
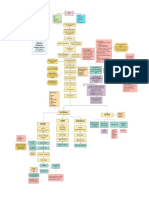
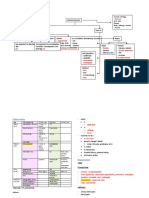
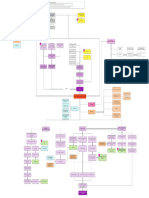
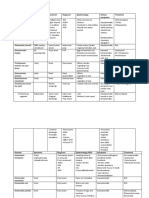
Stomach Cancer Concept Map
Stomach Cancer Concept Map
You might also like
- Utrecht Gender Dysphoria Scale PDFDocument16 pagesUtrecht Gender Dysphoria Scale PDFTherese EspinosaNo ratings yet
- Obesity Research PaperDocument10 pagesObesity Research PaperPaige-Hill88% (16)
- Syndromic Gastric PolypsDocument15 pagesSyndromic Gastric PolypsTheDrakairNo ratings yet
- Concept Map On Renal FailureDocument1 pageConcept Map On Renal FailureJessilda Damian VeranoNo ratings yet
- The Social Dilemma ReviewDocument5 pagesThe Social Dilemma ReviewNikkaDablio100% (1)
- Health and Fitness in Senior Years: Group MembersDocument35 pagesHealth and Fitness in Senior Years: Group MembersSiti Halimatus Saadiah100% (1)
- 0304 ConsultantoncallDocument4 pages0304 Consultantoncallnessimmounir1173No ratings yet
- Lacpacan Breast Cancer Concept MapDocument1 pageLacpacan Breast Cancer Concept MapRIZI LACPACANNo ratings yet
- Group D Members:: Kidney Liver PancreasDocument1 pageGroup D Members:: Kidney Liver PancreasCourtney KateNo ratings yet
- Pediatric Therapeutics: Eximius 2021Document13 pagesPediatric Therapeutics: Eximius 2021Isabel CastilloNo ratings yet
- Genome Poster 2009Document1 pageGenome Poster 2009ISAAC LEWNo ratings yet
- Gems Opt Select Brochure 2021 v6 3Document2 pagesGems Opt Select Brochure 2021 v6 3Bongani West VuthaNo ratings yet
- Week 3 - Amoeba - SarcodinaDocument14 pagesWeek 3 - Amoeba - SarcodinaShine CalarananNo ratings yet
- 5sample - Gastrointestinal System Notes - 3rd Ed OptimizedDocument28 pages5sample - Gastrointestinal System Notes - 3rd Ed OptimizedAlexis Tobar100% (2)
- GDM PathophysiologyDocument2 pagesGDM PathophysiologyShahina ShayneNo ratings yet
- HZ SummaryDocument1 pageHZ SummaryPratzNo ratings yet
- All Charts Final Exam 1 PDFDocument294 pagesAll Charts Final Exam 1 PDFYasir RasoolNo ratings yet
- Azathioprine Drug StudyDocument1 pageAzathioprine Drug StudyAlexa Lexington Rae Zagado100% (1)
- Gynaecology Revision PDFDocument13 pagesGynaecology Revision PDFAadhi AadhiNo ratings yet
- DRUGDocument4 pagesDRUGPINKI DEBNo ratings yet
- Tables ProtozoaDocument14 pagesTables ProtozoaJanette Monica BarriosNo ratings yet
- Poster Caitlin BrennanDocument1 pagePoster Caitlin Brennansagun maharjanNo ratings yet
- Medical Prefixes and SuffixesDocument12 pagesMedical Prefixes and SuffixesKrishnanunni KLNo ratings yet
- Severe: Severe Persis4ng Symptoms of One or More Of: Gastrointes Nal SkinDocument2 pagesSevere: Severe Persis4ng Symptoms of One or More Of: Gastrointes Nal SkinSanjuy GarzaNo ratings yet
- Chapter 5Document23 pagesChapter 5ozmanNo ratings yet
- Week 2 (Lec-Lab) Mls 306 Clinical Parasitology Bsmls 3A: Ascaris LumbricoidesDocument4 pagesWeek 2 (Lec-Lab) Mls 306 Clinical Parasitology Bsmls 3A: Ascaris LumbricoidesHannah Beatrice Adame TamayoNo ratings yet
- Colorect: Patient's Name: F.V Age: 64 Years OldDocument3 pagesColorect: Patient's Name: F.V Age: 64 Years OldGenynne Ragasa100% (1)
- Biowords v2Document3 pagesBiowords v2Hiezeyl Ymana GuntangNo ratings yet
- Drug To Xi CitiesDocument1 pageDrug To Xi CitiesGIST (Gujarat Institute of Science & Technology)No ratings yet
