. P SN 179 PDFDocument268 pagesRX-900-4 Parts Manual Rev. P SN 179 PDFoleg-spb80% (5)
- PNSG Table - LDocument17 pagesPNSG Table - Lapi-457773521No ratings yet
- Staff Emotional Intelligence ReportDocument4 pagesStaff Emotional Intelligence Reporttanveer ahmedNo ratings yet
- DSEP100 Operators ManualDocument42 pagesDSEP100 Operators ManualSon DoNo ratings yet
- NIH Public Access: Innovations That INSPIREDocument4 pagesNIH Public Access: Innovations That INSPIREshejila c hNo ratings yet
- Research Methodology in Dentistry: Part I - The Essentials and Relevance of ResearchDocument8 pagesResearch Methodology in Dentistry: Part I - The Essentials and Relevance of ResearchRomNo ratings yet
- PDF ImplementationLeanHealthCenterDocument24 pagesPDF ImplementationLeanHealthCenterpunishermoviesNo ratings yet
- Welp Et Al-2018-Journal of Clinical NursingDocument13 pagesWelp Et Al-2018-Journal of Clinical Nursinghendrihariadi12051988No ratings yet
- Transforming Leadership For Patient SatisfactionDocument4 pagesTransforming Leadership For Patient SatisfactionpietroNo ratings yet
- Best Practice - Journal ArticleDocument6 pagesBest Practice - Journal Articleutari dewiNo ratings yet
- Giving Feedback Effectively in The Clinical EnvironmentDocument5 pagesGiving Feedback Effectively in The Clinical EnvironmentMAurcioNo ratings yet
- International Journal of Nursing SciencesDocument8 pagesInternational Journal of Nursing SciencesjihaanNo ratings yet
- Healthcare 11 00545Document11 pagesHealthcare 11 00545Dina TrisnawatiNo ratings yet
- J of Nursing Scholarship - 2019 - Flynn - Understanding Determinants of Sustainability Through A Realist Investigation of ADocument10 pagesJ of Nursing Scholarship - 2019 - Flynn - Understanding Determinants of Sustainability Through A Realist Investigation of APaulo LemeNo ratings yet
- Sicometrik ICP IndonesiaDocument10 pagesSicometrik ICP IndonesiaUchi SuhermanNo ratings yet
- International Journal of Nursing Sciences: Yi Yang, Huaping Liu, Gwen D. SherwoodDocument9 pagesInternational Journal of Nursing Sciences: Yi Yang, Huaping Liu, Gwen D. SherwoodAbdulRahman MuthannaNo ratings yet
- h7d) KCD, 5bc$9zm-5Document29 pagesh7d) KCD, 5bc$9zm-5Kristel AnneNo ratings yet
- NCM 119 LM EndtermDocument10 pagesNCM 119 LM EndtermJmarie Brillantes PopiocoNo ratings yet
- Create A Learning Organization: Leadership'sDocument3 pagesCreate A Learning Organization: Leadership'sapi-3833460No ratings yet
- Research in Continuing Education Programme: C. Meribha Christy, V. HemavathyDocument4 pagesResearch in Continuing Education Programme: C. Meribha Christy, V. HemavathyRubina MasihNo ratings yet
- Effective Supervision in Clinical Practice Settings: A Literature ReviewDocument14 pagesEffective Supervision in Clinical Practice Settings: A Literature ReviewAmeng GosimNo ratings yet
- Quality Improvement by Review in Practical: Primary GuideDocument7 pagesQuality Improvement by Review in Practical: Primary GuideBruno Hudson CoutinhoNo ratings yet
- No33 Maximizingbenefitsofself-Assess GoodDocument8 pagesNo33 Maximizingbenefitsofself-Assess GoodShailendra KelaniNo ratings yet
- Niles J 6502 Assignment 1Document16 pagesNiles J 6502 Assignment 1api-597475939No ratings yet
- Organizational Resilience Cranfield Research ReportDocument54 pagesOrganizational Resilience Cranfield Research ReportJulio Armando FabazNo ratings yet
