Download as docx, pdf, or txt
You might also like
- Крок-2 - студ - 18 - англDocument8 pagesКрок-2 - студ - 18 - англAimeeNo ratings yet
- Ischemic Stroke Case StudyDocument33 pagesIschemic Stroke Case StudyYanne Barrido89% (19)
- Glosario Inglés FisioterapiaDocument3 pagesGlosario Inglés FisioterapiaEndermar Vilchez100% (1)
- Grand Case CHF Final Na Final Na Final Na TrueDocument40 pagesGrand Case CHF Final Na Final Na Final Na Truelyndzy100% (2)
- Bipap Ventilation Basic and MonitoringDocument33 pagesBipap Ventilation Basic and MonitoringPradip ChougaleNo ratings yet
- Final Paper Rheumatic Heart DiseaseDocument16 pagesFinal Paper Rheumatic Heart DiseasePrincess TumambingNo ratings yet
- Chronicheartfailure Inolderadults: Ali AhmedDocument23 pagesChronicheartfailure Inolderadults: Ali AhmedRaul LaraNo ratings yet
- ICU CVD GroupCaseStudyDocument43 pagesICU CVD GroupCaseStudyKrizziaNo ratings yet
- Hypertension Due To Renal Artery Stenosis: Case ReportDocument6 pagesHypertension Due To Renal Artery Stenosis: Case ReportSabhina AnseliaNo ratings yet
- Case Study in Congestive Heart CHFDocument31 pagesCase Study in Congestive Heart CHFJm RomancapNo ratings yet
- Exposure To Toxic SubstancesDocument21 pagesExposure To Toxic SubstancesDavid VillanuevaNo ratings yet
- Caso FarmaDocument7 pagesCaso FarmaIdelberto Torres BenitezNo ratings yet
- Idiopathic Thrombocytopenic Purpura (ITP)Document7 pagesIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiNo ratings yet
- CaseDocument24 pagesCasecintaNo ratings yet
- Case 5: Tutor GuideDocument18 pagesCase 5: Tutor GuidelubnaNo ratings yet
- Causes of Heart FailureDocument4 pagesCauses of Heart Failurejana7-7No ratings yet
- Ujian Lokal PembahasanDocument3 pagesUjian Lokal PembahasanAdityaWigunaNo ratings yet
- Exposure To Toxic SubstancesDocument21 pagesExposure To Toxic SubstancesDavid VillanuevaNo ratings yet
- Exposure To Toxic SubstancesDocument21 pagesExposure To Toxic SubstancesDavid VillanuevaNo ratings yet
- Ejhs2901 0887Document8 pagesEjhs2901 0887Syawal DragonballNo ratings yet
- CHF RevisedDocument74 pagesCHF RevisedAbigael Patricia GutierrezNo ratings yet
- Heart Failure With Preserved Ejection Fraction - Concept, Pathophysiology, Diagnosis and Challenges For TreatmentDocument7 pagesHeart Failure With Preserved Ejection Fraction - Concept, Pathophysiology, Diagnosis and Challenges For TreatmentOngky AristianNo ratings yet
- Pat2 Med Surg 2Document19 pagesPat2 Med Surg 2api-339132978No ratings yet
- JurnalDocument12 pagesJurnalFKWNo ratings yet
- ASD Internship ReportingDocument14 pagesASD Internship ReportingPernel Jose Alam MicuboNo ratings yet
- Aplastic Anemia Case Study FINALDocument53 pagesAplastic Anemia Case Study FINALMatthew Rich Laguitao Cortes100% (6)
- Aplastic AnemiaDocument26 pagesAplastic AnemiaMark Anthony S. Castillo100% (1)
- EBSTEIN'S ANOMALY Dhini - Maju 17 Juli 2014Document29 pagesEBSTEIN'S ANOMALY Dhini - Maju 17 Juli 2014Azizi PranokoNo ratings yet
- A2 Irreg Case PreDocument43 pagesA2 Irreg Case PreJade HemmingsNo ratings yet
- Coronary Artery Disease (Metabilism)Document137 pagesCoronary Artery Disease (Metabilism)Al-nazer Azer AlNo ratings yet
- A Premature Neonate LueucicitosisDocument3 pagesA Premature Neonate Lueucicitosisgonococo29No ratings yet
- Paper - Hypoplastic Left Heart SyndromeDocument22 pagesPaper - Hypoplastic Left Heart SyndromeЈован РадојевићNo ratings yet
- GRAND TotalDocument35 pagesGRAND TotalNoveeNo ratings yet
- 30-Article Text-55-2-10-20191114Document4 pages30-Article Text-55-2-10-20191114Møhammed Amer KamelNo ratings yet
- PracticeExam 2 AnsDocument51 pagesPracticeExam 2 AnsBehrouz YariNo ratings yet
- 9 16 1 SM PDFDocument5 pages9 16 1 SM PDFjeka222No ratings yet
- Ate Joya File Until LabsDocument36 pagesAte Joya File Until LabsMoneto CasaganNo ratings yet