- Trematodes ScheduleDocument1 pageTrematodes ScheduleDr-positive EnergyNo ratings yet
- Diarrhoea-Vomiting Pathway-Primary Care MAY 2015Document2 pagesDiarrhoea-Vomiting Pathway-Primary Care MAY 2015nimraNo ratings yet
- 2 1 Chemistry and Pharmacology of Anticancer Drugs - Docx-8-13Document6 pages2 1 Chemistry and Pharmacology of Anticancer Drugs - Docx-8-13A HNo ratings yet
- Viii. PathophysiologyDocument2 pagesViii. Pathophysiologymacedon145377No ratings yet
- Chapter54 Management of Patients With Kidney DisordersDocument40 pagesChapter54 Management of Patients With Kidney Disordersjericho dinglasanNo ratings yet
- Approach To Abdominal PainDocument4 pagesApproach To Abdominal PainShamen KohNo ratings yet
- HISTORY & EXAMINATION Edited 228Document11 pagesHISTORY & EXAMINATION Edited 228Saurabh LamkhadeNo ratings yet
- 01 Sick Bird SyndromeDocument1 page01 Sick Bird SyndromeAli BakNo ratings yet
- MUGOT - DEMENTIA CONCEPT MAP - Page 3Document1 pageMUGOT - DEMENTIA CONCEPT MAP - Page 3MICHELLIN VAN MUGOTNo ratings yet
- Gastrointestinal DisordersDocument4 pagesGastrointestinal DisordersJerica Mae VenoyaNo ratings yet
- T2 DM Seizure 1Document1 pageT2 DM Seizure 1Mika SaldanaNo ratings yet
- Hypoparathyroidism Care MapDocument1 pageHypoparathyroidism Care MapDeo FactuarNo ratings yet
- Ashap Medical Terminology Chapter 1Document1 pageAshap Medical Terminology Chapter 1Lorelyn FabrigarasNo ratings yet
- Legend: PathophysiologyDocument1 pageLegend: PathophysiologyMikhail LamayoNo ratings yet
- Algorithm 2: Diarrhea: Signalment/History/Exam Polyuria DiarrheaDocument1 pageAlgorithm 2: Diarrhea: Signalment/History/Exam Polyuria DiarrheaAli BakNo ratings yet
- NUR 3032 Pancreatic, Biliary, and Hepatic Disorders Study PlanDocument6 pagesNUR 3032 Pancreatic, Biliary, and Hepatic Disorders Study PlanThalia FortuneNo ratings yet
- Bacteria Chart FINAL 3 2Document32 pagesBacteria Chart FINAL 3 2Йеша Маниш МираниNo ratings yet
- Drug Study FormDocument4 pagesDrug Study FormRhea LaplanaNo ratings yet
- Pi Is 0923753419544970Document6 pagesPi Is 0923753419544970AyeshaNo ratings yet
- Pancreatitis Aguda Guías ClínicasDocument1 pagePancreatitis Aguda Guías Clínicaslbritez7No ratings yet
- DRUG - NDocument1 pageDRUG - NaizatiangcoNo ratings yet
- A3 Plant KingdomDocument1 pageA3 Plant KingdomMeenakshi VermaNo ratings yet
- Skema AnalisaDocument2 pagesSkema AnalisaAhmad MukhlisNo ratings yet
- Histopathological Features in Anemia DisordersDocument1 pageHistopathological Features in Anemia Disorderskoki74No ratings yet
- Drug Study Camillus MabiniDocument5 pagesDrug Study Camillus MabiniJonh Carlo LopezNo ratings yet
- Parasites High YoieldDocument4 pagesParasites High Yoieldnreena aslamNo ratings yet
- Animals Study Guide - Yeshen a. (2-4)Document5 pagesAnimals Study Guide - Yeshen a. (2-4)krisamikaela1123No ratings yet
- NoteDocument9 pagesNote65O6O78 ฐิติพันธ์ เพชรกระจายแสงNo ratings yet
- Endocrine SystemDocument1 pageEndocrine SystemMuhammad Jefri LukmanNo ratings yet
- PGI Reyes StomachDocument124 pagesPGI Reyes StomachMark ReyesNo ratings yet
- AmebasDocument3 pagesAmebasNaomi NicoleNo ratings yet
- Bacteriology 1: - Non MotileDocument27 pagesBacteriology 1: - Non MotileYeshaa MiraniNo ratings yet
- En DoDocument2 pagesEn Dofatima_antonioNo ratings yet
