
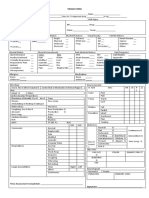
It U Physician Assessment Sheet
It U Physician Assessment Sheet
You might also like
- 2018 ESMO Handbook of Interpreting Oncological Study PublicationsDocument219 pages2018 ESMO Handbook of Interpreting Oncological Study PublicationsAlex Lugli100% (1)
- EndoquestionssolvedDocument14 pagesEndoquestionssolvedPuteri Nursyamimi Mohd SabilanNo ratings yet
- Bronchial Artery Embolization: DR Tinku JosephDocument51 pagesBronchial Artery Embolization: DR Tinku JosephRadison sierraNo ratings yet
- 2013 Urology CatalogDocument233 pages2013 Urology CatalogAna LauraNo ratings yet
- Neurosurgery Pre-Assessment Clinic Proforma TemplateDocument5 pagesNeurosurgery Pre-Assessment Clinic Proforma TemplateEslam Kandil100% (1)
- Intern Survival Guide 2014-2015Document145 pagesIntern Survival Guide 2014-2015Katie Kroll BradyNo ratings yet
- Basic Training For: Barangay Health Workers Barangay Nutrition ScholarDocument16 pagesBasic Training For: Barangay Health Workers Barangay Nutrition ScholarMario Hipolito100% (5)
- Suez Canal University/ Faculty of Nursing (Medical Surgical Nursing/ Clinical Assessment Sheet 2 Year 2020/2021)Document18 pagesSuez Canal University/ Faculty of Nursing (Medical Surgical Nursing/ Clinical Assessment Sheet 2 Year 2020/2021)طالب جامعة100% (1)
- DiureticsDocument61 pagesDiureticsJoyce WacukaNo ratings yet
- Family OSCE SummaryDocument12 pagesFamily OSCE SummarySarah ANo ratings yet
- Collaborative Care Clinical Manifestations: Concept MapDocument3 pagesCollaborative Care Clinical Manifestations: Concept MapMaica LectanaNo ratings yet
- Manual On Benchmarkin of QUality Improvement1Document42 pagesManual On Benchmarkin of QUality Improvement1James Lagamayo JavierNo ratings yet
- Abdominal Pain ManagementDocument3 pagesAbdominal Pain ManagementTeenu JobyNo ratings yet
- LabReportNew - 2022-12-29 EKTAT213904.745Document5 pagesLabReportNew - 2022-12-29 EKTAT213904.745Ekta BaraskarNo ratings yet
- Prevention of Cardiovascular Disease: Pocket Guidelines For Assessment and Management of Cardiovascular RiskDocument20 pagesPrevention of Cardiovascular Disease: Pocket Guidelines For Assessment and Management of Cardiovascular RiskCaryl Kit Balani TimtimNo ratings yet
- Triage FormDocument2 pagesTriage FormCael LayugNo ratings yet
- Stroke Program Education May2022Document22 pagesStroke Program Education May2022Laura VelaNo ratings yet
- R1 Orientation, Oncall Issues.Document55 pagesR1 Orientation, Oncall Issues.latifaNo ratings yet
- Family Medicine Clerkship Logbook G3 FinalDocument76 pagesFamily Medicine Clerkship Logbook G3 FinalMohammed AlomarNo ratings yet
- Age Related Cerebral Cortical Atrophy Is SeenDocument5 pagesAge Related Cerebral Cortical Atrophy Is SeenTamanash ChowdharyNo ratings yet
- Roh2201123544 2Document3 pagesRoh2201123544 2Ruby kushwahNo ratings yet
- LYMPHOGRAPHY-WPS OfficeDocument11 pagesLYMPHOGRAPHY-WPS OfficePax Giuseppe0% (1)
- Format of History and PEDocument2 pagesFormat of History and PEJill Eizavel BertisNo ratings yet
- Prospectus: Programmes OfferedDocument70 pagesProspectus: Programmes OfferedPrajwal MkNo ratings yet
