Download as pdf or txt
You might also like
- 100 Item Exam On Fundamentals of NursingDocument14 pages100 Item Exam On Fundamentals of Nursingshark_tale0488% (43)
- A Case Study On Preterm Labor FinalDocument32 pagesA Case Study On Preterm Labor FinalNiala Almario100% (3)
- Case ScenarioDocument3 pagesCase ScenarioCathy Marie Constante100% (1)
- Soap Note 2 MminerDocument8 pagesSoap Note 2 Mminerapi-272656243100% (2)
- A Case Study On Preterm LaborDocument29 pagesA Case Study On Preterm LaborBrexRomeoQuijada84% (19)
- Case Presentation - Acute GlomerulonephritisDocument10 pagesCase Presentation - Acute GlomerulonephritisRold Brio Sos100% (1)
- Case Study #117Document4 pagesCase Study #117Cheska Paloma100% (1)
- Labor AssessmentDocument14 pagesLabor AssessmentShay DayNo ratings yet
- Plant PhysiologyDocument321 pagesPlant Physiologykamal100% (2)
- Energy For All!: Engage: Food For CornDocument4 pagesEnergy For All!: Engage: Food For CornBri LavaeNo ratings yet
- Wim Hof Method PDFDocument4 pagesWim Hof Method PDFAnonymous HsAAhXFnGp100% (12)
- Obg - Case Presentation - FGRDocument24 pagesObg - Case Presentation - FGRNazee NazreenNo ratings yet
- Patient Report. 2Document7 pagesPatient Report. 2Ahlam Azam, MohamedNo ratings yet
- Obstric History Taking, CasesDocument151 pagesObstric History Taking, CasesljilffbNo ratings yet
- Preterm ContractionDocument19 pagesPreterm ContractionAiman ArifinNo ratings yet
- Case Study Medical Surgical WardDocument7 pagesCase Study Medical Surgical WardLucil Jaine Abayan BellezaNo ratings yet
- Inter MykDocument4 pagesInter Mykkengeramacklina3No ratings yet
- MS Practical Exams Final Cases-1Document49 pagesMS Practical Exams Final Cases-1Jill murphyNo ratings yet
- Soap Note1 - Gyn ComplaintDocument6 pagesSoap Note1 - Gyn Complaintapi-482726932100% (3)
- History Taking OBS GYNDocument10 pagesHistory Taking OBS GYNzvkznhsw2tNo ratings yet
- Kampala International University:: Morebu Peter MomanyiDocument10 pagesKampala International University:: Morebu Peter Momanyifadila mohammedNo ratings yet
- CC Minggu 29 Januari 2017 (Diare Akut Morbili)Document29 pagesCC Minggu 29 Januari 2017 (Diare Akut Morbili)KrisbiyantoroAriesNo ratings yet
- NCM 214 Aquino - Case StudyDocument3 pagesNCM 214 Aquino - Case StudyYoongiNo ratings yet
- Hiv in Pregnancy FinalDocument22 pagesHiv in Pregnancy FinalMoin PandithNo ratings yet
- Case Study 117Document4 pagesCase Study 117Jonah MaasinNo ratings yet
- GDM 3Document12 pagesGDM 3Aiman ArifinNo ratings yet
- OB-GYN Soap NoteDocument9 pagesOB-GYN Soap Notealex MusingilaNo ratings yet
- Gamo - Case Write-Up (TMC OB - Pre-LR 2)Document6 pagesGamo - Case Write-Up (TMC OB - Pre-LR 2)JUAN VICTOR GAMONo ratings yet
- Case High RiskDocument18 pagesCase High RiskAya AlntshNo ratings yet
- Twin PregnancyDocument23 pagesTwin PregnancyNazee NazreenNo ratings yet
- DR Case Presentation Group 1 PIHDocument6 pagesDR Case Presentation Group 1 PIHCharles Vergel Sabaldan MarceraNo ratings yet
- Post DatismDocument10 pagesPost DatismAiman ArifinNo ratings yet
- Tizon, R. - Patient History, Gordon's, Lab Results, Drug StudyDocument10 pagesTizon, R. - Patient History, Gordon's, Lab Results, Drug StudyRoyce Vincent TizonNo ratings yet