- Geriatric Nursing: Trends and IssuesDocument11 pagesGeriatric Nursing: Trends and IssuesNikkaDablioNo ratings yet
- OB WorkbookDocument13 pagesOB WorkbookNikkaDablioNo ratings yet
- Geriatric Nursing: Theories of AgingDocument4 pagesGeriatric Nursing: Theories of AgingNikkaDablioNo ratings yet
- TFN - BennerDocument1 pageTFN - BennerNikkaDablioNo ratings yet
- Geriatric Nursing: Physiologic ChangesDocument25 pagesGeriatric Nursing: Physiologic ChangesNikkaDablioNo ratings yet
- Nursing Care Plan For Patients With Pneumonia and Pulmonary EmbolismDocument5 pagesNursing Care Plan For Patients With Pneumonia and Pulmonary EmbolismNikkaDablioNo ratings yet
- 19th Century RizalDocument2 pages19th Century RizalNikkaDablioNo ratings yet
- PsoriasisDocument27 pagesPsoriasisNikkaDablioNo ratings yet
- Sihay - Ang Silid NG BuhayDocument5 pagesSihay - Ang Silid NG BuhayNikkaDablio100% (1)
- Nikka Dablio - ACTIVITY 1 The Paradox of Our TimeDocument1 pageNikka Dablio - ACTIVITY 1 The Paradox of Our TimeNikkaDablioNo ratings yet
- Central Mindanao University: Department of BiologyDocument4 pagesCentral Mindanao University: Department of BiologyNikkaDablioNo ratings yet
- Datasheet On Factors Affecting BuffersDocument14 pagesDatasheet On Factors Affecting BuffersNikkaDablioNo ratings yet
- Map of Region IIIDocument8 pagesMap of Region IIINikkaDablioNo ratings yet
- Saudi Arabia Written ReportDocument3 pagesSaudi Arabia Written ReportNikkaDablioNo ratings yet
- Patterns of StrugglesDocument2 pagesPatterns of StrugglesNikkaDablioNo ratings yet
- Vijaya DiagnosticsDocument3 pagesVijaya DiagnosticssampathNo ratings yet
- Women The Skilled Architect of The SocietyDocument4 pagesWomen The Skilled Architect of The SocietyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Orthodontic Space Closure Using Simple Mechanics in Compromised First Molar Extraction Spaces: Case SeriesDocument9 pagesOrthodontic Space Closure Using Simple Mechanics in Compromised First Molar Extraction Spaces: Case SeriesHabeeb AL-AbsiNo ratings yet
- 2048 Wal LA Clarification Deficiency CA FSHC PKTDocument7 pages2048 Wal LA Clarification Deficiency CA FSHC PKTJuliana GallardoNo ratings yet
- Resume of DR Pramod Nanda - Manager in Health Care Professional 2021Document10 pagesResume of DR Pramod Nanda - Manager in Health Care Professional 2021Dr Pramod NandaNo ratings yet
- The Paediatric Voice Clinic: Ian Smillie, Kirsy Mcmanus, Wendy Cohen, Elizabeth Lawson, David Macgregor WynneDocument5 pagesThe Paediatric Voice Clinic: Ian Smillie, Kirsy Mcmanus, Wendy Cohen, Elizabeth Lawson, David Macgregor WynneCarolina UrrutiaNo ratings yet
- Pilar College of Zamboanga City, IncDocument14 pagesPilar College of Zamboanga City, IncIvy VillalobosNo ratings yet
- Alternative FeedingDocument36 pagesAlternative FeedingEula Angelica OcoNo ratings yet
- History of MedicineDocument24 pagesHistory of MedicineРоман КравецьNo ratings yet
- Cleft Lip Palate TherapyDocument5 pagesCleft Lip Palate TherapyNathalieCaracaNo ratings yet
- English Project 2Document34 pagesEnglish Project 2HARSHNo ratings yet
- OralcholecystographyDocument13 pagesOralcholecystographySuman PokhrelNo ratings yet
- FS Nicotine Mouth SprayDocument11 pagesFS Nicotine Mouth SprayAdnan DugonjicNo ratings yet
- 06 AQU347 Course Notes Chapter 1Document13 pages06 AQU347 Course Notes Chapter 1Nurul Syafiqah Binti ShaidanNo ratings yet
