Download as pdf or txt
You might also like
- USMLE Step 3 CCS NotesDocument20 pagesUSMLE Step 3 CCS Notesaustinhitz96% (27)
- Wolverhampton NHS Interview QuestionsDocument10 pagesWolverhampton NHS Interview QuestionsChristiana OnyinyeNo ratings yet
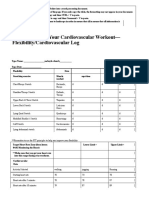
- 4.06 Recording Your Cardiovascular Workout - SchoologyDocument3 pages4.06 Recording Your Cardiovascular Workout - SchoologyMcKayla ChurchNo ratings yet
- Quality and Patient Safety ChecklistDocument7 pagesQuality and Patient Safety ChecklistKarl Roble100% (6)
- Ba GastrectomyDocument10 pagesBa GastrectomyHope3750% (2)
- Nursing InductionDocument114 pagesNursing InductionMichael Long92% (26)
- Housecalls 101: Policy and Procedure Manual for Medical Home VisitsFrom EverandHousecalls 101: Policy and Procedure Manual for Medical Home VisitsNo ratings yet
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- 0 - 16 03 24 Provincial PEWS Nursing Power Point MarchDocument30 pages0 - 16 03 24 Provincial PEWS Nursing Power Point MarchfannyNo ratings yet
- Critical Care NoteDocument10 pagesCritical Care NoteHanis Rozib99% (70)
- Haemodynamic Monitoring & Manipulation: an easy learning guideFrom EverandHaemodynamic Monitoring & Manipulation: an easy learning guideNo ratings yet
- Mikasa Ackerman Workout PDFDocument8 pagesMikasa Ackerman Workout PDFMaría100% (1)
- Sample RRTEducation Training Packet CHIDocument13 pagesSample RRTEducation Training Packet CHIReza Badruun Syahrul HakimNo ratings yet
- NCLEX ExamDocument26 pagesNCLEX ExamNaufal Fadli AmzarNo ratings yet
- TRIAGE POLICIES JuvyDocument6 pagesTRIAGE POLICIES JuvyCuyapo Infirmary Lying-In HospitalNo ratings yet
- PrioritizationDocument20 pagesPrioritizationPascal St Peter Nwaorgu100% (1)
- Introduction To Ews (Early Warning Scores) : DR Rachael Lucas Teaching Fellow Focp 2016 at SRHDocument30 pagesIntroduction To Ews (Early Warning Scores) : DR Rachael Lucas Teaching Fellow Focp 2016 at SRHPetros Akin-NibosunNo ratings yet
- JCI PresentationDocument66 pagesJCI PresentationOsama MarzoukNo ratings yet
- PEWS Training Slides March2017Document36 pagesPEWS Training Slides March2017Altama L. Sidarta100% (1)
- ESI Triage by Dr. Ryan MiranoDocument34 pagesESI Triage by Dr. Ryan MiranoEarl Kristoffer PiranteNo ratings yet
- Early Warning Scoring System (Unit 9) - 1Document6 pagesEarly Warning Scoring System (Unit 9) - 1Zharlene PadillaNo ratings yet
- TriageDocument40 pagesTriagerizka50% (2)
- Triage PDFDocument59 pagesTriage PDFagungNo ratings yet
- Diana Pefbrianti, S.Kep., NS., M.KepDocument33 pagesDiana Pefbrianti, S.Kep., NS., M.KepMursidah faNo ratings yet
- Night Float VADocument9 pagesNight Float VAkirNo ratings yet
- Sedation in Critically IllDocument32 pagesSedation in Critically IllSamantha Deshapriya100% (1)
- TriageDocument40 pagesTriagemody94546No ratings yet
- STUDENT Sepsis Rapid ReasoningDocument6 pagesSTUDENT Sepsis Rapid Reasoningghodghod123No ratings yet
- Adult Vital Sign ProtocolDocument10 pagesAdult Vital Sign ProtocolMegersa AleneNo ratings yet
- NCLEX-by SUKAWINACADocument44 pagesNCLEX-by SUKAWINACAAri WijayantiNo ratings yet
- PEWS Training IndonesiaDocument36 pagesPEWS Training IndonesiaBbenq Prasetyo100% (1)
- Hyper and Hypothyroid GuidelinesDocument51 pagesHyper and Hypothyroid GuidelinesFikar DarwisNo ratings yet
- The Triage Process: Primary Survey Vs Primary Nursing AssessmentDocument13 pagesThe Triage Process: Primary Survey Vs Primary Nursing AssessmentPingkan MuntuanNo ratings yet
- Assessment of Icu PatientDocument33 pagesAssessment of Icu PatientJRRMMC Nursing Division TWGNo ratings yet
- Advanced Cardiac Life Support (Acls) Part I: ACP 202 Module 6Document32 pagesAdvanced Cardiac Life Support (Acls) Part I: ACP 202 Module 6MoeNo ratings yet
