Download as pdf or txt
You might also like
- Dokumen - Pub Sbas For The Frcstramporth Examination A Companion To Postgraduate Orthopaedics Candidates Guide 1stnbsped 1108789978 9781108789974 1108803644 9781108803649 9781108846790Document646 pagesDokumen - Pub Sbas For The Frcstramporth Examination A Companion To Postgraduate Orthopaedics Candidates Guide 1stnbsped 1108789978 9781108789974 1108803644 9781108803649 9781108846790sharan sambhwani0% (2)
- Mitsubishi Lancer Owners HandbookDocument194 pagesMitsubishi Lancer Owners Handbookahmadkeshta100% (1)
- Artikel Bahasa Inggris Depresi 2Document6 pagesArtikel Bahasa Inggris Depresi 2Serli SafitriNo ratings yet
- The Association Between Diabetes Mellitus and DepressionDocument6 pagesThe Association Between Diabetes Mellitus and DepressionMeidy RamschieNo ratings yet
- Journal of Affective Disorders Volume 142 Issue 2012 (Doi 10.1016/s0165-0327 (12) 70004-6) Roy, Tapash Lloyd, Cathy E. - Epidemiology of Depression and Diabetes - A Systematic ReviewDocument14 pagesJournal of Affective Disorders Volume 142 Issue 2012 (Doi 10.1016/s0165-0327 (12) 70004-6) Roy, Tapash Lloyd, Cathy E. - Epidemiology of Depression and Diabetes - A Systematic ReviewSinta Rahmah SariNo ratings yet
- Cardiovascular Disease in People With DiabetesDocument11 pagesCardiovascular Disease in People With DiabetesSajal S.KumarNo ratings yet
- Major Depressive Disorder - New Clinical, Neurobiological, and Treatment PerspectivesDocument11 pagesMajor Depressive Disorder - New Clinical, Neurobiological, and Treatment PerspectivesArthur KummerNo ratings yet
- Psychosocial Support ofDocument13 pagesPsychosocial Support ofJEFFERSON MUÑOZNo ratings yet
- Does Treatment of Subsyndromal Depression Improve Depression and Diabetes Related OutcomesDocument9 pagesDoes Treatment of Subsyndromal Depression Improve Depression and Diabetes Related OutcomesRenato ObregónNo ratings yet
- Nouwen 2019Document11 pagesNouwen 2019Adrian SilaghiNo ratings yet
- Prevalence and Severity of DepressionDocument8 pagesPrevalence and Severity of DepressionWaheedullah AhmadiNo ratings yet
- Kupfer Et Al 2011 - Depression New TreatmentsDocument11 pagesKupfer Et Al 2011 - Depression New Treatmentsextra1zNo ratings yet
- Diabetic Medicine - 2017 - Perrin - The Prevalence of Diabetes Specific Emotional Distress in People With Type 2 DiabetesDocument13 pagesDiabetic Medicine - 2017 - Perrin - The Prevalence of Diabetes Specific Emotional Distress in People With Type 2 Diabetesnirmala amirNo ratings yet
- The Impact of Depression On Outcomes Following Acute Myocardial InfarctionDocument15 pagesThe Impact of Depression On Outcomes Following Acute Myocardial InfarctionChistan Junel DumoNo ratings yet
- On The Association Between Diabetes and Mental Disorders in A Community SampleDocument6 pagesOn The Association Between Diabetes and Mental Disorders in A Community SampleribkaNo ratings yet
- 62 Twenty Five Years of Diabetes Distress ResearchDocument8 pages62 Twenty Five Years of Diabetes Distress ResearchnaataajlaaNo ratings yet
- Diabetes DepressionDocument6 pagesDiabetes DepressionHaleelu Abdul JaleelNo ratings yet