- Ob Gyn Sample HisotryDocument4 pagesOb Gyn Sample HisotrySophia RubiaNo ratings yet
- Ong Case Sheet Sem7Document13 pagesOng Case Sheet Sem7Uchiha AnzarNo ratings yet
- Post DateDocument4 pagesPost DateRae RayNo ratings yet
- Case Summary 1 OGDocument1 pageCase Summary 1 OGYOS HANANo ratings yet
- Learning Log Proforma For Clinical Case Chronic HTNDocument8 pagesLearning Log Proforma For Clinical Case Chronic HTNAnjit PhuyalNo ratings yet
- OBG Cases-1 - 240402 - 092346Document77 pagesOBG Cases-1 - 240402 - 092346jashwanth t cNo ratings yet
- Case StudyDocument28 pagesCase Studyakoeljames8543No ratings yet
- Case Write Up 1 ANCDocument5 pagesCase Write Up 1 ANCfafa dejanNo ratings yet
- Safari - Jul 27, 2019 at 7:12 AMDocument1 pageSafari - Jul 27, 2019 at 7:12 AMKo NgeNo ratings yet
- Case Presentation 1Document9 pagesCase Presentation 1Sadiasifatafroz SifatNo ratings yet
- Case Presentation Post LSCSDocument14 pagesCase Presentation Post LSCSNazee NazreenNo ratings yet
- University of Northern Philippines: Republic of The Philippines Tamag, Vigan City, Ilocos SurDocument26 pagesUniversity of Northern Philippines: Republic of The Philippines Tamag, Vigan City, Ilocos Surneo quartoNo ratings yet
- Gamo - Case Write-Up (TMC OB - Pre-LR 1)Document7 pagesGamo - Case Write-Up (TMC OB - Pre-LR 1)JUAN VICTOR GAMONo ratings yet
- Anaemia in PregnancyDocument29 pagesAnaemia in PregnancySampritha P GNo ratings yet
- Unfolding Intrapartum Case StudyDocument9 pagesUnfolding Intrapartum Case Studyapi-726948535No ratings yet
- Anc 1 2 1Document22 pagesAnc 1 2 1Lemma AbishaNo ratings yet
- Obstetrics N Gynaecology CasesDocument21 pagesObstetrics N Gynaecology CasesMarutiNo ratings yet
- Obstetrics N Gynaecology Cases PDFDocument21 pagesObstetrics N Gynaecology Cases PDFAparna DeviNo ratings yet
- Case Write Up 2Document16 pagesCase Write Up 2Shidev100% (1)
- Module 6 Standardize Patient Postpartum StudentDocument12 pagesModule 6 Standardize Patient Postpartum StudentDaniela Claire FranciscoNo ratings yet
- Farah Cwu Gynae EditDocument16 pagesFarah Cwu Gynae EditfarahNo ratings yet
- Vicente Sotto Memorial Medical Center Department of Obstetrics & GynecologyDocument9 pagesVicente Sotto Memorial Medical Center Department of Obstetrics & GynecologyIrah FloresNo ratings yet
- English Case HIV in Pregnancy ArdeDocument48 pagesEnglish Case HIV in Pregnancy ArdeArde Hidayat100% (1)
- Antepartum Care AssignmentDocument3 pagesAntepartum Care AssignmentMattNo ratings yet
- Case Presentation: RH Negative PregnancyDocument19 pagesCase Presentation: RH Negative PregnancyNazee NazreenNo ratings yet
- 1696-Article Text-4009-1-10-20201129Document5 pages1696-Article Text-4009-1-10-20201129asmita sainiNo ratings yet
- Gestational Diabetes MellitusDocument9 pagesGestational Diabetes MellitusAiman ArifinNo ratings yet
- Draft 3-30-2024 Ob Case StudyDocument54 pagesDraft 3-30-2024 Ob Case StudyKent Jerimhe Daileg ManiaulNo ratings yet
- N. Bacalso Ave., Cebu City Philippines: Page 1 of 32Document32 pagesN. Bacalso Ave., Cebu City Philippines: Page 1 of 32Joule PeirreNo ratings yet