- Report Annaswamy UnlockedDocument7 pagesReport Annaswamy UnlockedBhaskhar AnnaswamyNo ratings yet
- Echo ReportDocument2 pagesEcho ReportweareweNo ratings yet
- The Effect of Obesity On Lung FunctionDocument25 pagesThe Effect of Obesity On Lung FunctionharvardboyNo ratings yet
- National Guideline For Dengue 2018 PDFDocument96 pagesNational Guideline For Dengue 2018 PDFTapash GopeNo ratings yet
- Positive Malaria Parasite Identification Test Report Format Example Sample Template Drlogy Lab ReportDocument1 pagePositive Malaria Parasite Identification Test Report Format Example Sample Template Drlogy Lab ReportMichaelNo ratings yet
- Dengue: Subjective FindingsDocument5 pagesDengue: Subjective FindingsRaghu VenkatNo ratings yet
- Total Artificial HeartDocument4 pagesTotal Artificial HeartRubz BulquerinNo ratings yet
- AbbreviationDocument90 pagesAbbreviationIrwanshah MohammadNo ratings yet
- CGHS RateListDocument45 pagesCGHS RateListSandip SharmaNo ratings yet
- Department of Chemical Pathology: Ena Quantrix 25 IggDocument2 pagesDepartment of Chemical Pathology: Ena Quantrix 25 IggKhurram ShehzadNo ratings yet
- DR - Darez Ahamed Vision For Tamil NaduDocument6 pagesDR - Darez Ahamed Vision For Tamil NaduBrunoNo ratings yet
- Lmfxt13worgcnkmx0k55zkcf PDFDocument2 pagesLmfxt13worgcnkmx0k55zkcf PDFamit guptaNo ratings yet
- Approach To A Patient With Fever?: 1 DR - Shamol /inter/feverDocument28 pagesApproach To A Patient With Fever?: 1 DR - Shamol /inter/feverkiloNo ratings yet
- Neuro PerformaDocument5 pagesNeuro PerformaSara KhanNo ratings yet
- Omnibus Health Guidelines For The Elderly 2022Document81 pagesOmnibus Health Guidelines For The Elderly 2022Raymunda Rauto-avila100% (1)
- Ome MicroDocument9 pagesOme MicroRiya ThoratNo ratings yet
- Allll Exams Combinedd FinalDocument14 pagesAllll Exams Combinedd FinalAnshuNo ratings yet
- SBT 13Document1 pageSBT 13Krishna Bharadwaj ReddyNo ratings yet
- Lab TestDocument7 pagesLab TestNIKKI JOYCE PASIANNo ratings yet
- Patient Reported OutcomesDocument17 pagesPatient Reported OutcomesSajjad alipourNo ratings yet
- Hypoglycemia: The Neglected Complication: Review ArticleDocument16 pagesHypoglycemia: The Neglected Complication: Review Articlesiti nur aishah jalilNo ratings yet
- Delayed Drug Hypersensitivity Reactions: Molecular Recognition, Genetic Susceptibility, and Immune MediatorsDocument20 pagesDelayed Drug Hypersensitivity Reactions: Molecular Recognition, Genetic Susceptibility, and Immune MediatorsTatiana Rejón CabezasNo ratings yet
- The Common Symptoms Guide 5eDocument411 pagesThe Common Symptoms Guide 5eseyalel959100% (1)
- PT Intake FormDocument4 pagesPT Intake FormChifor FlorinNo ratings yet
- European Stroke Organisation Guideline On Endarterectomy and Stenting For Carotid Artery Stenosis, 2021Document47 pagesEuropean Stroke Organisation Guideline On Endarterectomy and Stenting For Carotid Artery Stenosis, 2021CAMILO ARMANDO BENAVIDES BURBANO100% (1)
- Ccebdm Module 8Document140 pagesCcebdm Module 8AnkurNo ratings yet
- Drug AddictionDocument19 pagesDrug Addictiontrigui amir100% (1)
