Download as pdf or txt
You might also like
- Parabolas: Identify The Vertex, Focus, Axis of Symmetry, and Directrix of Each. Then Sketch The GraphDocument4 pagesParabolas: Identify The Vertex, Focus, Axis of Symmetry, and Directrix of Each. Then Sketch The GraphjaywarvenNo ratings yet
- Argumentative Essay About Getting Covid-19 VaccinesDocument2 pagesArgumentative Essay About Getting Covid-19 VaccinesMary Grace R. Ella100% (3)
- Worksheet - Graphing Sine and CosineDocument4 pagesWorksheet - Graphing Sine and CosineRudi BerlianNo ratings yet
- KernelDocument81 pagesKernelEdgar MarcaNo ratings yet
- Module 4 ActivityDocument2 pagesModule 4 Activityjermenbalatero333No ratings yet
- June Exam: Part III: Section I: Open Response - Answer The Questions in The Space ProvidedDocument3 pagesJune Exam: Part III: Section I: Open Response - Answer The Questions in The Space ProvidedrmhacheyNo ratings yet
- MHF4U Unit 1 Notes With SolutionsDocument31 pagesMHF4U Unit 1 Notes With SolutionsTony ParkNo ratings yet
- Circles Activity SheetDocument2 pagesCircles Activity SheetTeejay JimenezNo ratings yet
- Transformation of A Radical FunctionDocument2 pagesTransformation of A Radical FunctionAnamaria Alarcon-MejiaNo ratings yet
- Printable Dotted Letter X Tracing PDF WorksheetDocument1 pagePrintable Dotted Letter X Tracing PDF WorksheetFariha Muhammad AliNo ratings yet
- 10 - 4 - HyperbolasDocument4 pages10 - 4 - HyperbolasSUNGMIN CHOINo ratings yet
- Evaluating Definite Integrals PDFDocument3 pagesEvaluating Definite Integrals PDFJose Barrera GaleraNo ratings yet
- Active X Passive Voice ExercíciosDocument2 pagesActive X Passive Voice ExercíciosAline MitieNo ratings yet
- Dha CorrectionsDocument715 pagesDha Correctionsmohamad kansoNo ratings yet
- Exponential Function GraphsDocument2 pagesExponential Function GraphsMelony KimNo ratings yet
- 1998msce PS PaperDocument6 pages1998msce PS PaperAlfred MwayutaNo ratings yet
- Direct VariationDocument4 pagesDirect VariationDNo ratings yet
- Exponential Function Graphs - KEYDocument4 pagesExponential Function Graphs - KEYMelony KimNo ratings yet
- Ellipses WorksheetDocument1 pageEllipses WorksheetERVIN DANCANo ratings yet
- 10 - EllipsesDocument4 pages10 - EllipsesJasarine CabigasNo ratings yet
- Mica GandaDocument1 pageMica GandaKennevic Dela PeñaNo ratings yet
- 02 - Graphs of Polynomial FunctionsDocument4 pages02 - Graphs of Polynomial FunctionsKristine HensonNo ratings yet
- Background Reading 1 State PricesDocument13 pagesBackground Reading 1 State PricesMSNo ratings yet
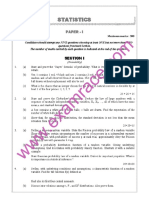
- IAS Mains Statistics 1991Document8 pagesIAS Mains Statistics 1991biltu majiNo ratings yet
- Whimsical Witch Hat FINALDocument15 pagesWhimsical Witch Hat FINALLes Mondes de Lundazepa100% (5)
- Matteo Fontana PortfolioDocument25 pagesMatteo Fontana PortfolioMatteo FontanaNo ratings yet
- Grade 7 Algebra ActivityDocument4 pagesGrade 7 Algebra Activityyt premNo ratings yet
- 1713333267-MCV 4U OVS Unit 3 Test C Fixed Curve SketchingDocument5 pages1713333267-MCV 4U OVS Unit 3 Test C Fixed Curve Sketching1sonirudNo ratings yet
- 04 - 6 - Inverse Trig FunctionsDocument4 pages04 - 6 - Inverse Trig FunctionsSUNGMIN CHOINo ratings yet
- Our Environment Class 10 NotesDocument8 pagesOur Environment Class 10 NotesChetan BhardwajNo ratings yet