- PDF Hypertension A Companion To Braunwalds Heart Disease 3Rd Edition George L Bakris Ebook Full ChapterDocument53 pagesPDF Hypertension A Companion To Braunwalds Heart Disease 3Rd Edition George L Bakris Ebook Full Chapteriris.russell843100% (3)
- Antimicrobial Drugs: Powerpoint Presentations Prepared by Bradley W. Christian, Mclennan Community CollegeDocument35 pagesAntimicrobial Drugs: Powerpoint Presentations Prepared by Bradley W. Christian, Mclennan Community CollegeTiffany Jane Huertas100% (1)
- 2021 Examining The Black U.S. Maternal Mortality Rate and How ToDocument2 pages2021 Examining The Black U.S. Maternal Mortality Rate and How ToCece JohnsonNo ratings yet
- Ab Omas A L Ulceration Andtympanyofcalves: Tessa S. MarshallDocument12 pagesAb Omas A L Ulceration Andtympanyofcalves: Tessa S. Marshallana lauraNo ratings yet
- Breast Cancer Complications and Prognosis LastDocument42 pagesBreast Cancer Complications and Prognosis Lastalalmaee1No ratings yet
- Spinal ShockDocument82 pagesSpinal ShockPhysiology by Dr Raghuveer100% (2)
- Big Can Be Beautiful, TIVA in The ObeseDocument7 pagesBig Can Be Beautiful, TIVA in The ObeseHernán GiménezNo ratings yet
- Medical Terminology CH 8Document139 pagesMedical Terminology CH 8ياسين المسطوNo ratings yet
- DEVPSY Reviewer - Chapters 1-6Document17 pagesDEVPSY Reviewer - Chapters 1-6Charmaine FloresNo ratings yet
- Development and Testing of ATime Resolved Personal Ozone MonitorDocument80 pagesDevelopment and Testing of ATime Resolved Personal Ozone MonitorJijo SagaiNo ratings yet
- A Study On Work From Home, Motivation & Productivity of Employees in Indian Population During COVID-19 PandemicDocument15 pagesA Study On Work From Home, Motivation & Productivity of Employees in Indian Population During COVID-19 Pandemicمعن الفاعوريNo ratings yet
- Laporan Bulanan Pasien CT - Scan 2016Document165 pagesLaporan Bulanan Pasien CT - Scan 2016Fera NurrizaNo ratings yet
- Oncology Nursing Must Knows by Dr. Chris G. SorongonDocument2 pagesOncology Nursing Must Knows by Dr. Chris G. SorongonAleandro DizonNo ratings yet



































































































Download as pdf or txt
You might also like
- Utrecht Gender Dysphoria Scale PDFDocument16 pagesUtrecht Gender Dysphoria Scale PDFTherese EspinosaNo ratings yet
- Obesity Research PaperDocument10 pagesObesity Research PaperPaige-Hill88% (16)
- Syndromic Gastric PolypsDocument15 pagesSyndromic Gastric PolypsTheDrakairNo ratings yet
- Concept Map On Renal FailureDocument1 pageConcept Map On Renal FailureJessilda Damian VeranoNo ratings yet
- The Social Dilemma ReviewDocument5 pagesThe Social Dilemma ReviewNikkaDablio100% (1)
- Health and Fitness in Senior Years: Group MembersDocument35 pagesHealth and Fitness in Senior Years: Group MembersSiti Halimatus Saadiah100% (1)
- 0304 ConsultantoncallDocument4 pages0304 Consultantoncallnessimmounir1173No ratings yet
- Lacpacan Breast Cancer Concept MapDocument1 pageLacpacan Breast Cancer Concept MapRIZI LACPACANNo ratings yet
- Group D Members:: Kidney Liver PancreasDocument1 pageGroup D Members:: Kidney Liver PancreasCourtney KateNo ratings yet
- Pediatric Therapeutics: Eximius 2021Document13 pagesPediatric Therapeutics: Eximius 2021Isabel CastilloNo ratings yet