- MCEM Part A Bromely Emergency MedicineDocument160 pagesMCEM Part A Bromely Emergency Medicinejones dondoNo ratings yet
- VILLANUEVA Nephrology APE Presentation NotesDocument8 pagesVILLANUEVA Nephrology APE Presentation NotesDeanne Kathleen VillanuevaNo ratings yet
- MR. No. 20081290896 Lab No. Collection: Name: Gender: Male Age: 31 YearsDocument1 pageMR. No. 20081290896 Lab No. Collection: Name: Gender: Male Age: 31 YearsПомощникПомощникNo ratings yet
- Client Information Sheet (For Individual Client)Document1 pageClient Information Sheet (For Individual Client)Daphne Delos SantosNo ratings yet
- Skilled Immigration-Assessment-FormDocument10 pagesSkilled Immigration-Assessment-FormBousekine Siham100% (1)
- AWESOME ASSESMENT AND PLAN LibrarydocxDocument49 pagesAWESOME ASSESMENT AND PLAN LibrarydocxAndrew McGowanNo ratings yet
- New Patient AdmitDocument2 pagesNew Patient AdmitNetradeep Narayansa DagduNo ratings yet
- Shoukat Lab ReportDocument1 pageShoukat Lab ReportKeep smileNo ratings yet
- CLL PatientReportDocument1 pageCLL PatientReportabdullahqqNo ratings yet
- 9-Andre Tan - S Surgical NotesDocument163 pages9-Andre Tan - S Surgical Notes肖楚天No ratings yet
- About Blanket 5Document1 pageAbout Blanket 5Sankit SasmalNo ratings yet
- Oral Schedule v5Document12 pagesOral Schedule v5Fiola FinandakasihNo ratings yet
- Obtaining A Wound Swab Culture SpecimenDocument2 pagesObtaining A Wound Swab Culture SpecimenMarj MendezNo ratings yet
- Darren ResumeDocument3 pagesDarren ResumezderonNo ratings yet
- Integrative Medicine and PhitotherapyDocument72 pagesIntegrative Medicine and PhitotherapyLibAmauNo ratings yet
- NCLEX Review ExamplefinalDocument52 pagesNCLEX Review Examplefinalisapatrick8126100% (1)
- A Case Report On Chronic Kidney DiseaseDocument4 pagesA Case Report On Chronic Kidney DiseaseEditor IJTSRDNo ratings yet
- JRCO - SOP - 001 Safety Reporting Final2012Document21 pagesJRCO - SOP - 001 Safety Reporting Final2012mrk_rlndNo ratings yet
- AYUSH Centre Entry Level For PrintDocument44 pagesAYUSH Centre Entry Level For Printshubham kumarNo ratings yet
- Communicating Clearly About MedicinesDocument125 pagesCommunicating Clearly About MedicinesDaniel MeloNo ratings yet
- Sitti Khadijah Hospital / Indah Ria Rezeki Meirisa Morning Report, January 4 2022Document2 pagesSitti Khadijah Hospital / Indah Ria Rezeki Meirisa Morning Report, January 4 2022Fitria AriantyNo ratings yet
- Dissection Hall Ethics: Roles and ResponsibilitiesDocument4 pagesDissection Hall Ethics: Roles and ResponsibilitiesIJAR JOURNALNo ratings yet
- (Clin Sports Med) - The Interface Between Sports Psychiatry and Spor Volume 24 Issue 4 October (2006) PDFDocument230 pages(Clin Sports Med) - The Interface Between Sports Psychiatry and Spor Volume 24 Issue 4 October (2006) PDFBIGZZZNo ratings yet
- Ebert 1987Document5 pagesEbert 1987Dheana Thalya AzzahraNo ratings yet
- Systemic and Local Applications of Steroids in Endodontics: An Update ReviewDocument8 pagesSystemic and Local Applications of Steroids in Endodontics: An Update ReviewJorge OrbeNo ratings yet
- PDF Lecture 9 Benign Soft Tissue TumorsDocument131 pagesPDF Lecture 9 Benign Soft Tissue TumorsMuhammad Rizqi100% (1)