- Graphing Quadratic Functions: y X y XDocument2 pagesGraphing Quadratic Functions: y X y XDessie McKinneyNo ratings yet
- Graphing Quadratic Functions 1 2Document2 pagesGraphing Quadratic Functions 1 2qshshw11No ratings yet
- Lesson 21 - 10 French AdjectivesDocument3 pagesLesson 21 - 10 French AdjectivesVincent DurrenbergerNo ratings yet
- 03 - Graphing LogarithmsDocument4 pages03 - Graphing LogarithmsKirk PolkaNo ratings yet
- Estimateaart 1801 WilliamrobbDocument1 pageEstimateaart 1801 Williamrobbapi-501783987No ratings yet
- Geography ch1 Test (Series)Document7 pagesGeography ch1 Test (Series)RangoliNo ratings yet
- 2.3: Trigonometric Substitution: Integrals Involving XDocument1 page2.3: Trigonometric Substitution: Integrals Involving Xfuriouslighning1929No ratings yet
- 10 - 1 - ParabolasDocument4 pages10 - 1 - ParabolasSUNGMIN CHOINo ratings yet
- Parabolas: Identify The Vertex, Focus, Axis of Symmetry, and Directrix of Each. Then Sketch The GraphDocument4 pagesParabolas: Identify The Vertex, Focus, Axis of Symmetry, and Directrix of Each. Then Sketch The Graphsyd ricafortNo ratings yet
- Parabolas: Identify The Vertex, Focus, Axis of Symmetry, and Directrix of Each. Then Sketch The GraphDocument4 pagesParabolas: Identify The Vertex, Focus, Axis of Symmetry, and Directrix of Each. Then Sketch The Graphsyd ricafortNo ratings yet
- Tema 6 - Derivación DiscretaDocument5 pagesTema 6 - Derivación DiscretaLuyi WangNo ratings yet
- Problem - Solution - Fit Sample TemplateDocument2 pagesProblem - Solution - Fit Sample TemplateSRIRAM S BNo ratings yet
- TMP 9 FA0Document7 pagesTMP 9 FA0FrontiersNo ratings yet
- Banu Subramaniam - Ghost Stories For Darwin - The Science of Variation and The Politics of Diversity-University of Illinois Press (2014)Document297 pagesBanu Subramaniam - Ghost Stories For Darwin - The Science of Variation and The Politics of Diversity-University of Illinois Press (2014)Julieta ChaparroNo ratings yet
- Matrix-Vector Operations: 4.1 Opening RemarksDocument40 pagesMatrix-Vector Operations: 4.1 Opening RemarksutaNo ratings yet
- Domain and Range HWDocument1 pageDomain and Range HWSalma RajabNo ratings yet
- Parametric EquationsDocument4 pagesParametric EquationsJahangeer0% (1)
- Lec 12 Edge DetectionDocument22 pagesLec 12 Edge DetectionIqrakhanNo ratings yet
- Study of Natural Fibers As An Admixture For Concrete Mix DesignDocument9 pagesStudy of Natural Fibers As An Admixture For Concrete Mix DesignJOHN FHILIP ORIT67% (3)
- Manhattan Policeman Lesson PlanDocument5 pagesManhattan Policeman Lesson Planphillochray5473No ratings yet
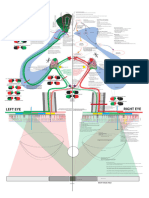
- Vision PhysiologyDocument1 pageVision PhysiologyOscar Orengo AlbertorioNo ratings yet
- A2 Semester 2 Review AnswersDocument4 pagesA2 Semester 2 Review AnswersrvmacroNo ratings yet
- Var AlgDocument7 pagesVar Algyasir.nawaz.mathsNo ratings yet
- Annotated-Exam 2 - 2020 Nashir JanmohamedDocument5 pagesAnnotated-Exam 2 - 2020 Nashir JanmohamedNashir JanmohamedNo ratings yet
- MHF4U Exam ReviewDocument6 pagesMHF4U Exam ReviewBrooke McBride-GeenNo ratings yet
- ដោះស្រាយវិសមីការតាមក្រាបដឺក្រេទី២Document2 pagesដោះស្រាយវិសមីការតាមក្រាបដឺក្រេទី២Sothea LyNo ratings yet
- MPM2DZ Exam ReviewDocument19 pagesMPM2DZ Exam Reviewashlee.lai10No ratings yet
- The LATEX Graphics Companion: Tools and Techniques for Computer TypesettingFrom EverandThe LATEX Graphics Companion: Tools and Techniques for Computer TypesettingRating: 3.5 out of 5 stars3.5/5 (18)