- Implementation Guidelines For The Canadian Emergency Department Triage & Acuity Scale (CTAS)Document27 pagesImplementation Guidelines For The Canadian Emergency Department Triage & Acuity Scale (CTAS)Jery JsNo ratings yet
- Mostcommonquestionsofcbahi Azza 230211125221 89d97424Document58 pagesMostcommonquestionsofcbahi Azza 230211125221 89d97424amal.jaberNo ratings yet
- Patient With Peripheral Arterial Occlusive Disease - Student VersionDocument5 pagesPatient With Peripheral Arterial Occlusive Disease - Student VersionDarby GravinoNo ratings yet
- Patient AssesmentDocument15 pagesPatient AssesmentDyah Arum KusumaningtyasNo ratings yet
- Dr. Ugi Sugiri, SpEm - PPT OBMED PDFDocument56 pagesDr. Ugi Sugiri, SpEm - PPT OBMED PDFDaniel Aprianto SihotangNo ratings yet
- Introduction To The Use of Manchester Triage in Accident and Emergency DobbsDocument16 pagesIntroduction To The Use of Manchester Triage in Accident and Emergency Dobbsrosalyn sugayNo ratings yet
- Triage in Emergency DepartmentDocument27 pagesTriage in Emergency Departmentnaqibsakila4286No ratings yet
- SEPSIS - Admin Training InfoDocument3 pagesSEPSIS - Admin Training Infohinal5616No ratings yet
- Hypertension BPGDocument31 pagesHypertension BPGSebastian BujorNo ratings yet
- IMED-Admission Orders GuideDocument2 pagesIMED-Admission Orders GuideJamie AsheNo ratings yet
- Final - MQC Presentation-Standing OrdersDocument29 pagesFinal - MQC Presentation-Standing OrdersElisya Nurri SyaniNo ratings yet
- Volume 2 GDVs and More - Rev1 Ed6jvjDocument39 pagesVolume 2 GDVs and More - Rev1 Ed6jvjErhan ErtuçNo ratings yet
- Templates AnaDocument16 pagesTemplates AnaWilfredo DecasaNo ratings yet
- PHECC Field Guide 2011Document125 pagesPHECC Field Guide 2011Michael B. San JuanNo ratings yet
- MOCKBOARD PART 3 Answer KeyDocument23 pagesMOCKBOARD PART 3 Answer KeyJayrald CruzadaNo ratings yet
- An Internship ReDocument4 pagesAn Internship RebakohmarynoelNo ratings yet
- Perioperative Nursing CareDocument92 pagesPerioperative Nursing Caredyingangel_09No ratings yet
- Rapid Response Teams: Aishah Al-Naiem, Omar Quintanar, and Ivan TorresDocument7 pagesRapid Response Teams: Aishah Al-Naiem, Omar Quintanar, and Ivan Torresapi-348838130No ratings yet
- Update: Lipid Guidelines: Do Not Burn The CookiesDocument50 pagesUpdate: Lipid Guidelines: Do Not Burn The CookiesNilson Morales CordobaNo ratings yet
- Clinical Opiate Withdrawal ScaleDocument2 pagesClinical Opiate Withdrawal Scalegiveme mychargerNo ratings yet
- Course: Emergency Procedures and Patient Care Lecture-4Document27 pagesCourse: Emergency Procedures and Patient Care Lecture-4saba ramzanNo ratings yet
- Gen. Pre & Post-OptDocument31 pagesGen. Pre & Post-OptSaminu JabirNo ratings yet
- Prioritization LectureDocument6 pagesPrioritization LecturesamNo ratings yet
- Heart of the Field "Refresher & Nha Certification Quick Notes"From EverandHeart of the Field "Refresher & Nha Certification Quick Notes"No ratings yet
- Thyroidectomy Diet: A Beginner's 2-Week Step-by-Step Guide After Thyroid Gland Removal, With Sample Recipes and a Meal PlanFrom EverandThyroidectomy Diet: A Beginner's 2-Week Step-by-Step Guide After Thyroid Gland Removal, With Sample Recipes and a Meal PlanNo ratings yet
- JCI Accreditation Presentation 5Document48 pagesJCI Accreditation Presentation 5Osama MarzoukNo ratings yet
- JCI Accreditation Presentation 4Document53 pagesJCI Accreditation Presentation 4Osama MarzoukNo ratings yet
- JCI PresentationDocument66 pagesJCI PresentationOsama MarzoukNo ratings yet
- JCI Accreditation Presentation 2Document39 pagesJCI Accreditation Presentation 2Osama MarzoukNo ratings yet
- Internship Report On Unilever Bangladesh LimitedDocument80 pagesInternship Report On Unilever Bangladesh LimitedTanzina Tanisha Ahamed83% (6)