- Onset Depression Health Related Risc Dztp2Document7 pagesOnset Depression Health Related Risc Dztp2Levente DobaiNo ratings yet
- Schmitt Et Al jpr2017 Depression-Related HyperglycaemiaDocument7 pagesSchmitt Et Al jpr2017 Depression-Related HyperglycaemiaTiToNo ratings yet
- The Thrifty Psychiatric PhenotypeDocument3 pagesThe Thrifty Psychiatric Phenotypeeduardobar2000No ratings yet
- Depression in Older Adults.21Document9 pagesDepression in Older Adults.21April Mae Balatibat LapueblaNo ratings yet
- Depression and Anxiety in Patients With COPD: Abebaw M. Yohannes and George S. AlexopoulosDocument5 pagesDepression and Anxiety in Patients With COPD: Abebaw M. Yohannes and George S. AlexopoulosAnthonyJohanNo ratings yet
- Diabetik Dan KelainannyaDocument11 pagesDiabetik Dan Kelainannyalatifah zahrohNo ratings yet
- Onset Depression Health Related Risc Dztp2Document7 pagesOnset Depression Health Related Risc Dztp2Levente DobaiNo ratings yet
- Manejo de Depresion en EMDocument17 pagesManejo de Depresion en EMAngela Villazon CriolloNo ratings yet
- Anxiety and Depression in Patients With Chronic Obstructive Pulmonary Disease (COPD) - A ReviewDocument6 pagesAnxiety and Depression in Patients With Chronic Obstructive Pulmonary Disease (COPD) - A ReviewArja' WaasNo ratings yet
- Soebandi Hospital) : Keywords: Diabetes Mellitus, Complication, Depression, Hamilton Depression Rating ScaleDocument6 pagesSoebandi Hospital) : Keywords: Diabetes Mellitus, Complication, Depression, Hamilton Depression Rating ScaleAoikiji KuzanNo ratings yet
- A Study of Depression in Diabetes Mellitus: Analysis From Rural Hospital, India 1Document6 pagesA Study of Depression in Diabetes Mellitus: Analysis From Rural Hospital, India 1International Medical PublisherNo ratings yet
- Seminar: Epidemiology, Comorbidity, and DiagnosisDocument11 pagesSeminar: Epidemiology, Comorbidity, and DiagnosisMartin GiraudoNo ratings yet
- What's Distressing About Having Type 1 DiabetesDocument14 pagesWhat's Distressing About Having Type 1 DiabetesTengku EltrikanawatiNo ratings yet
- Diabetes Distress Journal Review FINAL 2Document12 pagesDiabetes Distress Journal Review FINAL 2ZeroNine. TvNo ratings yet
- J Jocn 2017 09 022Document5 pagesJ Jocn 2017 09 022ÁngelesNo ratings yet
- Diabetes and Mental HealthDocument3 pagesDiabetes and Mental HealthVENNA FADILLAHNo ratings yet
- Alvah 492Document9 pagesAlvah 492adityakurniantoNo ratings yet
- Bipolar Pubmed IngDocument10 pagesBipolar Pubmed IngAsdhoNo ratings yet
- BBH 101h Written Report TBDocument11 pagesBBH 101h Written Report TBapi-608299493No ratings yet
- DiabetesSchizophreniaInterview CITROME BehavHealthCare2006Document8 pagesDiabetesSchizophreniaInterview CITROME BehavHealthCare2006Leslie CitromeNo ratings yet
- Comorbid Depression in Medical DiseasesDocument22 pagesComorbid Depression in Medical DiseasesArmando Marín FloresNo ratings yet
- The Costs of Depression - Kessler2012Document14 pagesThe Costs of Depression - Kessler2012chen eliseNo ratings yet
- A Review of Bipolar Disorder Among Adults PDFDocument13 pagesA Review of Bipolar Disorder Among Adults PDFNadyaNo ratings yet
- Feb 6 Introd Results Disc GPSY 513 Research Paper References AbstractDocument6 pagesFeb 6 Introd Results Disc GPSY 513 Research Paper References AbstractEva MartinNo ratings yet
