Download as pdf or txt
You might also like
- MycologyDocument129 pagesMycologyPriyanka Rajput100% (4)
- NAVLE Study Strategies Zuku ReviewDocument60 pagesNAVLE Study Strategies Zuku ReviewMohamed Omar90% (10)
- 8 Corynebacterium DiphtheriaeDocument5 pages8 Corynebacterium DiphtheriaeRami Moneem Oda SolaibiNo ratings yet
- General Characters of Nematodes: Cylindrical Cuticle. SeparateDocument18 pagesGeneral Characters of Nematodes: Cylindrical Cuticle. SeparateAyop KhNo ratings yet
- Small Coccobacilli: Pinpoint ColoniesDocument33 pagesSmall Coccobacilli: Pinpoint ColoniesPaul Avila SorianoNo ratings yet
- Mycology Practical 16 8 23Document29 pagesMycology Practical 16 8 23Dragon BogNo ratings yet
- Microb B1 CompileDocument13 pagesMicrob B1 CompileEarn chiNo ratings yet
- Cabison - Mycology ReviewerDocument10 pagesCabison - Mycology ReviewerPatricia Cabison100% (1)
- CoryneformDocument38 pagesCoryneformتجربة أولىNo ratings yet
- I. Corynebacterium: Non-Spore Forming Gram Positive BacilliDocument6 pagesI. Corynebacterium: Non-Spore Forming Gram Positive BacilliTob MoradosNo ratings yet
- Simulated No.1 General Rule:: ExceptDocument29 pagesSimulated No.1 General Rule:: ExceptJie FuentesNo ratings yet
- Anaerobic InfectionsDocument36 pagesAnaerobic Infectionsallenshanique1999No ratings yet
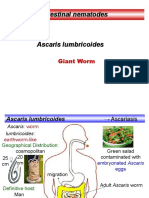
- Lab 4 Ascaris LumbricoidesDocument15 pagesLab 4 Ascaris LumbricoidesAAANo ratings yet
- BACTE m6Document9 pagesBACTE m6Gerald SorianoNo ratings yet
- Candidiasis: Sharada T Rajan Dept of Oral PathologyDocument70 pagesCandidiasis: Sharada T Rajan Dept of Oral PathologySharada GaneshNo ratings yet
- Food Testing Bacillus Species IbmaDocument22 pagesFood Testing Bacillus Species IbmaadiazcalidadNo ratings yet
- Parasites Life CycleDocument12 pagesParasites Life CyclebretonNo ratings yet
- Clinical Bacteriology Finals 2.0: Gram Positive BaciliDocument13 pagesClinical Bacteriology Finals 2.0: Gram Positive BaciliEzra LonodNo ratings yet
- A1 Methods To Identify BacteriaDocument6 pagesA1 Methods To Identify Bacteriahadigy1001No ratings yet
- Aerobic Gram PositiveDocument14 pagesAerobic Gram PositiveMickey mg100% (1)
- Family Vibrionaceae:: I. Vibrio SPPDocument8 pagesFamily Vibrionaceae:: I. Vibrio SPPpixholicNo ratings yet
- P3 Basil Gram (+) Rev2016Document50 pagesP3 Basil Gram (+) Rev2016AuliaNo ratings yet
- Gram Positive Bacili May StarDocument94 pagesGram Positive Bacili May StarJuliannaViktoriiaNo ratings yet
- MCQ QuestionsDocument9 pagesMCQ Questionshajra0325No ratings yet
- Candida Sinteza ImaginiDocument30 pagesCandida Sinteza ImaginiSandra PopescuNo ratings yet
- 11 - Anaerobic BacteriaDocument68 pages11 - Anaerobic BacteriaJohanna Kate DiestroNo ratings yet
- Nuôi Cáy Va Phan Lap Culture Reading and Bacterial IdentificationDocument56 pagesNuôi Cáy Va Phan Lap Culture Reading and Bacterial Identificationnguyen haNo ratings yet
- Practical Microbiology 2022Document71 pagesPractical Microbiology 2022Blendma AhmedNo ratings yet
- 11 NSF Gram + RodsDocument7 pages11 NSF Gram + RodsASECO LISHNo ratings yet
- NEMATODESDocument20 pagesNEMATODESLycah Jyde PechuancoNo ratings yet
- AntraxDocument14 pagesAntraxLigia OpreaNo ratings yet
- Bacte Notes 10 and 11Document10 pagesBacte Notes 10 and 11Reizel GaasNo ratings yet
