Download as pdf or txt
You might also like
- Pediatric ProsthodonticsDocument84 pagesPediatric Prosthodonticsnihu100% (2)
- Completedenture Theory and PracticeDocument1,233 pagesCompletedenture Theory and PracticeMostafa Fayad100% (7)
- Immediate Dentures - PPT (Autosaved)Document70 pagesImmediate Dentures - PPT (Autosaved)Pratik Chheda100% (6)
- Saudi License Exam - SLE (DENTAL Test Papers) Set-1Document108 pagesSaudi License Exam - SLE (DENTAL Test Papers) Set-1Adeel Ahmad86% (22)
- Standard Edgewise 2.6.2020Document110 pagesStandard Edgewise 2.6.2020nikita100% (3)
- Denture HandbookDocument13 pagesDenture HandbookBesHo TwadroUsNo ratings yet
- Interim (Transitional) Immediate DentureDocument8 pagesInterim (Transitional) Immediate DentureKrupali JainNo ratings yet
- Principles of Removable Denture Pros Tho Don Tics 2007-08 - KaddahDocument145 pagesPrinciples of Removable Denture Pros Tho Don Tics 2007-08 - KaddahJudy Abbott100% (1)
- A To Z Orthodontics Vol 20 SurgicalDocument23 pagesA To Z Orthodontics Vol 20 Surgicalshruti premsagarNo ratings yet
- 1) Introduction To Pre Clinical Complete Denture PDFDocument56 pages1) Introduction To Pre Clinical Complete Denture PDFMustafa AhmedNo ratings yet
- Single Denture 4th Year 8-3-2020Document37 pagesSingle Denture 4th Year 8-3-2020Ledia EssamNo ratings yet
- A To Z Orthodontics - Vol 9 - Preventive and Interceptive OrthodonticsDocument37 pagesA To Z Orthodontics - Vol 9 - Preventive and Interceptive OrthodonticsĐạt HuỳnhNo ratings yet
- I014634952 PDFDocument4 pagesI014634952 PDFGowriKrishnaraoNo ratings yet
- DentureDocument80 pagesDentureDrShweta SainiNo ratings yet
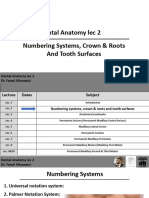
- DA Lec.2 Numbering Systems, Crown & RootsDocument26 pagesDA Lec.2 Numbering Systems, Crown & Rootswqdyyp9hw2No ratings yet
- Mouth Preparation For RPD Treatment-1-ModifiedDocument76 pagesMouth Preparation For RPD Treatment-1-ModifiedShemi SirajNo ratings yet
- Lec12 4th ClassDocument8 pagesLec12 4th ClassYaser JasNo ratings yet
- Indirect Restoration That Covered On or More Cusp and It Is Located Between Oclusal Surfaces of The Posterior Tooth Too Damage The Basics FillingDocument4 pagesIndirect Restoration That Covered On or More Cusp and It Is Located Between Oclusal Surfaces of The Posterior Tooth Too Damage The Basics FillingBagas Luthfi AlfatNo ratings yet
- 5 DR Ashfaq Tooth Extraction Abeer SignedDocument140 pages5 DR Ashfaq Tooth Extraction Abeer Signedali tiwanaNo ratings yet
- Oral and Maxillofacial SurgeryDocument22 pagesOral and Maxillofacial SurgeryafheaNo ratings yet
- Try-In RPDDocument8 pagesTry-In RPDSRO oONo ratings yet
- A To Z Orthodontics. Volume 9: Preventive and Interceptive OrthodonticsDocument38 pagesA To Z Orthodontics. Volume 9: Preventive and Interceptive OrthodonticsNayan NayanNo ratings yet
- Kirkuk Dentistry Collage: Complete DentureDocument15 pagesKirkuk Dentistry Collage: Complete Dentureمحمد عبدالهادي إسماعيلNo ratings yet
- Acrylic Removable Partial Denture (RPD)Document6 pagesAcrylic Removable Partial Denture (RPD)israaNo ratings yet
- Immediate Denture KhlygaDocument8 pagesImmediate Denture Khlygahanya.mohammedNo ratings yet
- Preventive Orthodontics / Orthodontic Courses by Indian Dental AcademyDocument15 pagesPreventive Orthodontics / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Fundamentals of Tooth PreparationDocument50 pagesFundamentals of Tooth Preparationمعاذ نوري محمدNo ratings yet
- محاضرات impression bite ثالث تكنولوجيا مؤقت مراحل 2024Document55 pagesمحاضرات impression bite ثالث تكنولوجيا مؤقت مراحل 2024محمد عبدالعالم البدويNo ratings yet
- Indication and Contraindication of ExodontiaDocument9 pagesIndication and Contraindication of ExodontiaSagad AlaaNo ratings yet
- Oral Surgery: Indication & Contra-Indication of ExtractionDocument9 pagesOral Surgery: Indication & Contra-Indication of Extractionتركيه تركيهNo ratings yet