- Application of Hipno-Breathing Exercise On Dyspnea and Hemodynamic Status of Congestive Heart Failure PatientDocument4 pagesApplication of Hipno-Breathing Exercise On Dyspnea and Hemodynamic Status of Congestive Heart Failure Patientedo100% (1)
- Exercise Stress Test As An Antidote For Anxiety Ne PDFDocument2 pagesExercise Stress Test As An Antidote For Anxiety Ne PDFmehrshad Farahpour Gp5No ratings yet
- Nursing Management of A Patient With: HyperthyroidismDocument31 pagesNursing Management of A Patient With: Hyperthyroidismember parkNo ratings yet
- A Study of 50 Cases of Hepatorenal: Syndrome and Its OutcomeDocument16 pagesA Study of 50 Cases of Hepatorenal: Syndrome and Its OutcomeRishabh GuptaNo ratings yet
- Case Presentation of AnemiaDocument71 pagesCase Presentation of AnemiaJessica Esther Canlas100% (2)
- Acromegaly Presenting As Heart Failure by Anumah Et AlDocument3 pagesAcromegaly Presenting As Heart Failure by Anumah Et AlChikezie OnwukweNo ratings yet
- The Editor's Roundtable: Acute Decompensated Heart FailureDocument8 pagesThe Editor's Roundtable: Acute Decompensated Heart Failuredrissy7711No ratings yet
- Nursing Care Process Case StudyDocument6 pagesNursing Care Process Case StudyEunice RosalesNo ratings yet
- Dental Management of Patients With CHFDocument4 pagesDental Management of Patients With CHFarjayNo ratings yet
- Rossano2014 PDFDocument6 pagesRossano2014 PDFAditya SanjayaNo ratings yet
- Coronary Artery Disease An Example Case StudyDocument19 pagesCoronary Artery Disease An Example Case StudyrumasadraunaNo ratings yet
- Abstrak INAECHODocument21 pagesAbstrak INAECHOAgung Angga KesumaNo ratings yet
- Heart Failure in ChildrenDocument27 pagesHeart Failure in ChildrendenakarinaNo ratings yet
- Ajol-File-Journals 563 Articles 252250 64cba8c4c41a6Document9 pagesAjol-File-Journals 563 Articles 252250 64cba8c4c41a6Dr. Ashwin Raja MBBS MSNo ratings yet
- Tasks:: For StudentDocument3 pagesTasks:: For StudentlalitrajindoliaNo ratings yet
- Acute Hypotonia in An Infant (2017)Document3 pagesAcute Hypotonia in An Infant (2017)nikos.alexandrNo ratings yet
- High Yield Board ReviewDocument5 pagesHigh Yield Board ReviewMarcoNo ratings yet
- 10 Iajps10072017Document5 pages10 Iajps10072017Baru Chandrasekhar RaoNo ratings yet
- Acute Coronary SyndromeDocument43 pagesAcute Coronary SyndromeMsOrange96% (27)
- 48 Seema Mahant EtalDocument2 pages48 Seema Mahant EtaleditorijmrhsNo ratings yet
- A Twins With Congenital Heart Disease: A Case ReportDocument5 pagesA Twins With Congenital Heart Disease: A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Timothy P. Moran Patient H&P #14 CC: Bilateral Knee Pain HpiDocument4 pagesTimothy P. Moran Patient H&P #14 CC: Bilateral Knee Pain Hpistarskyhutch0000No ratings yet
- Hypertension in Children and Adolescents: New PerspectivesFrom EverandHypertension in Children and Adolescents: New PerspectivesEmpar LurbeNo ratings yet
- Cardiorenal Syndrome in Heart FailureFrom EverandCardiorenal Syndrome in Heart FailureW. H. Wilson TangNo ratings yet
- Central Nervous System Tumours of ChildhoodFrom EverandCentral Nervous System Tumours of ChildhoodEdward EstlinNo ratings yet
- 2.arteri Complication PVDocument5 pages2.arteri Complication PVNovi Yanti NyNo ratings yet
- J Jclinane 2005 08 012Document3 pagesJ Jclinane 2005 08 012Novi Yanti NyNo ratings yet
- 2014 ESC/ESA Guidelines On Non-Cardiac Surgery: Cardiovascular Assessment and ManagementDocument49 pages2014 ESC/ESA Guidelines On Non-Cardiac Surgery: Cardiovascular Assessment and ManagementNovi Yanti NyNo ratings yet
- Eappendix A. Guideline Summary For Preoperative EcgDocument7 pagesEappendix A. Guideline Summary For Preoperative EcgNovi Yanti NyNo ratings yet
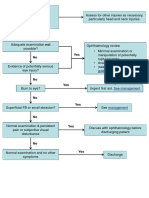