- Challenges in Implementing Innovations in Midwifery Practice An OverviewDocument3 pagesChallenges in Implementing Innovations in Midwifery Practice An OverviewEditor IJTSRDNo ratings yet
- Parand 2014 Sys Rev MGT BMJODocument17 pagesParand 2014 Sys Rev MGT BMJOAng Timotius Raymond AngkajayaNo ratings yet
- Sebok Syer 2018 Considering The Interdependence ofDocument11 pagesSebok Syer 2018 Considering The Interdependence ofYoliset RomeroNo ratings yet
- 4-Global Leadership in IPECP Research An Intro To Co-Creation of BestDocument8 pages4-Global Leadership in IPECP Research An Intro To Co-Creation of BestodetNo ratings yet
- Interprofessional Practice Education in Clinical Settings: Immersion Learning ActivitiesDocument48 pagesInterprofessional Practice Education in Clinical Settings: Immersion Learning ActivitiesShilla AnandaNo ratings yet
- Microsystems Culture Change A Refined Theory For Developing Person-Centred, Safe andDocument21 pagesMicrosystems Culture Change A Refined Theory For Developing Person-Centred, Safe andDiah PutriNo ratings yet
- Adv Post Graduate MGMT Program in Healthcare & Hospital Leadership 2023Document4 pagesAdv Post Graduate MGMT Program in Healthcare & Hospital Leadership 2023mushahid khanNo ratings yet
- Curriculum Development of Successful Intelligence Promoting For Nursing StudentsDocument5 pagesCurriculum Development of Successful Intelligence Promoting For Nursing StudentsApar SwaroopNo ratings yet
- Examining Psychological Capital of Optimism, Self-Efficacy and Self-Monitoring As Predictors of Attitude Towards Organizational ChangeDocument12 pagesExamining Psychological Capital of Optimism, Self-Efficacy and Self-Monitoring As Predictors of Attitude Towards Organizational ChangeSubramani A.KNo ratings yet
- PTJ 0416Document15 pagesPTJ 0416EemaNo ratings yet
- International Journal of Nursing StudiesDocument8 pagesInternational Journal of Nursing StudiesJos CanalesNo ratings yet
- Care 4 Supply PDFDocument8 pagesCare 4 Supply PDFMarcela TrujilloNo ratings yet
- Priddis 2017Document17 pagesPriddis 2017SheilaNo ratings yet
- Benefits of Semi-Structured InterviewsDocument8 pagesBenefits of Semi-Structured Interviewsopelob26No ratings yet
- What Is A Systematic Review?: Supported by Sanofi-AventisDocument8 pagesWhat Is A Systematic Review?: Supported by Sanofi-AventisAnggaraNo ratings yet
- Quality Improvement Project Proposal WorksheetDocument12 pagesQuality Improvement Project Proposal Worksheetapi-448506260No ratings yet
- EstudiosDocument6 pagesEstudiospatrickchoque84No ratings yet
- Case Report: A Tool For Clinical Reasoning and Reflection Using The InternationalDocument15 pagesCase Report: A Tool For Clinical Reasoning and Reflection Using The InternationalNishtha singhalNo ratings yet
- Gandes IPE S2 KeperawatanDocument31 pagesGandes IPE S2 KeperawatanPinkinNo ratings yet
- Nurse Manager CompetenciesDocument8 pagesNurse Manager Competenciessd pilar bangsaNo ratings yet
- AssessmentDocument9 pagesAssessmentdian maya puspitaNo ratings yet
- BJHM 226 229 CTME HalpernMcKimm 2009 SuperDocument5 pagesBJHM 226 229 CTME HalpernMcKimm 2009 SuperRajeev NepalNo ratings yet
- NCMB 311 LecDocument4 pagesNCMB 311 LecGian Carlo BenitoNo ratings yet
- Implementing Evidence Based Practice in ICUDocument26 pagesImplementing Evidence Based Practice in ICUSherlline Carillo-CasucianNo ratings yet