- Mouth Preparation in RPDDocument14 pagesMouth Preparation in RPDDr. Mangala Jyothi KJNo ratings yet
- Fixed ProsthodonticsDocument11 pagesFixed ProsthodonticsArxhenta ÇupiNo ratings yet
- 01 Đại cương tháo lắpDocument31 pages01 Đại cương tháo lắpNguyễn Thị Như NgọcNo ratings yet
- Introduction To ProsthodonticsDocument3 pagesIntroduction To ProsthodonticsArdesh abdilleNo ratings yet
- Theme 2 - Partial Acrylic Removable Denture: Maxilla LimitsDocument3 pagesTheme 2 - Partial Acrylic Removable Denture: Maxilla LimitsShany SchwarzwaldNo ratings yet
- Ortho (Lec)Document2 pagesOrtho (Lec)Leigh BelmonteNo ratings yet
- A New Fixed Acrylic Bite Plane For Deep Bite CorrectionDocument6 pagesA New Fixed Acrylic Bite Plane For Deep Bite CorrectionFisaNo ratings yet
- Lumineers M (1-5)Document5 pagesLumineers M (1-5)mm55mmaahh55No ratings yet
- Immediate DentureDocument9 pagesImmediate Dentureapi-371094867% (3)
- Unit Ii. Oral Surgery: SpeakingDocument5 pagesUnit Ii. Oral Surgery: SpeakingTolea SirghiNo ratings yet
- Immediate Denture: Advantages of Immediate DenturesDocument6 pagesImmediate Denture: Advantages of Immediate Denturesابراهيم منعم حسينNo ratings yet
- Single Complete DentureDocument33 pagesSingle Complete DentureAnjana ThomasNo ratings yet
- لمحاضره الاولى فيصل جراحهDocument9 pagesلمحاضره الاولى فيصل جراحهابو العزNo ratings yet
- Restoration of Esthetics And.... POST COREDocument6 pagesRestoration of Esthetics And.... POST COREnadeemNo ratings yet
- Prosthodontic Rehabilitation of A Patient With Maxillary Flabby Ridge - A Case ReportDocument4 pagesProsthodontic Rehabilitation of A Patient With Maxillary Flabby Ridge - A Case ReportdedeNo ratings yet
- Try in Step in Complete DentureDocument8 pagesTry in Step in Complete DentureMuhammad SdiqNo ratings yet
- Unconventional Denture (Autosaved)Document50 pagesUnconventional Denture (Autosaved)Shilpa SomanNo ratings yet
- عبد الرحمن خالد الزميلي Assighment Of Dental Surgery /Principle of routine exodontiaDocument20 pagesعبد الرحمن خالد الزميلي Assighment Of Dental Surgery /Principle of routine exodontiaعبد الرحمن خالد الزميليNo ratings yet
- Dental Anatomy: A Review: Antoinette Metivier, CDA Kimberly Bland, CDA, EFDA, M.EdDocument23 pagesDental Anatomy: A Review: Antoinette Metivier, CDA Kimberly Bland, CDA, EFDA, M.EdmarrNo ratings yet
- Overdenture VVDocument37 pagesOverdenture VVVikas Aggarwal50% (2)
- Reviewer For Perspectives in DentistryDocument3 pagesReviewer For Perspectives in DentistrySophia Aliyah Miel MacabeoNo ratings yet
- Imediate 4Document3 pagesImediate 4Alifia Ayu DelimaNo ratings yet
- Over Dentures Jan 2012Document40 pagesOver Dentures Jan 2012Mohsin HabibNo ratings yet
- Maxillofacial Prosthesis &materialsDocument7 pagesMaxillofacial Prosthesis &materialsطبطب صالحNo ratings yet
- Mouth Preparation: DR - Mona Galal Lecturer at Prosthodontics DepartmentDocument70 pagesMouth Preparation: DR - Mona Galal Lecturer at Prosthodontics DepartmentAbdelrhman AdelNo ratings yet
- 4th Grade Lec 8 Try in 2Document9 pages4th Grade Lec 8 Try in 2احمد سلامNo ratings yet
- Space MGMT PPT 38Document81 pagesSpace MGMT PPT 38AbboodNo ratings yet
- 3-Mouth PreparationDocument55 pages3-Mouth Preparationyahia salahNo ratings yet
- The Single-Tooth Implant:: A Minimally Invasive Approach for Anterior and Posterior Extraction SocketsFrom EverandThe Single-Tooth Implant:: A Minimally Invasive Approach for Anterior and Posterior Extraction SocketsNo ratings yet
- Guía Iadt 2020Document46 pagesGuía Iadt 2020Johanna Giliberto RodríguezNo ratings yet
- 2 Prostho To PrintDocument14 pages2 Prostho To PrintDENTAL REVIEWER ONLYNo ratings yet
- 9.2018.occlusal Onlays As A Modern Treatment Concept For The Reconstruction of Severely Worn Occlusal SurfacespdfDocument14 pages9.2018.occlusal Onlays As A Modern Treatment Concept For The Reconstruction of Severely Worn Occlusal Surfacespdfluis alejandroNo ratings yet
