Download as pdf or txt
You might also like
- Reflective Essay Draft 2Document5 pagesReflective Essay Draft 2Nancy Evans67% (3)
- Admas University Faculty of Business: Department of Accounting and Finance Course OutlineDocument6 pagesAdmas University Faculty of Business: Department of Accounting and Finance Course Outlineeyob astatkeNo ratings yet
- Social Studies SBA New and FinalDocument17 pagesSocial Studies SBA New and FinalsamoyaNo ratings yet
- Expressing Emotion in Interpersonal InteractionsDocument5 pagesExpressing Emotion in Interpersonal InteractionsAnish PandaNo ratings yet
- Sources of Nursing KnowledgeDocument13 pagesSources of Nursing KnowledgeVette Angelikka Dela CruzNo ratings yet
- Project Proposal Creba Scholars Feeding Program 2021Document3 pagesProject Proposal Creba Scholars Feeding Program 2021Angelica Perez100% (2)
- Millenium Development Goal No 4Document39 pagesMillenium Development Goal No 4preetie87No ratings yet
- Historical Perspective of Environmental HealthDocument11 pagesHistorical Perspective of Environmental HealthMatt67% (3)
- Palliative CareDocument25 pagesPalliative CareDwipa RozaliNo ratings yet
- HiAP PowerpointDocument21 pagesHiAP Powerpointjaypee pengNo ratings yet
- CMN 463 Lecture 2 Insurance Medicare and MedicaidDocument18 pagesCMN 463 Lecture 2 Insurance Medicare and MedicaidCarlos GuiterizNo ratings yet
- The Heath Care Delivery SystemDocument17 pagesThe Heath Care Delivery SystemAngelou RosalesNo ratings yet
- 9approaches To Public Health in IndiaDocument90 pages9approaches To Public Health in IndiaAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Nursing Care Delivery SystemDocument10 pagesNursing Care Delivery Systembardah wasalamahNo ratings yet
- The 10 Essential Public Health ServicesDocument38 pagesThe 10 Essential Public Health ServicesNaufal Faizul RafiNo ratings yet
- Importance of Understanding Your Community Powerpoint Presentation NSTP 2Document16 pagesImportance of Understanding Your Community Powerpoint Presentation NSTP 2Karen RasingNo ratings yet
- Disaster ManagementDocument42 pagesDisaster ManagementLoma Waghmare (Jadhav)No ratings yet
- Guidelines For CHPS ImplementationDocument16 pagesGuidelines For CHPS ImplementationErasmus Agongo100% (1)
- TFN DS 16 - LeiningerDocument31 pagesTFN DS 16 - LeiningerCatherine Martinez AvilaNo ratings yet
- Introduction of Public Health Nursing: Mr. Kailash NagarDocument37 pagesIntroduction of Public Health Nursing: Mr. Kailash NagarKailash NagarNo ratings yet
- CHN RevDocument134 pagesCHN RevGlenn Asuncion PagaduanNo ratings yet
- Che 238 Community Linkages 2023Document28 pagesChe 238 Community Linkages 2023Arum ComradeNo ratings yet
- Session 6: Advocacy Communication and Social Mobilization (ACSM)Document39 pagesSession 6: Advocacy Communication and Social Mobilization (ACSM)farajhiNo ratings yet
- The Nursing Process in The Care of The CommunityDocument96 pagesThe Nursing Process in The Care of The CommunityCzarina Aeri RollorataNo ratings yet
- History, Evolution & Classification of HospitalsDocument10 pagesHistory, Evolution & Classification of HospitalsAnonymous ibmeej9100% (1)
- Concept of Health CareDocument9 pagesConcept of Health CaredrnareshchauhanNo ratings yet
- 1 COMMUNITY HEALTH NURSING CONCEPTS AutosavedDocument65 pages1 COMMUNITY HEALTH NURSING CONCEPTS AutosavedAbdhanie PanontonganNo ratings yet
- National Health MissionDocument78 pagesNational Health MissionIndrajeev KumarNo ratings yet
- Cost EffectivenessDocument1 pageCost EffectivenessIswahyudi AlamsyahNo ratings yet
- Community Health NursingDocument94 pagesCommunity Health NursingKimTot OctavianoNo ratings yet
- Illness BehaviorDocument11 pagesIllness BehaviorRubelleMicahCagampangSapongNo ratings yet
- Community AssessmentDocument9 pagesCommunity Assessmentرانيا احمد عبد الكريمNo ratings yet
