Download as pdf or txt
You might also like
- Conference Proceedings - Vol3 - Short Paper - Final PDFDocument336 pagesConference Proceedings - Vol3 - Short Paper - Final PDFAdriana MuñozNo ratings yet
- Project Proposal DraftDocument14 pagesProject Proposal DraftAdasa EdwardsNo ratings yet
- 11 Fibro Osseous LesionsDocument22 pages11 Fibro Osseous Lesionsفراس الموسويNo ratings yet
- Oral Pathology Lec - 1Document9 pagesOral Pathology Lec - 1مصطفى محمدNo ratings yet
- Fibro Osseous LesionsDocument6 pagesFibro Osseous Lesionspxb8dhqgs9No ratings yet
- Fibro-Osseous Lesions of The JawsDocument68 pagesFibro-Osseous Lesions of The JawsAmisha SaxenaNo ratings yet
- ElMofty FibroOsseous Lesions of The Craniofacial SkeletonDocument13 pagesElMofty FibroOsseous Lesions of The Craniofacial Skeletonfabiana vasquezNo ratings yet
- Fibrous DysplasiaDocument2 pagesFibrous DysplasiaGus SwanjayaNo ratings yet
- Maxillofacial Fibro-Osseous LesionsDocument30 pagesMaxillofacial Fibro-Osseous Lesionsnaidu.harikaa15No ratings yet
- Fibroosseous LesionsDocument28 pagesFibroosseous LesionsDr'Paramjot KaurNo ratings yet
- Fibrous Dysplasia: A ReviewDocument5 pagesFibrous Dysplasia: A ReviewJuhiJahan AmanullahNo ratings yet
- Craniofacial Polyostotic FibrousDocument5 pagesCraniofacial Polyostotic FibrousFatima AliNo ratings yet
- AdsfDocument7 pagesAdsfNarito NianNo ratings yet
- Fibro-Osseus LesionsDocument56 pagesFibro-Osseus LesionsyomanNo ratings yet
- Benign Non Odontogenic Lesions - 6Document97 pagesBenign Non Odontogenic Lesions - 6Thaer ZabenNo ratings yet
- Jop 12797 PDFDocument7 pagesJop 12797 PDFNada lathifahNo ratings yet
- Fibro-Osseous Lesions A ReviewDocument4 pagesFibro-Osseous Lesions A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fibroosseous LesionsDocument17 pagesFibroosseous LesionsChampak PaulNo ratings yet
- 11-Metabolic &genetic Bone DiseasesDocument12 pages11-Metabolic &genetic Bone Diseasesفراس الموسويNo ratings yet
- Fibrous DysplasiaDocument29 pagesFibrous Dysplasiadr_adjie100% (2)
- Httpsamoodle - Su.edu - Egpluginfile.php202864mod Resourcecontent1Lecture20120 Bone20diseas20 PDFDocument7 pagesHttpsamoodle - Su.edu - Egpluginfile.php202864mod Resourcecontent1Lecture20120 Bone20diseas20 PDFtthtn6c8pbNo ratings yet
- Fibro-Osseous Lesions of Bone: Dr. Afrah Adnan Al-DelaimiDocument14 pagesFibro-Osseous Lesions of Bone: Dr. Afrah Adnan Al-DelaimiB AlhashimiNo ratings yet
- 2 5336943370080096042 PDFDocument21 pages2 5336943370080096042 PDFعبدالرحمن عبدالسلام ذنون المصريNo ratings yet
- Diseasesofboneandhistology 141211233452 Conversion Gate01Document218 pagesDiseasesofboneandhistology 141211233452 Conversion Gate01JuhiJahan AmanullahNo ratings yet
- Fibrous Dysplasia - Radiology Reference Article - RadiopaediaDocument18 pagesFibrous Dysplasia - Radiology Reference Article - RadiopaediaManuelGonzalezGaitanoNo ratings yet
- Word HereditereyDocument7 pagesWord Hereditereypxb8dhqgs9No ratings yet
- Bone DiseasesDocument191 pagesBone DiseasesDrRobin SabharwalNo ratings yet
- How Can We Diagnose and Treat Osteomyelitis of The Jaws As Early As PossibleDocument11 pagesHow Can We Diagnose and Treat Osteomyelitis of The Jaws As Early As Possiblebucomaxilofacial.hfiNo ratings yet
- 2 PDFDocument19 pages2 PDFsolikin ikinNo ratings yet
- Bone PathologyDocument103 pagesBone PathologyRubyrose Tagum100% (1)
- Fibrous Dysplasia in The Maxillo-Mandibular Region - Case ReportDocument4 pagesFibrous Dysplasia in The Maxillo-Mandibular Region - Case ReportDaud Yudhistira100% (1)
- L64 Tumor-Like Lesions of BoneDocument19 pagesL64 Tumor-Like Lesions of Bone8ht2twrg5fNo ratings yet