- Songs Without Words: Selection for piano lessonsFrom EverandSongs Without Words: Selection for piano lessonsRating: 5 out of 5 stars5/5 (1)
- Nursing CareDocument4 pagesNursing CareNdupan PandoersNo ratings yet
- NCP For AsthmaDocument2 pagesNCP For AsthmawaadNo ratings yet
- Risks of Self-Medication PracticesDocument6 pagesRisks of Self-Medication PracticesНиколаи ИвановNo ratings yet
- Rubrics Normal DeliveryDocument3 pagesRubrics Normal DeliveryLia TuazonNo ratings yet
- Dissertations of National Postgraduate Medical College of NigeriaDocument231 pagesDissertations of National Postgraduate Medical College of NigeriaErnest Omorose OsemwegieNo ratings yet
- ThyroidDocument12 pagesThyroidAliza Latif AftabNo ratings yet
- Severe Thoracic Kyphosis in The Older PatientDocument9 pagesSevere Thoracic Kyphosis in The Older PatientshivnairNo ratings yet
- Anaphylactic ShockDocument11 pagesAnaphylactic ShockBushra NaeemNo ratings yet
- Nursing Pharma ExamDocument2 pagesNursing Pharma ExamteabagmanNo ratings yet
- Basinger Abraham - ConsultationDocument80 pagesBasinger Abraham - ConsultationVikas NairNo ratings yet
- IV Fluid TherapyDocument48 pagesIV Fluid TherapyRonaldoNo ratings yet
- GK MCQ: Biology:: Gurudwara Road Model Town, Hisar 9729327755Document38 pagesGK MCQ: Biology:: Gurudwara Road Model Town, Hisar 9729327755megarebelNo ratings yet
- Laboratory Flow Sheet: Hematology Blood ChemistryDocument2 pagesLaboratory Flow Sheet: Hematology Blood ChemistrytrialqwNo ratings yet
- Doh ProgramsDocument7 pagesDoh ProgramsFatima Grace EchemNo ratings yet
- Thiotres Inj Tab LBLDocument4 pagesThiotres Inj Tab LBLDr Manish khabraniNo ratings yet
- Tips Spine-Surgery PDFDocument157 pagesTips Spine-Surgery PDFkleazevNo ratings yet
- Cutaneous Leishmania: Dr. Vijayakumar Unki Asst Professor VCGDocument16 pagesCutaneous Leishmania: Dr. Vijayakumar Unki Asst Professor VCGLohith MCNo ratings yet
- Adult Body Mass Index Bmi ChartDocument2 pagesAdult Body Mass Index Bmi ChartMyo Kyaw KyawNo ratings yet
- Bordetella SPPDocument19 pagesBordetella SPPsafilora0% (1)
- Dilution of Mida GTN AdenosineDocument94 pagesDilution of Mida GTN AdenosinenizamNo ratings yet
- Tuv Rheinland TD Guidance Ivdr Annex A enDocument27 pagesTuv Rheinland TD Guidance Ivdr Annex A ensgpconsultancykpmNo ratings yet
- AbPsych Board Exams 2 05.27.2015Document17 pagesAbPsych Board Exams 2 05.27.2015SteffiNo ratings yet
- Complications of Arteriovenous Fistula in Dialysis Patients.Document9 pagesComplications of Arteriovenous Fistula in Dialysis Patients.Renov BaligeNo ratings yet
- Splint and TractionsDocument40 pagesSplint and Tractionsakheel ahammed100% (1)
- Clinical EnzymologyDocument28 pagesClinical EnzymologySparrowNo ratings yet
- Anatomy McqsDocument3 pagesAnatomy McqsMunazzaNo ratings yet
- Alpha-2 Adrenergic Agonists As Analgesics 2002Document8 pagesAlpha-2 Adrenergic Agonists As Analgesics 2002Reginaldo CunhaNo ratings yet
- NPC Immunotherapy (Corey Smith)Document7 pagesNPC Immunotherapy (Corey Smith)fitrianyNo ratings yet
- Caries Risk Assessment Form (Age 0-6) : Contributing Conditions Check or Circle The Conditions That ApplyDocument2 pagesCaries Risk Assessment Form (Age 0-6) : Contributing Conditions Check or Circle The Conditions That ApplyMissyNo ratings yet