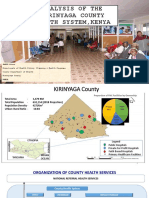
- Analysis of The Kirinyaga County Health System - Esbon - GakuuDocument18 pagesAnalysis of The Kirinyaga County Health System - Esbon - Gakuuesbon gakuu100% (1)
- Com Med CompiledDocument90 pagesCom Med Compiledbharati adhikariNo ratings yet
- Skill For Health PromotionDocument244 pagesSkill For Health PromotionElly MartinsNo ratings yet
- Concept of Health Disease and PreventionDocument33 pagesConcept of Health Disease and PreventionitdocNo ratings yet
- NCM 104 Lecture Chapter 2.1 Health-Care-Delivery-System 1Document25 pagesNCM 104 Lecture Chapter 2.1 Health-Care-Delivery-System 1Wilma Nierva BeraldeNo ratings yet
- Research in Palliative Care PresentationDocument20 pagesResearch in Palliative Care PresentationNICKY SAMBONo ratings yet
- Module Com DX Oct2020Document14 pagesModule Com DX Oct2020Marilyn PacantaraNo ratings yet
- Community Development Approaches To Health PromotionDocument35 pagesCommunity Development Approaches To Health PromotionOana Sorina AndronicNo ratings yet
- Role of NurseDocument24 pagesRole of NurseJohnykutty JosephNo ratings yet
- Descriptive Epidemiology Study Designs: Zziwa Swaibu (BEH, MPH MUK)Document47 pagesDescriptive Epidemiology Study Designs: Zziwa Swaibu (BEH, MPH MUK)Nina100% (1)
- The Community Client: Assessment Diagnosis: As andDocument43 pagesThe Community Client: Assessment Diagnosis: As andAbid HussainNo ratings yet
- Who Actions Towards SDGS: MR Sharad Adhikary Technical Officer Who IndonesiaDocument14 pagesWho Actions Towards SDGS: MR Sharad Adhikary Technical Officer Who IndonesiaReny Widya AstutiNo ratings yet
- Module 4 - Community Health AssessmentDocument8 pagesModule 4 - Community Health AssessmentSteffi100% (1)
- Module 2 PDFDocument24 pagesModule 2 PDFElla Nika FangonNo ratings yet
- Health System Management-3Document229 pagesHealth System Management-3Waltas KariukiNo ratings yet
- Social & Preventive MedicineDocument12 pagesSocial & Preventive Medicinedrsumanthmmc100% (1)
- Addiction PDFDocument14 pagesAddiction PDFJuwita Valen RamadhanniaNo ratings yet
- Chapter 24: Communication Communication and Nursing PracticeDocument4 pagesChapter 24: Communication Communication and Nursing PracticejoanneNo ratings yet
- Divine Word College of Legazpi College of Nursing: Franco L. Razon, Man, RNDocument91 pagesDivine Word College of Legazpi College of Nursing: Franco L. Razon, Man, RNFranco Razon100% (1)
- Demography 171220090930Document207 pagesDemography 171220090930Shankar GanigNo ratings yet
- Conference Program: 4th Asia Pacific Regional Conference On Health Impact Assessment (HIA), Seoul, South Korea, 9-11 October 2012Document56 pagesConference Program: 4th Asia Pacific Regional Conference On Health Impact Assessment (HIA), Seoul, South Korea, 9-11 October 2012ADB Health Sector GroupNo ratings yet
- Introduction To NutritionDocument19 pagesIntroduction To Nutritionseanne kskwkwkaNo ratings yet
- Chronic Non-communicable Diseases in Ghana: Multidisciplinary PerspectivesFrom EverandChronic Non-communicable Diseases in Ghana: Multidisciplinary PerspectivesNo ratings yet
- Module 1 Lesson 1Document37 pagesModule 1 Lesson 1John Dave V. Villarmente100% (1)
- Evidence-Based Practice: What'S in It For You?Document43 pagesEvidence-Based Practice: What'S in It For You?ApRil Anne Balanon100% (1)
- Scope & Concerns of Public HealthDocument56 pagesScope & Concerns of Public Healthraosaadi60% (5)
- 2023 - CHN - Topic 1Document55 pages2023 - CHN - Topic 1Mc Cobert AlipioNo ratings yet
- PUBLIC HEALTH SEM-II - Final 2020Document38 pagesPUBLIC HEALTH SEM-II - Final 2020Rajesh Kumar SahNo ratings yet
- Unit 2Document17 pagesUnit 2Shini SimonNo ratings yet
- Rehabilitation Services Group6Document62 pagesRehabilitation Services Group6Garima KwatraNo ratings yet