- Level 1 Framework-MatrixDocument23 pagesLevel 1 Framework-MatrixlouradelNo ratings yet
- Tital Page-MergedDocument22 pagesTital Page-Mergeddiscount composingNo ratings yet
- Using SBAR To Communicate Falls Risk and Management in Interprofessional Rehabilitation Teams PDFDocument54 pagesUsing SBAR To Communicate Falls Risk and Management in Interprofessional Rehabilitation Teams PDFmehara1920No ratings yet
- Using SBAR To Communicate Falls Risk and Management in Interprofessional Rehabilitation TeamsDocument54 pagesUsing SBAR To Communicate Falls Risk and Management in Interprofessional Rehabilitation Teamsmehara1920No ratings yet
- Ijmet 09 07 035Document10 pagesIjmet 09 07 035punishermoviesNo ratings yet
- The Kirkpatrick Model: A Useful Tool For Evaluating Training OutcomesDocument10 pagesThe Kirkpatrick Model: A Useful Tool For Evaluating Training OutcomesLucrecia Mendes da SilvaNo ratings yet
- Research in Social and Administrative Pharmacy 16 (2020) 25-32Document8 pagesResearch in Social and Administrative Pharmacy 16 (2020) 25-32School StuffNo ratings yet
- Performance Managementthrough PeopleDocument11 pagesPerformance Managementthrough PeopleRizan MohamedNo ratings yet
- Jurnal Inter5Document8 pagesJurnal Inter5Mhd FirdausNo ratings yet
- Republic of The Philippines City of Iriga City Health Office Government Center Sta. Cruz Sur, Iriga City, PhilippinesDocument7 pagesRepublic of The Philippines City of Iriga City Health Office Government Center Sta. Cruz Sur, Iriga City, PhilippinesRenee Mae GadilNo ratings yet
- Both Ed and AdminDocument12 pagesBoth Ed and Adminapi-384606877No ratings yet
- QI Merged With Semehal and Fikremariam Draft2Document22 pagesQI Merged With Semehal and Fikremariam Draft2radiopharmaceuticalsolutionsNo ratings yet
- Evaluation of a Dialogical Psychologically Informed Environment (PIE) Pilot: Addressing homelessness, re-offending, substance abuse, and mental illnessFrom EverandEvaluation of a Dialogical Psychologically Informed Environment (PIE) Pilot: Addressing homelessness, re-offending, substance abuse, and mental illnessNo ratings yet
- Clinical Research Associate - The Comprehensive Guide: Vanguard ProfessionalsFrom EverandClinical Research Associate - The Comprehensive Guide: Vanguard ProfessionalsNo ratings yet
- National Clinical Guidelines For Diagnosing Heart Failure in Primary Care - How Often Are They Followed and For Which PatientsDocument3 pagesNational Clinical Guidelines For Diagnosing Heart Failure in Primary Care - How Often Are They Followed and For Which PatientsomaNo ratings yet
- Better Communication, Better Quality Person-Centred Care - Supporting Primary Care in The Community With EconsultDocument6 pagesBetter Communication, Better Quality Person-Centred Care - Supporting Primary Care in The Community With EconsultomaNo ratings yet
- Reopening Shuttered Hospitals To Expand Surge Capacity - Surge ...Document266 pagesReopening Shuttered Hospitals To Expand Surge Capacity - Surge ...omaNo ratings yet
- Module 5 Publication Review ArticleDocument12 pagesModule 5 Publication Review ArticleomaNo ratings yet
- Columbia SraDocument1 pageColumbia SraomaNo ratings yet
- Quality of Primary Care in Low and Middle-Income Countries - New Evidence From Standardized Patients StudiesDocument7 pagesQuality of Primary Care in Low and Middle-Income Countries - New Evidence From Standardized Patients StudiesomaNo ratings yet