- Nclex Mnemonics 2020 2Document9 pagesNclex Mnemonics 2020 2Winnie OkothNo ratings yet
- WHLP - Grade 10Document21 pagesWHLP - Grade 10Sam dela CernaNo ratings yet
- Best Critical Care Injectable PCD CompaniesDocument1 pageBest Critical Care Injectable PCD Companiesseo.intelicopharmaceuticalsNo ratings yet
- Annotated BibliographyDocument5 pagesAnnotated Bibliographyapi-259924791No ratings yet
- Welcome To The Family Of: Advance Polyclinic & Path CareDocument19 pagesWelcome To The Family Of: Advance Polyclinic & Path Caredipendra kumarNo ratings yet
- Paragraph Outline Modern Society TodayDocument1 pageParagraph Outline Modern Society Todayracedemon22No ratings yet
- Summative Test in Hope 1: 2 Quarter - Week 5-8Document3 pagesSummative Test in Hope 1: 2 Quarter - Week 5-8Mylyn Mina67% (3)
- Resume Chapter 12Document3 pagesResume Chapter 12Ari IlhamNo ratings yet
- NAC Asthma COPD Meds Chart November 2020 WebDocument1 pageNAC Asthma COPD Meds Chart November 2020 WebEman ShalabyNo ratings yet
- LD - Test 1A - StudentDocument12 pagesLD - Test 1A - StudentLuu Hong NhiNo ratings yet
- NCM 107 Transes Prelim 1Document7 pagesNCM 107 Transes Prelim 1Tatel JocelleNo ratings yet
- Lesson PlanningDocument4 pagesLesson PlanningPatrice BlakeNo ratings yet
- SUR en US BOD Workout Calendar 111422Document1 pageSUR en US BOD Workout Calendar 111422ArshadNo ratings yet
- Case Study Rockland Hospital, Qutub Institutional Area, New DelhiDocument15 pagesCase Study Rockland Hospital, Qutub Institutional Area, New DelhiBruce BharathiNo ratings yet
- BON Gelati PREMIUM ICE CREAM CLASSIC - Lidl - 6 X 84 G 504g 6×120ml 720mlDocument1 pageBON Gelati PREMIUM ICE CREAM CLASSIC - Lidl - 6 X 84 G 504g 6×120ml 720mlлао нирпNo ratings yet
- Textbook Narcissism and Its Discontents Diagnostic Dilemmas and Treatment Strategies With Narcissistic Patients Glen O Gabbard Ebook All Chapter PDFDocument54 pagesTextbook Narcissism and Its Discontents Diagnostic Dilemmas and Treatment Strategies With Narcissistic Patients Glen O Gabbard Ebook All Chapter PDFdarryl.potolsky581100% (9)
- Asarnow 2021Document15 pagesAsarnow 2021Jaime YañezNo ratings yet
- Comprehensive Safety and Health Policies: Policies, Rules, Procedures, Programs, HandbooksDocument13 pagesComprehensive Safety and Health Policies: Policies, Rules, Procedures, Programs, HandbooksMart oro alNo ratings yet
- Signed Off - Physical Education11 - q1 - m3 - Health Related Fitness Components and Safety Protocols in Case of Emergency - v3Document34 pagesSigned Off - Physical Education11 - q1 - m3 - Health Related Fitness Components and Safety Protocols in Case of Emergency - v3loraine.ruadoNo ratings yet
- Role of Orthodontist in Cleft Palate Patient: Erum MinhasDocument16 pagesRole of Orthodontist in Cleft Palate Patient: Erum MinhasAhmed FarghlyNo ratings yet
- Pe ReviewerDocument2 pagesPe ReviewerKEMBERLY GARDENo ratings yet
- Nutritionist Project PlanningDocument8 pagesNutritionist Project Planningapi-572189697No ratings yet
- Motivation Factor To Undergo Cosmetic Surgery Among Thai Working Officer in Private EnterpriseDocument20 pagesMotivation Factor To Undergo Cosmetic Surgery Among Thai Working Officer in Private EnterpriseBUI THI THANH HANGNo ratings yet
- Hiv Trends Pir RHWC DavaoDocument57 pagesHiv Trends Pir RHWC DavaoIsfahan MasulotNo ratings yet
- RRL (Modern Medicine)Document3 pagesRRL (Modern Medicine)Michelle Oñas VillarealNo ratings yet
- Implikasi "Teori Hirarki Maslow" Pada Era New Normal: Ns. Sherly Amelia, S.Kep.,M.KepDocument19 pagesImplikasi "Teori Hirarki Maslow" Pada Era New Normal: Ns. Sherly Amelia, S.Kep.,M.KepSherly RamadaniNo ratings yet
- Lippincott Advisor BrochureDocument4 pagesLippincott Advisor BrochurePatrick Darmawan TaslimNo ratings yet