- Genome Poster 2009Document1 pageGenome Poster 2009ISAAC LEWNo ratings yet
- Gems Opt Select Brochure 2021 v6 3Document2 pagesGems Opt Select Brochure 2021 v6 3Bongani West VuthaNo ratings yet
- Week 3 - Amoeba - SarcodinaDocument14 pagesWeek 3 - Amoeba - SarcodinaShine CalarananNo ratings yet
- 5sample - Gastrointestinal System Notes - 3rd Ed OptimizedDocument28 pages5sample - Gastrointestinal System Notes - 3rd Ed OptimizedAlexis Tobar100% (2)
- GDM PathophysiologyDocument2 pagesGDM PathophysiologyShahina ShayneNo ratings yet
- HZ SummaryDocument1 pageHZ SummaryPratzNo ratings yet
- All Charts Final Exam 1 PDFDocument294 pagesAll Charts Final Exam 1 PDFYasir RasoolNo ratings yet
- Azathioprine Drug StudyDocument1 pageAzathioprine Drug StudyAlexa Lexington Rae Zagado100% (1)
- Gynaecology Revision PDFDocument13 pagesGynaecology Revision PDFAadhi AadhiNo ratings yet
- DRUGDocument4 pagesDRUGPINKI DEBNo ratings yet
- Tables ProtozoaDocument14 pagesTables ProtozoaJanette Monica BarriosNo ratings yet
- Poster Caitlin BrennanDocument1 pagePoster Caitlin Brennansagun maharjanNo ratings yet
- Medical Prefixes and SuffixesDocument12 pagesMedical Prefixes and SuffixesKrishnanunni KLNo ratings yet
- Severe: Severe Persis4ng Symptoms of One or More Of: Gastrointes Nal SkinDocument2 pagesSevere: Severe Persis4ng Symptoms of One or More Of: Gastrointes Nal SkinSanjuy GarzaNo ratings yet
- Chapter 5Document23 pagesChapter 5ozmanNo ratings yet
- Week 2 (Lec-Lab) Mls 306 Clinical Parasitology Bsmls 3A: Ascaris LumbricoidesDocument4 pagesWeek 2 (Lec-Lab) Mls 306 Clinical Parasitology Bsmls 3A: Ascaris LumbricoidesHannah Beatrice Adame TamayoNo ratings yet
- Colorect: Patient's Name: F.V Age: 64 Years OldDocument3 pagesColorect: Patient's Name: F.V Age: 64 Years OldGenynne Ragasa100% (1)
- Biowords v2Document3 pagesBiowords v2Hiezeyl Ymana GuntangNo ratings yet
- Drug To Xi CitiesDocument1 pageDrug To Xi CitiesGIST (Gujarat Institute of Science & Technology)No ratings yet
- Trematodes ScheduleDocument1 pageTrematodes ScheduleDr-positive EnergyNo ratings yet
- Diarrhoea-Vomiting Pathway-Primary Care MAY 2015Document2 pagesDiarrhoea-Vomiting Pathway-Primary Care MAY 2015nimraNo ratings yet
- 2 1 Chemistry and Pharmacology of Anticancer Drugs - Docx-8-13Document6 pages2 1 Chemistry and Pharmacology of Anticancer Drugs - Docx-8-13A HNo ratings yet
- Viii. PathophysiologyDocument2 pagesViii. Pathophysiologymacedon145377No ratings yet
- Chapter54 Management of Patients With Kidney DisordersDocument40 pagesChapter54 Management of Patients With Kidney Disordersjericho dinglasanNo ratings yet
- Approach To Abdominal PainDocument4 pagesApproach To Abdominal PainShamen KohNo ratings yet
- HISTORY & EXAMINATION Edited 228Document11 pagesHISTORY & EXAMINATION Edited 228Saurabh LamkhadeNo ratings yet
- 01 Sick Bird SyndromeDocument1 page01 Sick Bird SyndromeAli BakNo ratings yet
- MUGOT - DEMENTIA CONCEPT MAP - Page 3Document1 pageMUGOT - DEMENTIA CONCEPT MAP - Page 3MICHELLIN VAN MUGOTNo ratings yet
- Gastrointestinal DisordersDocument4 pagesGastrointestinal DisordersJerica Mae VenoyaNo ratings yet
- T2 DM Seizure 1Document1 pageT2 DM Seizure 1Mika SaldanaNo ratings yet
- Hypoparathyroidism Care MapDocument1 pageHypoparathyroidism Care MapDeo FactuarNo ratings yet