- FMCH MidtermsDocument91 pagesFMCH MidtermsjandaniellerasNo ratings yet
- Medical Waste Disposal BrochureDocument3 pagesMedical Waste Disposal BrochureRachael HernandezNo ratings yet
- CTG Interpretation and Response - 280720Document7 pagesCTG Interpretation and Response - 280720Yane Aulia YasminNo ratings yet
- SPIRIVA HandiHaler InstructionsDocument11 pagesSPIRIVA HandiHaler InstructionsMario WilmathNo ratings yet
- Delirium and Acute Confusional States - Prevention, Treatment, and Prognosis - UpToDateDocument18 pagesDelirium and Acute Confusional States - Prevention, Treatment, and Prognosis - UpToDateKarina CabayNo ratings yet
- Free Download Oxford Handbook of Medical Ethics and Law Anna Smajdor Full Chapter PDFDocument51 pagesFree Download Oxford Handbook of Medical Ethics and Law Anna Smajdor Full Chapter PDFlawrence.hendrix951100% (24)
- DLA Piper Global Telehealth Guide December 2020Document145 pagesDLA Piper Global Telehealth Guide December 2020grimace11No ratings yet
- Pain ManagementDocument175 pagesPain ManagementBobby Noel Cerro Jr100% (4)
- Oncoplastic Breast SurgeryDocument27 pagesOncoplastic Breast SurgeryReem Amr El-DafrawiNo ratings yet
- Price List###Document35 pagesPrice List###Balai Pengobatan AdventNo ratings yet
- Energy Healing TechniquesDocument17 pagesEnergy Healing TechniquesRAMESHBABUNo ratings yet
- Aua 2012Document90 pagesAua 2012Tawfiq El-Far100% (5)
- Nwabshah Children HospitalDocument6 pagesNwabshah Children HospitalJunaid AhmedNo ratings yet






















































































Download as pdf or txt
You might also like
- 2018 ESMO Handbook of Interpreting Oncological Study PublicationsDocument219 pages2018 ESMO Handbook of Interpreting Oncological Study PublicationsAlex Lugli100% (1)
- EndoquestionssolvedDocument14 pagesEndoquestionssolvedPuteri Nursyamimi Mohd SabilanNo ratings yet
- Bronchial Artery Embolization: DR Tinku JosephDocument51 pagesBronchial Artery Embolization: DR Tinku JosephRadison sierraNo ratings yet
- 2013 Urology CatalogDocument233 pages2013 Urology CatalogAna LauraNo ratings yet
- Neurosurgery Pre-Assessment Clinic Proforma TemplateDocument5 pagesNeurosurgery Pre-Assessment Clinic Proforma TemplateEslam Kandil100% (1)
- Intern Survival Guide 2014-2015Document145 pagesIntern Survival Guide 2014-2015Katie Kroll BradyNo ratings yet
- Basic Training For: Barangay Health Workers Barangay Nutrition ScholarDocument16 pagesBasic Training For: Barangay Health Workers Barangay Nutrition ScholarMario Hipolito100% (5)
- Suez Canal University/ Faculty of Nursing (Medical Surgical Nursing/ Clinical Assessment Sheet 2 Year 2020/2021)Document18 pagesSuez Canal University/ Faculty of Nursing (Medical Surgical Nursing/ Clinical Assessment Sheet 2 Year 2020/2021)طالب جامعة100% (1)
- DiureticsDocument61 pagesDiureticsJoyce WacukaNo ratings yet
- Family OSCE SummaryDocument12 pagesFamily OSCE SummarySarah ANo ratings yet
- Collaborative Care Clinical Manifestations: Concept MapDocument3 pagesCollaborative Care Clinical Manifestations: Concept MapMaica LectanaNo ratings yet