- Draft For Preterm LaborDocument31 pagesDraft For Preterm LaborKimberly Jose100% (1)
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- Chapter 6 Q. P.1Document28 pagesChapter 6 Q. P.1RawanMazen SharifNo ratings yet
- Reviewer in PerioperativeDocument25 pagesReviewer in PerioperativeACERET, IVAN LAURENTINE G.No ratings yet
- AntitussiveDocument7 pagesAntitussiveCucumber WarriorNo ratings yet
- 227-Article Text-1075-3-10-20220717Document16 pages227-Article Text-1075-3-10-20220717Pocut siti Umaiya rahmadiNo ratings yet
- Nervous-System Parctice-TestDocument10 pagesNervous-System Parctice-TestDhon FrondaNo ratings yet
- Human Body SystemsDocument35 pagesHuman Body SystemsSir Rannie Espanto100% (1)
- Pe Health 3 Module q1 Module 1 Claire L. Vince CruzDocument6 pagesPe Health 3 Module q1 Module 1 Claire L. Vince CruzperldeveraNo ratings yet
- Anatomy & Physiology: 5Fyucppl&Rvjuz&EjujpoDocument10 pagesAnatomy & Physiology: 5Fyucppl&Rvjuz&EjujpoRajeshwar KumdaleNo ratings yet
- ResperationDocument5 pagesResperationaishabroNo ratings yet
- Integration of MetabolismDocument40 pagesIntegration of Metabolismseada JemalNo ratings yet
- 5 Minute Biochemistry PresentationDocument23 pages5 Minute Biochemistry PresentationPITAGAN, Galda Boy 1-FNo ratings yet
- Respiratory - Gas ExchangeDocument3 pagesRespiratory - Gas ExchangeChris P. BeaconNo ratings yet
- Fleeting ObservationDocument20 pagesFleeting ObservationJERIC APORBONo ratings yet
- English Guide-Workshop #15 - 10th Grade PDFDocument13 pagesEnglish Guide-Workshop #15 - 10th Grade PDFFelipe Jeri OrjuelaNo ratings yet
- MCQ Examples Jan 2016Document30 pagesMCQ Examples Jan 2016Arshad KhanNo ratings yet
- Basic First Aid Procedures-Safety by ESPDocument4 pagesBasic First Aid Procedures-Safety by ESPLijo JohnNo ratings yet
- Principles of ECGDocument11 pagesPrinciples of ECGDeinielle Magdangal RomeroNo ratings yet
- Understanding Anatomy and Physiology A Visual Auditory Interactive Approach 2 Ed 978-0-8036 4373 4 0 8036 4373 XDocument538 pagesUnderstanding Anatomy and Physiology A Visual Auditory Interactive Approach 2 Ed 978-0-8036 4373 4 0 8036 4373 Xgusneli137No ratings yet
- NIBP-Series DatasheetDocument4 pagesNIBP-Series DatasheetChatchayMahatanoNo ratings yet
- Cardiolab: A Virtual Laboratory For The Analysis of Human Circulatory SystemDocument18 pagesCardiolab: A Virtual Laboratory For The Analysis of Human Circulatory SystemCarito PulgarinNo ratings yet
- 20 Questions HypothermiaDocument8 pages20 Questions HypothermiaManuelNo ratings yet
- Sympathetic Vs para SympatheticDocument2 pagesSympathetic Vs para SympatheticLesther Alba Dela CruzNo ratings yet
- Expermental Models For Memory ImpairmentDocument13 pagesExpermental Models For Memory ImpairmentIJAR JOURNALNo ratings yet
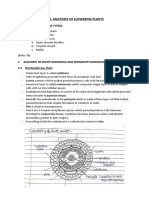
- CH6 - Anatomy of Flowering Plants - NotesDocument4 pagesCH6 - Anatomy of Flowering Plants - NotesanuminiatureNo ratings yet
- Essentials of Anatomy and PhysiologyDocument68 pagesEssentials of Anatomy and PhysiologyhamidiNo ratings yet
- Cardiac ArrestDocument64 pagesCardiac ArrestJoel Estacio100% (1)