Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- What Is Metabolic AbsorptionDocument9 pagesWhat Is Metabolic AbsorptionAmber Nicole Hubbard100% (5)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- AMPATH Nepal RFP 2024Document12 pagesAMPATH Nepal RFP 2024hamrovisionnewsNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lit 1 - CooperDocument3 pagesLit 1 - CooperSanjeev KushwahaNo ratings yet
- Case Study 2Document5 pagesCase Study 2Sanjeev KushwahaNo ratings yet
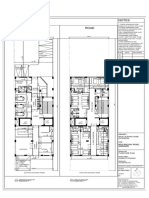
- Nursing Home - R1-FO + COLUMN LAYOUTDocument1 pageNursing Home - R1-FO + COLUMN LAYOUTSanjeev KushwahaNo ratings yet
- Nursing Home - R1-FURNITUREDocument1 pageNursing Home - R1-FURNITURESanjeev KushwahaNo ratings yet
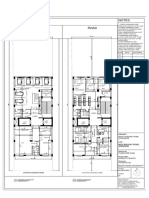
- Nursing Home - R1-SF + TFDocument1 pageNursing Home - R1-SF + TFSanjeev KushwahaNo ratings yet
- Cambridge International General Certificate of Secondary EducationDocument16 pagesCambridge International General Certificate of Secondary EducationRay PeramathevanNo ratings yet
- 07 Feb 2023 MODUS OPERANDI FOR THE TREATMENT OF FROZEN SHOULDER: A NOVEL APPROACHDocument3 pages07 Feb 2023 MODUS OPERANDI FOR THE TREATMENT OF FROZEN SHOULDER: A NOVEL APPROACHIJAR JOURNALNo ratings yet
- PrepGenie GAMSAT Full Length TestDocument77 pagesPrepGenie GAMSAT Full Length TestRebekahNo ratings yet
- Handout 4 Unit 1 ReadingDocument3 pagesHandout 4 Unit 1 Readingwilfrido barrios cordobaNo ratings yet
- Clinical DeathDocument2 pagesClinical DeathIoNo ratings yet
- Tugas Bu Lala NewDocument41 pagesTugas Bu Lala Newafra faNo ratings yet
- Benfotiamine Inhibits Intracellular Formation of Advanced Glycation End Products in VivoDocument1 pageBenfotiamine Inhibits Intracellular Formation of Advanced Glycation End Products in VivokoesantoNo ratings yet
- AgustusDocument43 pagesAgustusGunawanNo ratings yet
- According To GreenDocument2 pagesAccording To Greencate karanjaNo ratings yet
- Infografía InglesDocument1 pageInfografía InglesSarahi VazquezNo ratings yet
- Fatima Ishaq Adam MLT Project CompleteDocument37 pagesFatima Ishaq Adam MLT Project CompleteCapitallink cafeNo ratings yet
- Effectiveness of Statin Therapy in Ischemic Post Stroke PatientsDocument6 pagesEffectiveness of Statin Therapy in Ischemic Post Stroke Patientsvhania baniNo ratings yet
- Rishabh Letter Draft-1Document2 pagesRishabh Letter Draft-1Rishabh AgarwalNo ratings yet
- Kamus KesehatanDocument19 pagesKamus KesehatanJaisyullah Rafiul IslamNo ratings yet
- Classification and Coding of NeoplasmsDocument18 pagesClassification and Coding of NeoplasmsNajmul HasanNo ratings yet
- Audio Drama Risk AssessmentDocument1 pageAudio Drama Risk Assessmentapi-548670866No ratings yet
- Nursing Care of The Client With High-Risk Labor Delivery Her FamilyDocument135 pagesNursing Care of The Client With High-Risk Labor Delivery Her Familycoosa liquorsNo ratings yet
- Preparation of Soaps by Using Various Oil and Analyse Their VirtuesDocument9 pagesPreparation of Soaps by Using Various Oil and Analyse Their VirtuesSM BarathNo ratings yet
- Alternative FeedingDocument36 pagesAlternative FeedingEula Angelica OcoNo ratings yet
- Final ResearchDocument23 pagesFinal ResearchDesayNo ratings yet
- 4 ExamDocument7 pages4 Examjacynda linsanganNo ratings yet
- Winter Teacher Doc LFSC Grade 12 2023 FinalDocument23 pagesWinter Teacher Doc LFSC Grade 12 2023 FinalangelkhensaneNo ratings yet
- Active Assisted and Passive Movement in TreatmentDocument4 pagesActive Assisted and Passive Movement in TreatmentshravaniNo ratings yet
- HSV1 HSV2 R-Gene & VZV R-GeneDocument2 pagesHSV1 HSV2 R-Gene & VZV R-GeneSachinNo ratings yet
- Transferring Between Bed and ChairDocument3 pagesTransferring Between Bed and ChairKceey Cruz100% (1)
- Principles of Antimicrobial TherapyDocument12 pagesPrinciples of Antimicrobial TherapyAnne Abejuela ObialNo ratings yet
- Part I: Demographic ProfileDocument5 pagesPart I: Demographic ProfileThe ArtistNo ratings yet
- Uniece Fennell AutopsyDocument7 pagesUniece Fennell AutopsySarahNo ratings yet