- Manual On Benchmarkin of QUality Improvement1Document42 pagesManual On Benchmarkin of QUality Improvement1James Lagamayo JavierNo ratings yet
- Abdominal Pain ManagementDocument3 pagesAbdominal Pain ManagementTeenu JobyNo ratings yet
- LabReportNew - 2022-12-29 EKTAT213904.745Document5 pagesLabReportNew - 2022-12-29 EKTAT213904.745Ekta BaraskarNo ratings yet
- Prevention of Cardiovascular Disease: Pocket Guidelines For Assessment and Management of Cardiovascular RiskDocument20 pagesPrevention of Cardiovascular Disease: Pocket Guidelines For Assessment and Management of Cardiovascular RiskCaryl Kit Balani TimtimNo ratings yet
- Triage FormDocument2 pagesTriage FormCael LayugNo ratings yet
- Stroke Program Education May2022Document22 pagesStroke Program Education May2022Laura VelaNo ratings yet
- R1 Orientation, Oncall Issues.Document55 pagesR1 Orientation, Oncall Issues.latifaNo ratings yet
- Family Medicine Clerkship Logbook G3 FinalDocument76 pagesFamily Medicine Clerkship Logbook G3 FinalMohammed AlomarNo ratings yet
- Age Related Cerebral Cortical Atrophy Is SeenDocument5 pagesAge Related Cerebral Cortical Atrophy Is SeenTamanash ChowdharyNo ratings yet
- Roh2201123544 2Document3 pagesRoh2201123544 2Ruby kushwahNo ratings yet
- LYMPHOGRAPHY-WPS OfficeDocument11 pagesLYMPHOGRAPHY-WPS OfficePax Giuseppe0% (1)
- Format of History and PEDocument2 pagesFormat of History and PEJill Eizavel BertisNo ratings yet
- Prospectus: Programmes OfferedDocument70 pagesProspectus: Programmes OfferedPrajwal MkNo ratings yet
- Report Annaswamy UnlockedDocument7 pagesReport Annaswamy UnlockedBhaskhar AnnaswamyNo ratings yet
- Echo ReportDocument2 pagesEcho ReportweareweNo ratings yet
- The Effect of Obesity On Lung FunctionDocument25 pagesThe Effect of Obesity On Lung FunctionharvardboyNo ratings yet
- National Guideline For Dengue 2018 PDFDocument96 pagesNational Guideline For Dengue 2018 PDFTapash GopeNo ratings yet
- Positive Malaria Parasite Identification Test Report Format Example Sample Template Drlogy Lab ReportDocument1 pagePositive Malaria Parasite Identification Test Report Format Example Sample Template Drlogy Lab ReportMichaelNo ratings yet
- Dengue: Subjective FindingsDocument5 pagesDengue: Subjective FindingsRaghu VenkatNo ratings yet
- Total Artificial HeartDocument4 pagesTotal Artificial HeartRubz BulquerinNo ratings yet
- AbbreviationDocument90 pagesAbbreviationIrwanshah MohammadNo ratings yet
- CGHS RateListDocument45 pagesCGHS RateListSandip SharmaNo ratings yet
- Department of Chemical Pathology: Ena Quantrix 25 IggDocument2 pagesDepartment of Chemical Pathology: Ena Quantrix 25 IggKhurram ShehzadNo ratings yet
- DR - Darez Ahamed Vision For Tamil NaduDocument6 pagesDR - Darez Ahamed Vision For Tamil NaduBrunoNo ratings yet
- Lmfxt13worgcnkmx0k55zkcf PDFDocument2 pagesLmfxt13worgcnkmx0k55zkcf PDFamit guptaNo ratings yet
- Approach To A Patient With Fever?: 1 DR - Shamol /inter/feverDocument28 pagesApproach To A Patient With Fever?: 1 DR - Shamol /inter/feverkiloNo ratings yet
- Neuro PerformaDocument5 pagesNeuro PerformaSara KhanNo ratings yet