- No Yes: Penetrating Eye Injury GuidelinesDocument1 pageNo Yes: Penetrating Eye Injury GuidelinesNovi Yanti NyNo ratings yet
- Forensic Toxicological Analysis in Cyanide Poisoning Two Case ReportsDocument3 pagesForensic Toxicological Analysis in Cyanide Poisoning Two Case ReportsNovi Yanti NyNo ratings yet
- Ccalifornia Mastitis Tests Proyecto en InglesDocument10 pagesCcalifornia Mastitis Tests Proyecto en InglesERIKA DAYANA HERRERA QUIROZNo ratings yet
- Lumasiran: An Investigational Rnai Therapeutic For Primary Hyperoxaluria Type 1 (Ph1)Document1 pageLumasiran: An Investigational Rnai Therapeutic For Primary Hyperoxaluria Type 1 (Ph1)Muhammad HaneefNo ratings yet
- EPWired Magazine June Issue PDFDocument36 pagesEPWired Magazine June Issue PDFBorbála Heléna (Macika)No ratings yet
- Triad of DiseaseDocument4 pagesTriad of DiseaseThierd Cañete IIINo ratings yet
- Original Research Paper Neurosurgery: Epidemiology of Head Injury-Level 1 Taei Centre StudyDocument6 pagesOriginal Research Paper Neurosurgery: Epidemiology of Head Injury-Level 1 Taei Centre StudyArjun CVNo ratings yet
- Multiple Choice Questions For Part IVDocument18 pagesMultiple Choice Questions For Part IVTarek MohsenNo ratings yet
- Safety Data Sheet: Conbextra GPDocument3 pagesSafety Data Sheet: Conbextra GPsizmaruNo ratings yet
- HemaDocument17 pagesHemakamaluNo ratings yet
- Case Presentation On CHFDocument13 pagesCase Presentation On CHFCalingalan Hussin CaluangNo ratings yet
- Aseptic Meningitis: Exams and TestsDocument8 pagesAseptic Meningitis: Exams and TestsJoylyn Sagon VergaraNo ratings yet
- Jurnal KDPDocument5 pagesJurnal KDPRAIHAN ANUGRAHNo ratings yet
- HLTC27 Assignment 2 PlanDocument8 pagesHLTC27 Assignment 2 Planalainacaffoor1No ratings yet
- Patient Registration Form 29Document8 pagesPatient Registration Form 29Cahayastore CahayastoreNo ratings yet
- M.Phil Thesis Dr. AttiqueDocument201 pagesM.Phil Thesis Dr. Attiquedoctor attiqueNo ratings yet
- En Abbott Realtime Hiv-1: Customer Service International: Call Your Abbott RepresentativeDocument24 pagesEn Abbott Realtime Hiv-1: Customer Service International: Call Your Abbott RepresentativegdurouxNo ratings yet
- All About Insulin: Jill E. Vollbrecht, MDDocument41 pagesAll About Insulin: Jill E. Vollbrecht, MDkeylapireNo ratings yet
- Nosocomial Infections Epidemiology Prevention Control and SurveillanceDocument21 pagesNosocomial Infections Epidemiology Prevention Control and SurveillanceFelicia BulaiNo ratings yet
- Diabetes: World Journal ofDocument14 pagesDiabetes: World Journal ofdesytrilistyoatiNo ratings yet
- Activity 6 Blood Agar PlateDocument4 pagesActivity 6 Blood Agar PlateNico LokoNo ratings yet
- Keating Local and Regional Anesthesia in Small AnimalsDocument16 pagesKeating Local and Regional Anesthesia in Small AnimalsDrMohd IQbal SoFiNo ratings yet
- SPINAL CORD SYNDROMES by Dr. Monday Jacob ZaccheausDocument84 pagesSPINAL CORD SYNDROMES by Dr. Monday Jacob ZaccheausDr. Amb. Monday ZaccheausNo ratings yet
- English PretestDocument11 pagesEnglish PretestSuchon KeeratisuntornNo ratings yet
- The Epidemiology of Epilepsy: ReviewDocument7 pagesThe Epidemiology of Epilepsy: ReviewArnaldo Pérez SellésNo ratings yet
- FIFe Breeding & Registration RulesDocument30 pagesFIFe Breeding & Registration RulesHimNo ratings yet
- J. P. Rizal ST., San Vicente East, Calapan CityDocument27 pagesJ. P. Rizal ST., San Vicente East, Calapan CityEinjhel Gaverielle ReyesNo ratings yet
- Reseach (Case Study)Document25 pagesReseach (Case Study)salahnaser9999No ratings yet
- Lumbar Compression Fracture: A Case StudyDocument46 pagesLumbar Compression Fracture: A Case StudyOlivia SolomonNo ratings yet
- DUMMYZ005 : LPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Document2 pagesDUMMYZ005 : LPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Yatin VermaNo ratings yet