- Port Loko User RequirementsDocument8 pagesPort Loko User RequirementsDanNo ratings yet
- Citation CJ4 - Checklist Working TitleDocument3 pagesCitation CJ4 - Checklist Working TitlePhilippe MagnoNo ratings yet
- Soilmec SR-125 HIT Hydraulic Rotary Rig (April 2016)Document12 pagesSoilmec SR-125 HIT Hydraulic Rotary Rig (April 2016)sandycastleNo ratings yet
- J6-S9014 DatasheetDocument2 pagesJ6-S9014 DatasheetOreol100% (1)
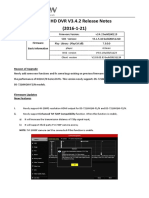
- Turbo HD DVR V3.4.2 Release Notes - ExternalDocument3 pagesTurbo HD DVR V3.4.2 Release Notes - Externalcrishtopher saenzNo ratings yet
- Econ487 000Document5 pagesEcon487 000021a604No ratings yet
- CCC.1-Circ.2-Rev.1 - Carriage of Bauxite Which May Liquefy (Secretariat)Document14 pagesCCC.1-Circ.2-Rev.1 - Carriage of Bauxite Which May Liquefy (Secretariat)Achwan SatyaNo ratings yet
- Teaching Vocabulrary SskillDocument463 pagesTeaching Vocabulrary SskillJoAnne K. ANo ratings yet
- AJP VMFWH 22142Document44 pagesAJP VMFWH 22142mrprem7768No ratings yet
- Garden City MovementDocument13 pagesGarden City MovementLenard O. MelgarNo ratings yet
- Advancements in Weft Knitting TechnologyDocument28 pagesAdvancements in Weft Knitting TechnologyAbhi Sheikh100% (1)
- 555 Timers With PSpice LabDocument6 pages555 Timers With PSpice LabHatem MOKHTARI0% (1)
- Whitman Resume AnnotatedDocument1 pageWhitman Resume Annotatedapi-664114983No ratings yet
- FILIPINO Calendar of ActivitiesDocument2 pagesFILIPINO Calendar of ActivitiesMariven NavarroNo ratings yet
- OralCommSHS q1 Week2 Models of Communication 1 RHEA ANN NAVILLADocument16 pagesOralCommSHS q1 Week2 Models of Communication 1 RHEA ANN NAVILLAJaspher Radoc AbelaNo ratings yet
- DCRM 6 Channel NewDocument9 pagesDCRM 6 Channel NewSayan ChatterjeeNo ratings yet
- KELAS XI SUMATIF (ULANGAN HARIAN) - HORTATORY EXPOSITION TEXT - DieditDocument5 pagesKELAS XI SUMATIF (ULANGAN HARIAN) - HORTATORY EXPOSITION TEXT - Dieditbagussetiawan76634No ratings yet
- Maths DPP PDFDocument4 pagesMaths DPP PDFSwarnava ChatterjeeNo ratings yet
- Hedland Scratch Band Tunebook (Dedicated To Colleen)Document219 pagesHedland Scratch Band Tunebook (Dedicated To Colleen)api-3836032100% (6)
- Fintech Adoption and Its Impact On Sustainability: Risk Benefit Analysis of An Emerging EconomyDocument32 pagesFintech Adoption and Its Impact On Sustainability: Risk Benefit Analysis of An Emerging EconomyAudit and Accounting ReviewNo ratings yet
- DocxDocument6 pagesDocxherrajohn100% (1)
- Digital Educational Technology in Improving Professional Auditory CompetenceDocument3 pagesDigital Educational Technology in Improving Professional Auditory CompetenceOpen Access JournalNo ratings yet
- Bosch Motorsport - 2009Document341 pagesBosch Motorsport - 2009Андрей ТатаренковNo ratings yet
- CMPR TextureDocument20 pagesCMPR TextureBejeweled LuigiGhostNo ratings yet
- EFuel100 Product Information BrochureDocument2 pagesEFuel100 Product Information BrochurekuttraNo ratings yet
- Profitability Analysis of Chilime Hydropower CompanyDocument10 pagesProfitability Analysis of Chilime Hydropower CompanySangita GhimireNo ratings yet
- Moving History Dancing Cultures A Dance History Re... - (An Anthropologist Looks at Ballet As A Form of Ethnic Dance)Document11 pagesMoving History Dancing Cultures A Dance History Re... - (An Anthropologist Looks at Ballet As A Form of Ethnic Dance)Vyenna BurlonNo ratings yet