- NEW - Clinical Mycology - Aliazas 2020 Ver-CompressedDocument84 pagesNEW - Clinical Mycology - Aliazas 2020 Ver-CompressedTrisha RomeoNo ratings yet
- 12 Aerobic Gram-Positive BacilliDocument68 pages12 Aerobic Gram-Positive BacilliClarence SantosNo ratings yet
- Enterobacteriaceae: - Prepared byDocument16 pagesEnterobacteriaceae: - Prepared byuwais sysNo ratings yet
- ProtozoaDocument78 pagesProtozoaChangkuoth Dak PuochNo ratings yet
- 1 Methods of Virol ResearchesDocument26 pages1 Methods of Virol ResearchesMann SarwanNo ratings yet
- Tables, Diagrams and SummariesDocument68 pagesTables, Diagrams and SummariesMicah JadeNo ratings yet
- ZVDVDZDDocument21 pagesZVDVDZDViorelci CizNo ratings yet
- THIRD OspeDocument133 pagesTHIRD OspeFree Style MusicNo ratings yet
- Overview of Gram - Negative Rods Enterobacteriaceae & Other Than EnterobacteriaceaeDocument51 pagesOverview of Gram - Negative Rods Enterobacteriaceae & Other Than EnterobacteriaceaeAudhrey BNo ratings yet
- Practical Parasitology 2008 Done by DR Ibrahim Samaha Medical Student Mansoura University EgyptDocument137 pagesPractical Parasitology 2008 Done by DR Ibrahim Samaha Medical Student Mansoura University EgyptNur DiyanaNo ratings yet
- (Perfringens Mobil Capsulat) : - Sporogenes, Novyi, Septicum, PERFRINGENS (Gangrena Gazoasa)Document9 pages(Perfringens Mobil Capsulat) : - Sporogenes, Novyi, Septicum, PERFRINGENS (Gangrena Gazoasa)Attila SzakacsNo ratings yet
- Diphteria, Leprae, Tetanus, Typhoid, Leptospirosis, MeningitisDocument57 pagesDiphteria, Leprae, Tetanus, Typhoid, Leptospirosis, MeningitisNur OctavianiNo ratings yet
- Microbiology FlashcardsDocument36 pagesMicrobiology FlashcardsKrisha Bernadette TillamanNo ratings yet
- Microbiology Bacteriological CultureDocument2 pagesMicrobiology Bacteriological CultureAlyssum JJNo ratings yet
- Introduction To Medical MycologyDocument31 pagesIntroduction To Medical MycologychiyeoncherryNo ratings yet
- Pre 1 MibrobiologyDocument3 pagesPre 1 MibrobiologyDeannise AnnNo ratings yet
- Campylobacter & Plesiomonas - Bacter ReportDocument55 pagesCampylobacter & Plesiomonas - Bacter ReportRona SalandoNo ratings yet
- Proteus& VibiroDocument21 pagesProteus& Vibirosajad abasNo ratings yet
- FinalDocument62 pagesFinalChristian AriasNo ratings yet
- Strongyloides Stercoralis: Faecal Like CylinderDocument18 pagesStrongyloides Stercoralis: Faecal Like CylinderAyop KhNo ratings yet
- MSS Lab 2022-2023Document19 pagesMSS Lab 2022-2023zaina.bookshopNo ratings yet
- Preg Test Vaginal SecretionsDocument43 pagesPreg Test Vaginal Secretionsepson printerNo ratings yet
- Opportunistic Pathogens MLS 109 CondensadaDocument4 pagesOpportunistic Pathogens MLS 109 Condensadajoseadreannes.pinedaNo ratings yet
- CC14 Edited LNB (Primary Check)Document78 pagesCC14 Edited LNB (Primary Check)redgravevarienNo ratings yet
- Bacte Day 2Document24 pagesBacte Day 2Jadey InfanteNo ratings yet
- Corynebacterium and Other Non-spore-Forming Gram-Positive RodsDocument3 pagesCorynebacterium and Other Non-spore-Forming Gram-Positive RodsYelai CarveroNo ratings yet
- UrineDocument42 pagesUrineحسين علاوي طاميNo ratings yet
- Fungi 1Document51 pagesFungi 1Azman YaacubNo ratings yet