- Community Nursing Diagnosis N Health Community Planning (Compatibility Mode) - 2Document27 pagesCommunity Nursing Diagnosis N Health Community Planning (Compatibility Mode) - 2Egie Nugraha Fitriyan Apriyadi50% (2)
- TQM in HospitalDocument21 pagesTQM in HospitalAhmed AliNo ratings yet
- Public Health Midterm StudyguideDocument21 pagesPublic Health Midterm StudyguideJustin Lee100% (1)
- Oral Com 3rd Summative TestDocument4 pagesOral Com 3rd Summative TestRyan BustilloNo ratings yet
- Out of The Box QuestionsDocument4 pagesOut of The Box QuestionsRathva SameerNo ratings yet
- كراسة تسميع تالته ث هدية من بروفيشنالDocument20 pagesكراسة تسميع تالته ث هدية من بروفيشنالMohammad FathyNo ratings yet
- Cause and Effect of StressDocument3 pagesCause and Effect of StressThu Hà LêNo ratings yet
- Essay Class 03-NotesDocument2 pagesEssay Class 03-NotesDurga SinghNo ratings yet
- Assignment 02 of RWSDocument9 pagesAssignment 02 of RWSAmal NoorNo ratings yet
- Department of Education Department of Developmental ServicesDocument40 pagesDepartment of Education Department of Developmental ServicesJuan CabezasNo ratings yet
- Guidelines For Competence Assessment Updated August 2019Document13 pagesGuidelines For Competence Assessment Updated August 2019Danni MoniqueNo ratings yet
- How To Treat Yourself Well - A Comprehensive Guide To Self-Care and Personal WellbeingDocument3 pagesHow To Treat Yourself Well - A Comprehensive Guide To Self-Care and Personal WellbeingktzvdxocyaNo ratings yet
- Midterm Examination: Henri Fayol Identified 5 Functions of Management. According To Fayol (1916), ThisDocument12 pagesMidterm Examination: Henri Fayol Identified 5 Functions of Management. According To Fayol (1916), ThisPatrizzia Ann Rose OcbinaNo ratings yet
- ACT Case Formulation WorksheetDocument3 pagesACT Case Formulation Worksheetmergun919No ratings yet
- Community Health Nursing Chapter 10Document1 pageCommunity Health Nursing Chapter 10Audrie Allyson GabalesNo ratings yet
- Title: Is Money The Most Important Thing in Life?Document2 pagesTitle: Is Money The Most Important Thing in Life?Ticher InaNo ratings yet
- Developing Customer Loyalty in Healthcare: December 2019Document31 pagesDeveloping Customer Loyalty in Healthcare: December 2019Stacia AnastashaNo ratings yet
- Language of Research PG XWD AnsDocument1 pageLanguage of Research PG XWD AnsLourhenz AliyacyacNo ratings yet
- Patient-Centered Care TrainingDocument10 pagesPatient-Centered Care Trainingradomir.boskovicNo ratings yet
- Presentation 16Document12 pagesPresentation 16JeanelleNo ratings yet
- Discursive Essay Model Analysis: Task 1. Read The IELTS Writing Task Below. Then Order The Sentences To Make A CompleteDocument6 pagesDiscursive Essay Model Analysis: Task 1. Read The IELTS Writing Task Below. Then Order The Sentences To Make A CompleteNgoc YenNo ratings yet
- M-E For OVC Programs PresentationDocument32 pagesM-E For OVC Programs PresentationRichard KariukiNo ratings yet
- Perdev Leap Week 1 1st QuarterDocument8 pagesPerdev Leap Week 1 1st QuarterHarold LimboNo ratings yet
- B2 Word Formation WF010: Use The Word in Brackets To Form A New Word That Fits Into Each BlankDocument2 pagesB2 Word Formation WF010: Use The Word in Brackets To Form A New Word That Fits Into Each BlankSabrina Gabriela50% (2)
- V.1 060222 Materi Interpretation of Draw A Person TestDocument37 pagesV.1 060222 Materi Interpretation of Draw A Person TestAgus PratomoNo ratings yet
- N103 Lecture NotesDocument2 pagesN103 Lecture NotesAANo ratings yet
- The Validity of The Malay Brief COPE in Identifying Coping Strategies Among Adolescents in SecondayDocument5 pagesThe Validity of The Malay Brief COPE in Identifying Coping Strategies Among Adolescents in SecondayTiffany Johnson100% (1)