- Omnibus Health Guidelines For The Elderly 2022Document81 pagesOmnibus Health Guidelines For The Elderly 2022Raymunda Rauto-avila100% (1)
- Ome MicroDocument9 pagesOme MicroRiya ThoratNo ratings yet
- Allll Exams Combinedd FinalDocument14 pagesAllll Exams Combinedd FinalAnshuNo ratings yet
- SBT 13Document1 pageSBT 13Krishna Bharadwaj ReddyNo ratings yet
- Lab TestDocument7 pagesLab TestNIKKI JOYCE PASIANNo ratings yet
- Patient Reported OutcomesDocument17 pagesPatient Reported OutcomesSajjad alipourNo ratings yet
- Hypoglycemia: The Neglected Complication: Review ArticleDocument16 pagesHypoglycemia: The Neglected Complication: Review Articlesiti nur aishah jalilNo ratings yet
- Delayed Drug Hypersensitivity Reactions: Molecular Recognition, Genetic Susceptibility, and Immune MediatorsDocument20 pagesDelayed Drug Hypersensitivity Reactions: Molecular Recognition, Genetic Susceptibility, and Immune MediatorsTatiana Rejón CabezasNo ratings yet
- The Common Symptoms Guide 5eDocument411 pagesThe Common Symptoms Guide 5eseyalel959100% (1)
- PT Intake FormDocument4 pagesPT Intake FormChifor FlorinNo ratings yet
- European Stroke Organisation Guideline On Endarterectomy and Stenting For Carotid Artery Stenosis, 2021Document47 pagesEuropean Stroke Organisation Guideline On Endarterectomy and Stenting For Carotid Artery Stenosis, 2021CAMILO ARMANDO BENAVIDES BURBANO100% (1)
- Ccebdm Module 8Document140 pagesCcebdm Module 8AnkurNo ratings yet
- Drug AddictionDocument19 pagesDrug Addictiontrigui amir100% (1)
- MCEM Part A Bromely Emergency MedicineDocument160 pagesMCEM Part A Bromely Emergency Medicinejones dondoNo ratings yet
- VILLANUEVA Nephrology APE Presentation NotesDocument8 pagesVILLANUEVA Nephrology APE Presentation NotesDeanne Kathleen VillanuevaNo ratings yet
- MR. No. 20081290896 Lab No. Collection: Name: Gender: Male Age: 31 YearsDocument1 pageMR. No. 20081290896 Lab No. Collection: Name: Gender: Male Age: 31 YearsПомощникПомощникNo ratings yet
- Client Information Sheet (For Individual Client)Document1 pageClient Information Sheet (For Individual Client)Daphne Delos SantosNo ratings yet
- Skilled Immigration-Assessment-FormDocument10 pagesSkilled Immigration-Assessment-FormBousekine Siham100% (1)
- AWESOME ASSESMENT AND PLAN LibrarydocxDocument49 pagesAWESOME ASSESMENT AND PLAN LibrarydocxAndrew McGowanNo ratings yet
- New Patient AdmitDocument2 pagesNew Patient AdmitNetradeep Narayansa DagduNo ratings yet
- Shoukat Lab ReportDocument1 pageShoukat Lab ReportKeep smileNo ratings yet
- CLL PatientReportDocument1 pageCLL PatientReportabdullahqqNo ratings yet
- 9-Andre Tan - S Surgical NotesDocument163 pages9-Andre Tan - S Surgical Notes肖楚天No ratings yet
- About Blanket 5Document1 pageAbout Blanket 5Sankit SasmalNo ratings yet
- Oral Schedule v5Document12 pagesOral Schedule v5Fiola FinandakasihNo ratings yet
- Obtaining A Wound Swab Culture SpecimenDocument2 pagesObtaining A Wound Swab Culture SpecimenMarj MendezNo ratings yet
- Darren ResumeDocument3 pagesDarren ResumezderonNo ratings yet