- Ashap Medical Terminology Chapter 1Document1 pageAshap Medical Terminology Chapter 1Lorelyn FabrigarasNo ratings yet
- Legend: PathophysiologyDocument1 pageLegend: PathophysiologyMikhail LamayoNo ratings yet
- Algorithm 2: Diarrhea: Signalment/History/Exam Polyuria DiarrheaDocument1 pageAlgorithm 2: Diarrhea: Signalment/History/Exam Polyuria DiarrheaAli BakNo ratings yet
- NUR 3032 Pancreatic, Biliary, and Hepatic Disorders Study PlanDocument6 pagesNUR 3032 Pancreatic, Biliary, and Hepatic Disorders Study PlanThalia FortuneNo ratings yet
- Bacteria Chart FINAL 3 2Document32 pagesBacteria Chart FINAL 3 2Йеша Маниш МираниNo ratings yet
- Drug Study FormDocument4 pagesDrug Study FormRhea LaplanaNo ratings yet
- Pi Is 0923753419544970Document6 pagesPi Is 0923753419544970AyeshaNo ratings yet
- Pancreatitis Aguda Guías ClínicasDocument1 pagePancreatitis Aguda Guías Clínicaslbritez7No ratings yet
- DRUG - NDocument1 pageDRUG - NaizatiangcoNo ratings yet
- A3 Plant KingdomDocument1 pageA3 Plant KingdomMeenakshi VermaNo ratings yet
- Skema AnalisaDocument2 pagesSkema AnalisaAhmad MukhlisNo ratings yet
- Histopathological Features in Anemia DisordersDocument1 pageHistopathological Features in Anemia Disorderskoki74No ratings yet
- Drug Study Camillus MabiniDocument5 pagesDrug Study Camillus MabiniJonh Carlo LopezNo ratings yet
- Parasites High YoieldDocument4 pagesParasites High Yoieldnreena aslamNo ratings yet
- Animals Study Guide - Yeshen a. (2-4)Document5 pagesAnimals Study Guide - Yeshen a. (2-4)krisamikaela1123No ratings yet
- NoteDocument9 pagesNote65O6O78 ฐิติพันธ์ เพชรกระจายแสงNo ratings yet
- Endocrine SystemDocument1 pageEndocrine SystemMuhammad Jefri LukmanNo ratings yet
- PGI Reyes StomachDocument124 pagesPGI Reyes StomachMark ReyesNo ratings yet
- AmebasDocument3 pagesAmebasNaomi NicoleNo ratings yet
- Bacteriology 1: - Non MotileDocument27 pagesBacteriology 1: - Non MotileYeshaa MiraniNo ratings yet
- En DoDocument2 pagesEn Dofatima_antonioNo ratings yet
- Geriatric Nursing: Trends and IssuesDocument11 pagesGeriatric Nursing: Trends and IssuesNikkaDablioNo ratings yet
- OB WorkbookDocument13 pagesOB WorkbookNikkaDablioNo ratings yet
- Geriatric Nursing: Theories of AgingDocument4 pagesGeriatric Nursing: Theories of AgingNikkaDablioNo ratings yet
- TFN - BennerDocument1 pageTFN - BennerNikkaDablioNo ratings yet
- Geriatric Nursing: Physiologic ChangesDocument25 pagesGeriatric Nursing: Physiologic ChangesNikkaDablioNo ratings yet
- Nursing Care Plan For Patients With Pneumonia and Pulmonary EmbolismDocument5 pagesNursing Care Plan For Patients With Pneumonia and Pulmonary EmbolismNikkaDablioNo ratings yet
- 19th Century RizalDocument2 pages19th Century RizalNikkaDablioNo ratings yet
- PsoriasisDocument27 pagesPsoriasisNikkaDablioNo ratings yet
- Sihay - Ang Silid NG BuhayDocument5 pagesSihay - Ang Silid NG BuhayNikkaDablio100% (1)
- Nikka Dablio - ACTIVITY 1 The Paradox of Our TimeDocument1 pageNikka Dablio - ACTIVITY 1 The Paradox of Our TimeNikkaDablioNo ratings yet
- Central Mindanao University: Department of BiologyDocument4 pagesCentral Mindanao University: Department of BiologyNikkaDablioNo ratings yet
- Datasheet On Factors Affecting BuffersDocument14 pagesDatasheet On Factors Affecting BuffersNikkaDablioNo ratings yet
- Map of Region IIIDocument8 pagesMap of Region IIINikkaDablioNo ratings yet