- Lumps and Swellings in The Jaws: Aneurysmal Bone CystDocument4 pagesLumps and Swellings in The Jaws: Aneurysmal Bone CystGokul SivaNo ratings yet
- Fibro Osseous Lesions Seminar SantoshDocument77 pagesFibro Osseous Lesions Seminar SantoshSarath MohanNo ratings yet
- 05.15.17 Bone Pathology (Atkinson) - NotesDocument8 pages05.15.17 Bone Pathology (Atkinson) - NotesDan WuiytNo ratings yet
- المستندDocument12 pagesالمستند22368717No ratings yet
- Craniofacial Fibrous DysplasiaDocument15 pagesCraniofacial Fibrous DysplasiassleosNo ratings yet
- Fibro Osseous LesionsDocument50 pagesFibro Osseous LesionsanviNo ratings yet
- Fibro Osseous LesionsDocument42 pagesFibro Osseous LesionsRose DawoudNo ratings yet
- Zamala 5-2015Document53 pagesZamala 5-2015Ah-ragab HouseNo ratings yet
- Monostotic Fibrous Dysplasia of The Mandible: Oral Health and Dental Management June 2014Document5 pagesMonostotic Fibrous Dysplasia of The Mandible: Oral Health and Dental Management June 2014Narito NianNo ratings yet
- Clinical Guidelines For The Management of Craniofacial Fibrous DysplasiaDocument20 pagesClinical Guidelines For The Management of Craniofacial Fibrous DysplasiaPhúc BùiNo ratings yet
- Radiographic Diagnosis of Fibrous Dysplasia in Maxilla: Corresponding Author: Ahmed Z. Abdelkarim, Ahmedz@hawaii - EduDocument8 pagesRadiographic Diagnosis of Fibrous Dysplasia in Maxilla: Corresponding Author: Ahmed Z. Abdelkarim, Ahmedz@hawaii - Edusolikin ikinNo ratings yet
- Zebra XX, Part 2 PDFDocument3 pagesZebra XX, Part 2 PDFRamona MateiNo ratings yet
- Información Épuli FibromatosoDocument3 pagesInformación Épuli FibromatosoDaniela IbarraNo ratings yet
- Bones & Joints Pathology 4thDocument8 pagesBones & Joints Pathology 4thlovelyc95No ratings yet
- Differential Diagnosis of Periapical Radiolucencies and RadiopacitiesDocument27 pagesDifferential Diagnosis of Periapical Radiolucencies and RadiopacitiesDerya İçözNo ratings yet
- S SunilDocument4 pagesS SunileditorompjNo ratings yet
- JCM 12 04100Document10 pagesJCM 12 04100Siri NeNo ratings yet
- Non Odontogenic Tumours of JawDocument22 pagesNon Odontogenic Tumours of JawDrMuskan AroraNo ratings yet
- Iseasesof ONE: Section I Pseudo-DiseasesDocument16 pagesIseasesof ONE: Section I Pseudo-Diseasesseunnuga93No ratings yet
- Sheet 4 (Bone Pathology)Document206 pagesSheet 4 (Bone Pathology)ardesh abdille0% (1)
- MUSKULOSKELETALDocument79 pagesMUSKULOSKELETALkhalishaNo ratings yet
- Diseases of Bone MangalaDocument246 pagesDiseases of Bone MangalaharshiniNo ratings yet
- Disorders of The BoneDocument35 pagesDisorders of The BoneAyeshaNo ratings yet
- Pa ThoDocument1 pagePa Tho022389No ratings yet
- Fibrous Dysplasia of MaxillaDocument4 pagesFibrous Dysplasia of Maxillasachender_rocksNo ratings yet
- One Tumours Fibrous Tumours: Prof. R. N .Srivastav Dr. Anil PandaDocument40 pagesOne Tumours Fibrous Tumours: Prof. R. N .Srivastav Dr. Anil PandaNaysahNo ratings yet
- Presentation ON Fibrous Dysplasia: Made by Dr. Waqas Iqbal MDS in Oral PathologyDocument47 pagesPresentation ON Fibrous Dysplasia: Made by Dr. Waqas Iqbal MDS in Oral PathologyWaqas IqbalNo ratings yet
- Fibrous Dysplasia: Kepaniteraan Klinik Senior Bagian Ilmu Bedah Orthopaedic Royal Prima MedanDocument14 pagesFibrous Dysplasia: Kepaniteraan Klinik Senior Bagian Ilmu Bedah Orthopaedic Royal Prima MedanPutraNo ratings yet
- Drug-Induced Osteonecrosis of the Jaws: How to Diagnose, Prevent, and Treat ItFrom EverandDrug-Induced Osteonecrosis of the Jaws: How to Diagnose, Prevent, and Treat ItNo ratings yet
