Download as pdf or txt
You might also like
- Break-Out Session 3b Winner PLC Salary Discrimination?: Kristin Fridgeirsdottir Data Analytics For LeadersDocument6 pagesBreak-Out Session 3b Winner PLC Salary Discrimination?: Kristin Fridgeirsdottir Data Analytics For LeadersEklilEklildzNo ratings yet
- Original Research Abstract AFCC ASMIHA 2019Document82 pagesOriginal Research Abstract AFCC ASMIHA 2019Program Studi Kardiologi100% (1)
- HMEF5113 Statistics For Educational Research PDFDocument216 pagesHMEF5113 Statistics For Educational Research PDFDalila Wahida91% (11)
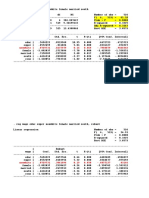
- Nonwhite - .0729731 .4437979 0.16 0.869 - .7988879 .9448342Document11 pagesNonwhite - .0729731 .4437979 0.16 0.869 - .7988879 .9448342TrầnMinhChâuNo ratings yet
- 865 FullDocument4 pages865 FullmugpijNo ratings yet
- Ischemic PreconditioningDocument14 pagesIschemic PreconditioninghariNo ratings yet
- Thrombectomy For Stroke at 6 To 16 Hours With Selection by Perfusion ImagingDocument11 pagesThrombectomy For Stroke at 6 To 16 Hours With Selection by Perfusion ImagingLia Ruby FariztaNo ratings yet
- Small Intracranial Aneurysms in The Barrow Ruptured Aneurysm Trial (BRAT)Document7 pagesSmall Intracranial Aneurysms in The Barrow Ruptured Aneurysm Trial (BRAT)Matheus TorresNo ratings yet
- (19330693 - Journal of Neurosurgery) Decompressive Hemicraniectomy - Predictors of Functional Outcome in Patients With Ischemic StrokeDocument7 pages(19330693 - Journal of Neurosurgery) Decompressive Hemicraniectomy - Predictors of Functional Outcome in Patients With Ischemic StrokeRandy Reina RiveroNo ratings yet
- Rory Hachamovitch, MD, MSC Sean W. Hayes, MD John D. Friedman, MD Ishac Cohen, PHD Daniel S. Berman, MDDocument8 pagesRory Hachamovitch, MD, MSC Sean W. Hayes, MD John D. Friedman, MD Ishac Cohen, PHD Daniel S. Berman, MDFarah SukmanaNo ratings yet
- Leukoaraiosis Is Associated With Poor Outcomes After Successful Recanalization For Large Vessel Occlusion StrokeDocument7 pagesLeukoaraiosis Is Associated With Poor Outcomes After Successful Recanalization For Large Vessel Occlusion StrokeLaura Valentina Huertas SaavedraNo ratings yet
- Zaidat Et Al 2023 Tesla Trial Rationale Protocol and DesignDocument9 pagesZaidat Et Al 2023 Tesla Trial Rationale Protocol and Designdvkhvbbds7No ratings yet
- Article - Surgical Management of Infective Endocarditis - Early Predictors of Short-Term Morbidity and MortalityDocument6 pagesArticle - Surgical Management of Infective Endocarditis - Early Predictors of Short-Term Morbidity and Mortalityfluid_man_brazilNo ratings yet
- Archivos - CT Angiography Followed by InvasiveDocument10 pagesArchivos - CT Angiography Followed by InvasiveGiselle LeonNo ratings yet
- Stroke Mimics VagalDocument12 pagesStroke Mimics VagalBrunaProençaNo ratings yet
- Sharma Et Al 2021 Frequency and Patterns of Brain Infarction in Patients With Embolic Stroke of Undetermined SourceDocument8 pagesSharma Et Al 2021 Frequency and Patterns of Brain Infarction in Patients With Embolic Stroke of Undetermined SourceSuryati HusinNo ratings yet
- Brain-X - 2023 - Li - Heart Brain Team Approach of Acute Myocardial Infarction Complicating Acute Stroke Evidencing TheDocument2 pagesBrain-X - 2023 - Li - Heart Brain Team Approach of Acute Myocardial Infarction Complicating Acute Stroke Evidencing TheBlackswannnNo ratings yet
- Medium Vessel Occlusion and Acute Ischemic Stroke: EditorialDocument3 pagesMedium Vessel Occlusion and Acute Ischemic Stroke: EditorialJihad AbdelgadirNo ratings yet
- 402 FullDocument7 pages402 Fullyohanes0gadiNo ratings yet