- Dr. Pitts The Protocol Clinical Article IssueDocument51 pagesDr. Pitts The Protocol Clinical Article IssueNhock LamentosNo ratings yet
- Piper Classification InfographicDocument1 pagePiper Classification InfographicJazNo ratings yet
- Deep Bite Malocclusion: Exploration of The Skeletal and Dental FactorsDocument6 pagesDeep Bite Malocclusion: Exploration of The Skeletal and Dental FactorsSofeaNo ratings yet
- Diagnosis of Transverse Problems - 2019 - Seminars in Orthodontics PDFDocument8 pagesDiagnosis of Transverse Problems - 2019 - Seminars in Orthodontics PDFOmy J. CruzNo ratings yet
- The Gothic Arch (Needle Point) Tracing and Condylar InclinationDocument5 pagesThe Gothic Arch (Needle Point) Tracing and Condylar InclinationPraveen KumarNo ratings yet
- 1 ManualDocument10 pages1 Manualwendyjemmy8gmailcomNo ratings yet
- GelbDocument6 pagesGelbAlex BernierNo ratings yet
- BPS - The Biofunctional Prosthetic System PDFDocument20 pagesBPS - The Biofunctional Prosthetic System PDFVinay PandeyNo ratings yet
- Clinical Considerations and Rationale For The Use of Simplified Instrumentation in Occlusal Rehabilitation Part 2, Stefano GracisDocument9 pagesClinical Considerations and Rationale For The Use of Simplified Instrumentation in Occlusal Rehabilitation Part 2, Stefano GracisSUSAN LUCINDA MEJIA TIPAZNo ratings yet
- Multiple Choice Questions: Fixed ProsthodonticsDocument5 pagesMultiple Choice Questions: Fixed Prosthodonticshamza waheedNo ratings yet
- The Influence of Anterior Coupling On Mandibular MovementDocument9 pagesThe Influence of Anterior Coupling On Mandibular MovementRavneet LehalNo ratings yet
- The Effects of Splinting Periodontally Compromised Removable Partial Denture Abutments On Bone Stresses: A Three-Dimensional Finite Element StudyDocument7 pagesThe Effects of Splinting Periodontally Compromised Removable Partial Denture Abutments On Bone Stresses: A Three-Dimensional Finite Element StudytovarichNo ratings yet
- Swinglock DentureDocument7 pagesSwinglock DentureLouis HutahaeanNo ratings yet
- Reduction Resto ProcedureDocument5 pagesReduction Resto ProcedureAnindyaNoviaPutriNo ratings yet
- Orthodontic Treatment of A Patient With Bilateral Congenitally Missing Maxillary Canines: The Effects of First Premolar Substitution On The Functional OutcomeDocument6 pagesOrthodontic Treatment of A Patient With Bilateral Congenitally Missing Maxillary Canines: The Effects of First Premolar Substitution On The Functional OutcomesauriuaNo ratings yet
- Denture Trouble Shooting GuideDocument5 pagesDenture Trouble Shooting Guideheri asriyadiNo ratings yet
- Refined Begg TechniqueDocument137 pagesRefined Begg Techniquejohn suryavardhanNo ratings yet
- Applsci 11 00816 v2Document16 pagesApplsci 11 00816 v2KhuleedShaikhNo ratings yet
- Orthodontic and Prosthetic Rehabilitation of Unilateral Free-End Edentulous SpaceDocument4 pagesOrthodontic and Prosthetic Rehabilitation of Unilateral Free-End Edentulous SpaceDohotariu MioaraNo ratings yet
- Welcome To Journal Club: Evolution of Occlusion and Temporomandibular DISORDER IN ORTHODONTICS: Past, Present & FutureDocument25 pagesWelcome To Journal Club: Evolution of Occlusion and Temporomandibular DISORDER IN ORTHODONTICS: Past, Present & FutureReshamIrshad100% (1)
- Functional Occlusion and The Mounting of The CastsDocument88 pagesFunctional Occlusion and The Mounting of The CastsAina SalsaNo ratings yet
- 14 PDFDocument1,474 pages14 PDFAiluul Almaa100% (2)
- Document 20220802170615Document105 pagesDocument 20220802170615ณิช กุลNo ratings yet
- 6 Keys of OcclusionDocument30 pages6 Keys of OcclusionMuzna AftabNo ratings yet
- Expanding Torque PossibilitiesDocument11 pagesExpanding Torque Possibilitiesdruzair007No ratings yet