- Cryptococcal Antigen Latex Agglutination Test JOSEPHDocument14 pagesCryptococcal Antigen Latex Agglutination Test JOSEPHchocoholic potchiNo ratings yet
- Peigon Nuisance /problemsDocument6 pagesPeigon Nuisance /problemsVidya DufareNo ratings yet
- The Evidence Supporting The Revised EORTC-MSGERC Definitions For Invasive Fungal InfectionsDocument2 pagesThe Evidence Supporting The Revised EORTC-MSGERC Definitions For Invasive Fungal Infectionsgwyneth.green.512No ratings yet
- Poultry Production AssignmentDocument9 pagesPoultry Production AssignmentAyele AsefaNo ratings yet
- Pharmaceutical Microbiology and Parasitology (PHMP211)Document59 pagesPharmaceutical Microbiology and Parasitology (PHMP211)Crisamor Rose Pareja ClarisaNo ratings yet
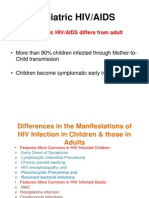
- Paediatric HIV Infection by DR A.K.Gupta, Additional Project Director, Delhi State AIDS Control SocietyDocument88 pagesPaediatric HIV Infection by DR A.K.Gupta, Additional Project Director, Delhi State AIDS Control Societydr.a.k.gupta6924No ratings yet
- Perfect 2015Document6 pagesPerfect 2015windaNo ratings yet
- Swaziland SOPs 2016 PDFDocument44 pagesSwaziland SOPs 2016 PDFTeguh PermanaNo ratings yet
- CryptococcosisDocument25 pagesCryptococcosisinvisibleyetinvincibleNo ratings yet
- CryptococcosisDocument17 pagesCryptococcosisKarthick AnbuNo ratings yet
- Fungalarthritis and OsteomyelitisDocument21 pagesFungalarthritis and OsteomyelitisYampold Estheben ChusiNo ratings yet
- Mycology Board Review Presentation10Document54 pagesMycology Board Review Presentation10Foysal SirazeeNo ratings yet
- Mec CronicaDocument29 pagesMec CronicaAlfredo Luis Arana MaqueraNo ratings yet
- Opportunistic MycosesDocument7 pagesOpportunistic MycosesAbhishek ChandraNo ratings yet
- PHT 112 Topic Quiz & Answers CompleteDocument24 pagesPHT 112 Topic Quiz & Answers CompletesammyNo ratings yet
- HivDocument36 pagesHivfenendriyaniNo ratings yet
- Assignment Hdb10503 Basic MicrobiologyDocument4 pagesAssignment Hdb10503 Basic MicrobiologyNida RidzuanNo ratings yet
- MYCOLOGYDocument33 pagesMYCOLOGYiwennieNo ratings yet
- Namibia Essential MedicinesDocument62 pagesNamibia Essential MedicinesportosinNo ratings yet
- Cryptococcosis - WikipediaDocument35 pagesCryptococcosis - Wikipedianoveva cenoNo ratings yet
- JASHC 2022 Abstracts19Document177 pagesJASHC 2022 Abstracts19Rodgers SsenyondoNo ratings yet
- Pigeon Excreta A Potential Source of Cryptococcus Neoformans and Their Antifungal Susceptibility ProfileDocument6 pagesPigeon Excreta A Potential Source of Cryptococcus Neoformans and Their Antifungal Susceptibility ProfileEditor IJTSRDNo ratings yet
- Chronic MeningitisDocument7 pagesChronic Meningitisneurojuancarfab100% (1)
- Opportunistic MycosesDocument13 pagesOpportunistic MycosesErnest CañosNo ratings yet
- Most Common Nelsons 16th EdDocument32 pagesMost Common Nelsons 16th EdRegine PanaliganNo ratings yet
- HIV Infection - Opportunistic InfectionsDocument21 pagesHIV Infection - Opportunistic InfectionszawadiNo ratings yet
- Final Consolidated Hiv-Aids Guidelines-2022Document380 pagesFinal Consolidated Hiv-Aids Guidelines-2022Odulusi DanielNo ratings yet
- Opportunistic Infections PDFDocument88 pagesOpportunistic Infections PDFironbuang100% (1)
- Cryptococcus ZoonosisDocument39 pagesCryptococcus ZoonosisLuluu CortésNo ratings yet