- 1726-Article Text-23983-2-10-20220330Document6 pages1726-Article Text-23983-2-10-20220330CL X-RAY IMAGESNo ratings yet
- NIHSS Cut-Point For Predicting Outcome in Supra-Vs Infratentorial Acute Ischemic StrokeDocument8 pagesNIHSS Cut-Point For Predicting Outcome in Supra-Vs Infratentorial Acute Ischemic StrokePutri NurdiyantiNo ratings yet
- 11 - Espectroscopia Desmiel Tumefactive - Ikeguchi2018Document8 pages11 - Espectroscopia Desmiel Tumefactive - Ikeguchi2018Henry DanielNo ratings yet
- Stenoza MitralaDocument7 pagesStenoza MitralaVerginia OnofreiNo ratings yet
- Bind Al 1996Document7 pagesBind Al 1996fira rifaNo ratings yet
- Accepted Manuscript: 10.1016/j.ijrobp.2017.01.201Document28 pagesAccepted Manuscript: 10.1016/j.ijrobp.2017.01.201Diana ArgüelloNo ratings yet
- Antiagregacion Vs Anticoagulacion en DiseccionDocument4 pagesAntiagregacion Vs Anticoagulacion en DiseccionCarlos Alberto CorredorNo ratings yet
- Jama Siegler 2024 Ed 240004 1706915651.01607Document2 pagesJama Siegler 2024 Ed 240004 1706915651.01607Srinivas PingaliNo ratings yet
- 708 FullDocument8 pages708 FullHidayadNo ratings yet
- 2022 - Long-Term Clinical Outcomes and Its Predictors Between the 1- and 2-Stent Strategy in Coronary Bifurcation Lesions ― A Baseline Clinical and Lesion Characteristic-Matched Analysis ―Document11 pages2022 - Long-Term Clinical Outcomes and Its Predictors Between the 1- and 2-Stent Strategy in Coronary Bifurcation Lesions ― A Baseline Clinical and Lesion Characteristic-Matched Analysis ―Qui Nguyen MinhNo ratings yet
- 12??Document7 pages12??pokharelriwaj82No ratings yet
- A Trial of Imaging Selection and Endovascular Treatment For Ischemic StrokeDocument10 pagesA Trial of Imaging Selection and Endovascular Treatment For Ischemic StrokelorenaNo ratings yet
- Yamga Et Al 2023 Optimized Risk Score To Predict Mortality in Patients With Cardiogenic Shock in The Cardiac IntensiveDocument24 pagesYamga Et Al 2023 Optimized Risk Score To Predict Mortality in Patients With Cardiogenic Shock in The Cardiac IntensivePPDS PDL JULI 23No ratings yet
- Articulo Cilliani 3ra HistoriaDocument6 pagesArticulo Cilliani 3ra HistoriaFabricio Nuñez de la CruzNo ratings yet
- 4 - 01-03-07 - J Neurosurg 2007 - Decompressive Hemicraniectomy in Malignant MCA InfarctionDocument7 pages4 - 01-03-07 - J Neurosurg 2007 - Decompressive Hemicraniectomy in Malignant MCA InfarctionThiago Scharth MontenegroNo ratings yet
- Safety of Middle Meningeal Artery Embolization For Treatment of Subdural Hematoma - A Nationwide Propensity Score Matched AnalysisDocument10 pagesSafety of Middle Meningeal Artery Embolization For Treatment of Subdural Hematoma - A Nationwide Propensity Score Matched AnalysisJUANNo ratings yet
- Sardar 2017Document10 pagesSardar 2017hafizaNo ratings yet
- Refining Angiographic Biomarkers of Revascularization: Improving Outcome Prediction After Intra-Arterial TherapyDocument5 pagesRefining Angiographic Biomarkers of Revascularization: Improving Outcome Prediction After Intra-Arterial TherapyDra. Carol Angélica Artigas GómezNo ratings yet
- CyberKnife Radiosurgery For Trigeminal NeuralgiaDocument7 pagesCyberKnife Radiosurgery For Trigeminal NeuralgiaAlfredo VelaNo ratings yet
- Strokeaha 114 005305Document7 pagesStrokeaha 114 005305Firdaous TouarsaNo ratings yet
- MainDocument11 pagesMainDella Alvita SNo ratings yet
- Emergent Carotid Stenting Plus Thrombectomy After Thrombolysis in Tandem Strokes - Analysis of The TITAN RegistryDocument3 pagesEmergent Carotid Stenting Plus Thrombectomy After Thrombolysis in Tandem Strokes - Analysis of The TITAN RegistryVictor M TorresNo ratings yet