- Integrative Medicine and PhitotherapyDocument72 pagesIntegrative Medicine and PhitotherapyLibAmauNo ratings yet
- NCLEX Review ExamplefinalDocument52 pagesNCLEX Review Examplefinalisapatrick8126100% (1)
- A Case Report On Chronic Kidney DiseaseDocument4 pagesA Case Report On Chronic Kidney DiseaseEditor IJTSRDNo ratings yet
- JRCO - SOP - 001 Safety Reporting Final2012Document21 pagesJRCO - SOP - 001 Safety Reporting Final2012mrk_rlndNo ratings yet
- AYUSH Centre Entry Level For PrintDocument44 pagesAYUSH Centre Entry Level For Printshubham kumarNo ratings yet
- Communicating Clearly About MedicinesDocument125 pagesCommunicating Clearly About MedicinesDaniel MeloNo ratings yet
- Sitti Khadijah Hospital / Indah Ria Rezeki Meirisa Morning Report, January 4 2022Document2 pagesSitti Khadijah Hospital / Indah Ria Rezeki Meirisa Morning Report, January 4 2022Fitria AriantyNo ratings yet
- Dissection Hall Ethics: Roles and ResponsibilitiesDocument4 pagesDissection Hall Ethics: Roles and ResponsibilitiesIJAR JOURNALNo ratings yet
- (Clin Sports Med) - The Interface Between Sports Psychiatry and Spor Volume 24 Issue 4 October (2006) PDFDocument230 pages(Clin Sports Med) - The Interface Between Sports Psychiatry and Spor Volume 24 Issue 4 October (2006) PDFBIGZZZNo ratings yet
- Ebert 1987Document5 pagesEbert 1987Dheana Thalya AzzahraNo ratings yet
- Systemic and Local Applications of Steroids in Endodontics: An Update ReviewDocument8 pagesSystemic and Local Applications of Steroids in Endodontics: An Update ReviewJorge OrbeNo ratings yet
- PDF Lecture 9 Benign Soft Tissue TumorsDocument131 pagesPDF Lecture 9 Benign Soft Tissue TumorsMuhammad Rizqi100% (1)
- FMCH MidtermsDocument91 pagesFMCH MidtermsjandaniellerasNo ratings yet
- Medical Waste Disposal BrochureDocument3 pagesMedical Waste Disposal BrochureRachael HernandezNo ratings yet
- CTG Interpretation and Response - 280720Document7 pagesCTG Interpretation and Response - 280720Yane Aulia YasminNo ratings yet
- SPIRIVA HandiHaler InstructionsDocument11 pagesSPIRIVA HandiHaler InstructionsMario WilmathNo ratings yet
- Delirium and Acute Confusional States - Prevention, Treatment, and Prognosis - UpToDateDocument18 pagesDelirium and Acute Confusional States - Prevention, Treatment, and Prognosis - UpToDateKarina CabayNo ratings yet
- Free Download Oxford Handbook of Medical Ethics and Law Anna Smajdor Full Chapter PDFDocument51 pagesFree Download Oxford Handbook of Medical Ethics and Law Anna Smajdor Full Chapter PDFlawrence.hendrix951100% (24)
- DLA Piper Global Telehealth Guide December 2020Document145 pagesDLA Piper Global Telehealth Guide December 2020grimace11No ratings yet
- Pain ManagementDocument175 pagesPain ManagementBobby Noel Cerro Jr100% (4)
- Oncoplastic Breast SurgeryDocument27 pagesOncoplastic Breast SurgeryReem Amr El-DafrawiNo ratings yet
- Price List###Document35 pagesPrice List###Balai Pengobatan AdventNo ratings yet
- Energy Healing TechniquesDocument17 pagesEnergy Healing TechniquesRAMESHBABUNo ratings yet
- Aua 2012Document90 pagesAua 2012Tawfiq El-Far100% (5)
- Nwabshah Children HospitalDocument6 pagesNwabshah Children HospitalJunaid AhmedNo ratings yet