- Cohen 2007 Stress and DiseaseDocument3 pagesCohen 2007 Stress and DiseaseBilly CooperNo ratings yet
- Cardiometabolic Risk in Patients With First Episode of - 2022 - Neuroscience ApDocument1 pageCardiometabolic Risk in Patients With First Episode of - 2022 - Neuroscience AploloasbNo ratings yet
- Gejala Depresi Pada Pasien Pasca Operasi Dan Peningkatan Sitokin Pro Inflamasi Pada Pasien Yang Menjalani Terapi Kanker Payudara.Document23 pagesGejala Depresi Pada Pasien Pasca Operasi Dan Peningkatan Sitokin Pro Inflamasi Pada Pasien Yang Menjalani Terapi Kanker Payudara.irfhanahusaNo ratings yet
- Binge Eating As A Determinant of Emotional State in Overweight and Obese MalesDocument5 pagesBinge Eating As A Determinant of Emotional State in Overweight and Obese Malesjudith goldmanNo ratings yet
- Appi Ajp 2017 17040409Document2 pagesAppi Ajp 2017 17040409jhuNo ratings yet
- The Association Between Insomnia and Cardiovascular DiseasesDocument8 pagesThe Association Between Insomnia and Cardiovascular Diseasesnouval_iqbalNo ratings yet
- Tmp66a1 TMPDocument10 pagesTmp66a1 TMPFrontiersNo ratings yet
- Shao2020 PDFDocument7 pagesShao2020 PDFAndrea ZambranoNo ratings yet
- Study of The Relationship Between Aggression and Chronic Diseases (Diabetes and Hypertension)Document5 pagesStudy of The Relationship Between Aggression and Chronic Diseases (Diabetes and Hypertension)tsujanaNo ratings yet
- Prevalence of Anxiety Among Diabetic Patients in Al-Madinah Al-Munawarah, Ksa 2021Document7 pagesPrevalence of Anxiety Among Diabetic Patients in Al-Madinah Al-Munawarah, Ksa 2021IJAR JOURNALNo ratings yet
- Studyprotocol Open Access: Gian Mauro Manzoni, Gianluca Castelnuovo and Enrico MolinariDocument8 pagesStudyprotocol Open Access: Gian Mauro Manzoni, Gianluca Castelnuovo and Enrico Molinarigguida0No ratings yet
- Suicide and Treatm EntDocument8 pagesSuicide and Treatm EntSourav DasNo ratings yet
- 4200 Research Report Form (3) Rough DraftDocument4 pages4200 Research Report Form (3) Rough Draftapi-285634882No ratings yet
- M5W Wang FeedbackDocument21 pagesM5W Wang FeedbackIsaac HassanNo ratings yet
- Bipolar Disorder in Adults - Epidemiology and Pathogenesis - UpToDateDocument17 pagesBipolar Disorder in Adults - Epidemiology and Pathogenesis - UpToDateOmar FallutoNo ratings yet
- Articulo de Psiquiatria, DepresiónDocument5 pagesArticulo de Psiquiatria, Depresiónterecrabb_718751911No ratings yet
- Use of Antidepressants To Treat Depression in Bipolar Disorder.Document5 pagesUse of Antidepressants To Treat Depression in Bipolar Disorder.teddypolNo ratings yet
- 2015 Article 118Document14 pages2015 Article 118Denisse DelgadoNo ratings yet
- Origin ArticleDocument8 pagesOrigin ArticleMaya Putri HaryantiNo ratings yet
- PCC 11258Document5 pagesPCC 11258Alina PopaNo ratings yet
- Rethinking Diabetes: Entanglements with Trauma, Poverty, and HIVFrom EverandRethinking Diabetes: Entanglements with Trauma, Poverty, and HIVNo ratings yet
- Nursing Care Plan - Using NandaDocument16 pagesNursing Care Plan - Using NandaWardinatul ImanNo ratings yet