- Trial of Endovascular Thrombectomy For Large Ischemic StrokesDocument13 pagesTrial of Endovascular Thrombectomy For Large Ischemic StrokesMABEL LUCERO OLARTE JURADONo ratings yet
- Plasma D-Dimer As A Biomarker For The Early Classification of Common Acute Ischemic Stroke Subtypes in IndonesiaDocument6 pagesPlasma D-Dimer As A Biomarker For The Early Classification of Common Acute Ischemic Stroke Subtypes in Indonesiaarifian wlpNo ratings yet
- Jurnal 11Document7 pagesJurnal 11Zella ZakyaNo ratings yet
- Impact of Statins On Cardiovascular Outcomes Following Coronary Artery Calcium ScoringDocument10 pagesImpact of Statins On Cardiovascular Outcomes Following Coronary Artery Calcium ScoringJNo ratings yet
- Keywords:-STS Score, MACE, CABGDocument6 pagesKeywords:-STS Score, MACE, CABGInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Endovascular Therapy For Cerebral Vein Thrombosis A Propensity-Matched Analysis of Anticoagulation in The Treatment of Cerebral Venous ThrombosisDocument7 pagesEndovascular Therapy For Cerebral Vein Thrombosis A Propensity-Matched Analysis of Anticoagulation in The Treatment of Cerebral Venous Thrombosisguohong huNo ratings yet
- Imagenes Multimodales en Valoracion de Grades VasosDocument51 pagesImagenes Multimodales en Valoracion de Grades VasosSebas MartinezNo ratings yet
- Of March 15, 2024. This Information Is Current As K.M. Schmainda, M.A. Prah, Z. Zhang, B.S. Snyder, S.DDocument9 pagesOf March 15, 2024. This Information Is Current As K.M. Schmainda, M.A. Prah, Z. Zhang, B.S. Snyder, S.DAhana MukherjeeNo ratings yet
- Low Diagnostic AngiographyDocument10 pagesLow Diagnostic AngiographyMei Lisa PutriNo ratings yet
- 42 Ijmrp 4 (3) 192-201Document10 pages42 Ijmrp 4 (3) 192-201SanjayNo ratings yet
- Management of Atypical Cranial Meningiomas Part 2Document8 pagesManagement of Atypical Cranial Meningiomas Part 2Edie DelgadoNo ratings yet
- Endovascular Management of Acute Ischaemic Stroke in NepaDocument2 pagesEndovascular Management of Acute Ischaemic Stroke in NepaJitendra PrasadNo ratings yet
- 1 s2.0 S0735109723055444 MainDocument10 pages1 s2.0 S0735109723055444 MainamadoNo ratings yet
- GPA Graded Prognostic Assessment Brain Metastasis RadiosurgeryDocument5 pagesGPA Graded Prognostic Assessment Brain Metastasis RadiosurgeryFNo ratings yet
- Make Clipping Great Again: Microsurgery For Cerebral Aneurysms by Dual-Trained NeurosurgeonsDocument8 pagesMake Clipping Great Again: Microsurgery For Cerebral Aneurysms by Dual-Trained NeurosurgeonsJohnson SimatupangNo ratings yet
- Ana 24309Document14 pagesAna 24309cah bagusNo ratings yet
- Thursday, October 10, 2013 4:10 - 5:10 Concurrent Session: TraumaDocument2 pagesThursday, October 10, 2013 4:10 - 5:10 Concurrent Session: TraumaPeko PekoNo ratings yet
- Lakunar and Outcome StrokeDocument11 pagesLakunar and Outcome StrokesitialimahNo ratings yet
- Endovascular Therapy For Acute Stroke With A Large Ischemic Region NEJMDocument21 pagesEndovascular Therapy For Acute Stroke With A Large Ischemic Region NEJMSubhashini KNo ratings yet
- Strokeaha 119 027356Document4 pagesStrokeaha 119 027356Orlin ZlatarskiNo ratings yet
- Outcome of Children With Severe Traumatic Brain Injury Who Are Treated With Decompressive CraniectomyDocument7 pagesOutcome of Children With Severe Traumatic Brain Injury Who Are Treated With Decompressive CraniectomyCarmen Juscamaita VegaNo ratings yet
- 10-1108 - Ijmf-12-2014-0187 (Jurnal Audit)Document21 pages10-1108 - Ijmf-12-2014-0187 (Jurnal Audit)indri retnoningtyasNo ratings yet
- Principles of Econometrics 4th Edition Hill Test BankDocument25 pagesPrinciples of Econometrics 4th Edition Hill Test BankEugeneMurraykspo100% (49)