- The Influence of Work Environment, Work Discipline and Motivation On The Performance of Civil Servants at The Ministry of Home AffairsDocument9 pagesThe Influence of Work Environment, Work Discipline and Motivation On The Performance of Civil Servants at The Ministry of Home AffairsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Automating Inequality - Virginia EubanksDocument223 pagesAutomating Inequality - Virginia EubanksTanmay100% (1)
- Helen The HR Manager: Thinks Helen Thinks The Hiring Process Should Be So Much Better-More SystematicDocument2 pagesHelen The HR Manager: Thinks Helen Thinks The Hiring Process Should Be So Much Better-More SystematicArun Kumar SatapathyNo ratings yet
- Regulating Social Media in The Global South by Zahra TakhshidDocument56 pagesRegulating Social Media in The Global South by Zahra TakhshidJosé Luis SilveroNo ratings yet
- Cpar Module-2Document26 pagesCpar Module-2Princess Shamell LaberintoNo ratings yet
- Lesson Exemplar School Grade Level Teacher Learning Area Practical Research 2 Teaching Date Quarter Teaching Time No. of DaysDocument9 pagesLesson Exemplar School Grade Level Teacher Learning Area Practical Research 2 Teaching Date Quarter Teaching Time No. of DaysJovie Bitas DaeloNo ratings yet
- STS PrelimDocument5 pagesSTS PrelimGomez Agustin LeslieNo ratings yet
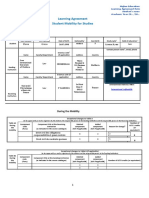
- Learning Agreement During The MobilityDocument3 pagesLearning Agreement During The MobilityVictoria GrosuNo ratings yet
- Fashion Construction SyllabusDocument7 pagesFashion Construction Syllabusapi-293881613No ratings yet
- How To Prepare A Construction Traffic Management Plan (CTMP) ReportDocument1 pageHow To Prepare A Construction Traffic Management Plan (CTMP) Reportmyco samNo ratings yet
- HTML, Javascript, XHTML & CssDocument102 pagesHTML, Javascript, XHTML & CssAmandio_DioNo ratings yet
- Covid ReportDocument1 pageCovid ReportTV UNITNo ratings yet
- Self WorthDocument5 pagesSelf WorthSav chan123No ratings yet
- Journal Pneumonia 1Document1 pageJournal Pneumonia 1dwi-148502No ratings yet
- Tokai Hit Nikon Catalog 2019Document12 pagesTokai Hit Nikon Catalog 2019Brandon LEeNo ratings yet
- We Imagine 100% Sustainable Beamhouse Systems With Stunning Leather QualityDocument2 pagesWe Imagine 100% Sustainable Beamhouse Systems With Stunning Leather QualityLuisy EncarnacionNo ratings yet
- Saeed Elseddig 4110 XA Paper 4Document16 pagesSaeed Elseddig 4110 XA Paper 4ShiawaNo ratings yet
- Grade 1 Olympiad My PDFDocument3 pagesGrade 1 Olympiad My PDFConnie Hii100% (1)
- 1 Miner: Source: University of Manchester Institute of Science and Technology (UK)Document2 pages1 Miner: Source: University of Manchester Institute of Science and Technology (UK)NI WAYAN KERTINo ratings yet
- Empower 2e B1+ Word List GermanDocument94 pagesEmpower 2e B1+ Word List GermanwaiNo ratings yet
- AMS4029MDocument5 pagesAMS4029M黄当甲No ratings yet
- 2014 JC1 H2 PH BT P2 Question SolutionDocument17 pages2014 JC1 H2 PH BT P2 Question Solutionshakthee sivakumarNo ratings yet
- Sister Margaret Beatty's CommentsDocument2 pagesSister Margaret Beatty's Commentssavannahnow.comNo ratings yet
- Imperial V DavidDocument1 pageImperial V DavidAlyssa Mae Ogao-ogaoNo ratings yet
- Below Mentioned Is The List of Mumbai Management CollegesDocument3 pagesBelow Mentioned Is The List of Mumbai Management CollegesManish SainiNo ratings yet
- Boq Grand SummaryDocument44 pagesBoq Grand Summaryelsabet gezahegnNo ratings yet
- Extrusion Compounding Process For The Development of Eco-Friendly SCG/PP Composite PelletsDocument12 pagesExtrusion Compounding Process For The Development of Eco-Friendly SCG/PP Composite PelletsVirendra RathvaNo ratings yet
- 2 Knowledge CheckDocument7 pages2 Knowledge CheckEyyEychNo ratings yet