- B1 Questions QN001: Form Questions Which Ask For The Underlined WordsDocument2 pagesB1 Questions QN001: Form Questions Which Ask For The Underlined WordsMirjana Paunovic100% (1)
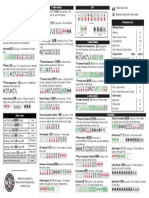
- Closed Hand Only Reduced Value When Hand Open: 2-Han Hands KEY 1-Han HandsDocument1 pageClosed Hand Only Reduced Value When Hand Open: 2-Han Hands KEY 1-Han Hands8o1kfW9No ratings yet
- Get To Know The Newly Redesigned Texas DL and ID Cards: Adult & Under 21 Identification CardDocument2 pagesGet To Know The Newly Redesigned Texas DL and ID Cards: Adult & Under 21 Identification Carddominique marshallNo ratings yet
- Normal ForceDocument29 pagesNormal ForceRusella Mariz EsteronNo ratings yet
- DemblaDocument12 pagesDemblaISHAN VERMANo ratings yet
- CRYOGENIC TRANSFER System - Mechanical Design Handbook - Cryo - Transfer - System PDFDocument33 pagesCRYOGENIC TRANSFER System - Mechanical Design Handbook - Cryo - Transfer - System PDFDayo IdowuNo ratings yet
- UK DynaSand C0209Document2 pagesUK DynaSand C0209Mee DepoNo ratings yet
- 2&3&4&5 Burner Induction+Infrared Cooker Quotations-Alan Liu (LONGSTAR)Document9 pages2&3&4&5 Burner Induction+Infrared Cooker Quotations-Alan Liu (LONGSTAR)Dương Nguyễn ĐắcNo ratings yet
- Solid State13thDocument19 pagesSolid State13thRaju SinghNo ratings yet
- Dbsmote: Density-Based Synthetic Minority Over-Sampling TechniqueDocument21 pagesDbsmote: Density-Based Synthetic Minority Over-Sampling TechniqueIndi Wei-Huan HuNo ratings yet
- Your Results For: "Multiple Choice Questions": Always Receive Straight CommissionDocument4 pagesYour Results For: "Multiple Choice Questions": Always Receive Straight CommissionRaman KulkarniNo ratings yet
- Survey Questionnaire PresentationDocument14 pagesSurvey Questionnaire PresentationFaith PaladoNo ratings yet
- EDUC 70 Module 2.2Document4 pagesEDUC 70 Module 2.2Leslie mae GioNo ratings yet
- Butternut Squash SoupDocument1 pageButternut Squash SouplyllacycusNo ratings yet
- 04 Abstract-Central WorkshopDocument75 pages04 Abstract-Central Workshopumesh prustyNo ratings yet
- Godrej Case Study For Business Intelligence and Reporting ServicesDocument4 pagesGodrej Case Study For Business Intelligence and Reporting ServicesSonu LovesforuNo ratings yet
- Epoxy - Chemical ResistanceDocument13 pagesEpoxy - Chemical ResistanceLaxmesh Hegde100% (1)
- Powered ExoskeletonDocument22 pagesPowered ExoskeletonSarfaras Ali K100% (1)
- Dactylorhiza PaperDocument6 pagesDactylorhiza PaperBrij Mohan SinghNo ratings yet
- Ferrups FE Series: FeaturesDocument2 pagesFerrups FE Series: Featuresandy175No ratings yet
- Chem Jeem SeptDocument62 pagesChem Jeem SeptStephen SatwikNo ratings yet
- ADV Word GivenDocument13 pagesADV Word Givengloria500100% (1)
- SDS Weberfloor VB ResinDocument25 pagesSDS Weberfloor VB ResinMaha MuflehNo ratings yet
- 16-31 Maret 2021Document23 pages16-31 Maret 2021Medika AntapaniNo ratings yet
- Pressure Vessel DesignDocument46 pagesPressure Vessel DesignAxenta0% (1)
- Financial Inclusion Through Small Finance BanksDocument16 pagesFinancial Inclusion Through Small Finance BanksbobNo ratings yet
- Primary Frca Help Plain UpdatedDocument5 pagesPrimary Frca Help Plain UpdatedDavid PappinNo ratings yet