- Datamining ss17Document57 pagesDatamining ss17Sun JavaNo ratings yet
- Comparison of Rigid Pavement Thickness Design SystemsDocument168 pagesComparison of Rigid Pavement Thickness Design Systemskamalnath100% (1)
- Chapter 4 Statistical Inference in Quality Control and ImprovementDocument106 pagesChapter 4 Statistical Inference in Quality Control and ImprovementEfraim John Hernandez100% (1)
- A Quantitative Assessment of Student Performance and Examination FormatDocument10 pagesA Quantitative Assessment of Student Performance and Examination FormatSherlyn Mae AlimanNo ratings yet
- SPE 30316 - PVT Correlations For Heavy and Extra Heavy Oils PDFDocument16 pagesSPE 30316 - PVT Correlations For Heavy and Extra Heavy Oils PDFLuis Alberto IzarraNo ratings yet
- Business Ethics Research PaperDocument14 pagesBusiness Ethics Research PaperMeann CubolNo ratings yet
- Fraud Prevention: Relevance To Religiosity and Spirituality in The WorkplaceDocument9 pagesFraud Prevention: Relevance To Religiosity and Spirituality in The WorkplaceJannah ZahraNo ratings yet
- ProblemSet422 23Document5 pagesProblemSet422 23lsanchez.ieu2021No ratings yet
- Risk Management 4Document20 pagesRisk Management 4Amin ShafanezhadNo ratings yet
- SPM - Indian StudyDocument7 pagesSPM - Indian StudyShera BahadurNo ratings yet
- ISSN (E) : 2222-6737/ISSN (P) : 2305-2147: Asian Economic and Financial Review, 2015, 5 (2) :218-228Document11 pagesISSN (E) : 2222-6737/ISSN (P) : 2305-2147: Asian Economic and Financial Review, 2015, 5 (2) :218-228hero birawanNo ratings yet
- Vector Autoregressions: Dr. Chen, Jo-HuiDocument33 pagesVector Autoregressions: Dr. Chen, Jo-HuiTajammul NaseemNo ratings yet
- Lab 6 AnswersDocument14 pagesLab 6 Answerswelcome martinNo ratings yet
- (Textbooks in Mathematics) Rodney X. Sturdivant, William P. Fox - Probability and Statistics For Engineering and The Sciences With Modeling Using R-CRC Press - Chapman & Hall (2022)Document429 pages(Textbooks in Mathematics) Rodney X. Sturdivant, William P. Fox - Probability and Statistics For Engineering and The Sciences With Modeling Using R-CRC Press - Chapman & Hall (2022)Adalberto SilvaNo ratings yet
- Handy Reference Sheet 2 - HRP 259 Calculation Formula's For Sample DataDocument15 pagesHandy Reference Sheet 2 - HRP 259 Calculation Formula's For Sample DataRosetta RennerNo ratings yet
- MAS202 Final ProjectDocument12 pagesMAS202 Final ProjectTran Huu Vinh QP3553No ratings yet
- TSExamples PDFDocument9 pagesTSExamples PDFKhalilNo ratings yet
- Does Urban Density Follow Centrality EmpDocument13 pagesDoes Urban Density Follow Centrality EmpFouad LeghribNo ratings yet
- Basic Marketing ResearchDocument34 pagesBasic Marketing ResearchSrinivasan ManavalanNo ratings yet
- An Assessment of Extension of Palli Daridro Bimochon Foundation (PDBF) Activities For Poverty Alleviation and Self Employment Project in BangladeshDocument10 pagesAn Assessment of Extension of Palli Daridro Bimochon Foundation (PDBF) Activities For Poverty Alleviation and Self Employment Project in BangladeshInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Managerial Economics (8522) LEVEL: MBA (3 Years) Assignment No. 1Document26 pagesManagerial Economics (8522) LEVEL: MBA (3 Years) Assignment No. 1saniaNo ratings yet
- BSC Statistics Syllabus CBCSDocument29 pagesBSC Statistics Syllabus CBCSpardha saradhi sekharNo ratings yet
- The Coefficient of Determinaton Exposed - HahnDocument4 pagesThe Coefficient of Determinaton Exposed - HahnAndre LanzerNo ratings yet
- Introduction To Regression and Analysis of Variance PDFDocument15 pagesIntroduction To Regression and Analysis of Variance PDFevan igorNo ratings yet