- Saudi Arabia Written ReportDocument3 pagesSaudi Arabia Written ReportNikkaDablioNo ratings yet
- Patterns of StrugglesDocument2 pagesPatterns of StrugglesNikkaDablioNo ratings yet
- Vijaya DiagnosticsDocument3 pagesVijaya DiagnosticssampathNo ratings yet
- Women The Skilled Architect of The SocietyDocument4 pagesWomen The Skilled Architect of The SocietyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Orthodontic Space Closure Using Simple Mechanics in Compromised First Molar Extraction Spaces: Case SeriesDocument9 pagesOrthodontic Space Closure Using Simple Mechanics in Compromised First Molar Extraction Spaces: Case SeriesHabeeb AL-AbsiNo ratings yet
- 2048 Wal LA Clarification Deficiency CA FSHC PKTDocument7 pages2048 Wal LA Clarification Deficiency CA FSHC PKTJuliana GallardoNo ratings yet
- Resume of DR Pramod Nanda - Manager in Health Care Professional 2021Document10 pagesResume of DR Pramod Nanda - Manager in Health Care Professional 2021Dr Pramod NandaNo ratings yet
- The Paediatric Voice Clinic: Ian Smillie, Kirsy Mcmanus, Wendy Cohen, Elizabeth Lawson, David Macgregor WynneDocument5 pagesThe Paediatric Voice Clinic: Ian Smillie, Kirsy Mcmanus, Wendy Cohen, Elizabeth Lawson, David Macgregor WynneCarolina UrrutiaNo ratings yet
- Pilar College of Zamboanga City, IncDocument14 pagesPilar College of Zamboanga City, IncIvy VillalobosNo ratings yet
- Alternative FeedingDocument36 pagesAlternative FeedingEula Angelica OcoNo ratings yet
- History of MedicineDocument24 pagesHistory of MedicineРоман КравецьNo ratings yet
- Cleft Lip Palate TherapyDocument5 pagesCleft Lip Palate TherapyNathalieCaracaNo ratings yet
- English Project 2Document34 pagesEnglish Project 2HARSHNo ratings yet
- OralcholecystographyDocument13 pagesOralcholecystographySuman PokhrelNo ratings yet
- FS Nicotine Mouth SprayDocument11 pagesFS Nicotine Mouth SprayAdnan DugonjicNo ratings yet
- 06 AQU347 Course Notes Chapter 1Document13 pages06 AQU347 Course Notes Chapter 1Nurul Syafiqah Binti ShaidanNo ratings yet
- PDF Hypertension A Companion To Braunwalds Heart Disease 3Rd Edition George L Bakris Ebook Full ChapterDocument53 pagesPDF Hypertension A Companion To Braunwalds Heart Disease 3Rd Edition George L Bakris Ebook Full Chapteriris.russell843100% (3)
- Antimicrobial Drugs: Powerpoint Presentations Prepared by Bradley W. Christian, Mclennan Community CollegeDocument35 pagesAntimicrobial Drugs: Powerpoint Presentations Prepared by Bradley W. Christian, Mclennan Community CollegeTiffany Jane Huertas100% (1)
- 2021 Examining The Black U.S. Maternal Mortality Rate and How ToDocument2 pages2021 Examining The Black U.S. Maternal Mortality Rate and How ToCece JohnsonNo ratings yet
- Ab Omas A L Ulceration Andtympanyofcalves: Tessa S. MarshallDocument12 pagesAb Omas A L Ulceration Andtympanyofcalves: Tessa S. Marshallana lauraNo ratings yet
- Breast Cancer Complications and Prognosis LastDocument42 pagesBreast Cancer Complications and Prognosis Lastalalmaee1No ratings yet
- Spinal ShockDocument82 pagesSpinal ShockPhysiology by Dr Raghuveer100% (2)
- Big Can Be Beautiful, TIVA in The ObeseDocument7 pagesBig Can Be Beautiful, TIVA in The ObeseHernán GiménezNo ratings yet
- Medical Terminology CH 8Document139 pagesMedical Terminology CH 8ياسين المسطوNo ratings yet
- DEVPSY Reviewer - Chapters 1-6Document17 pagesDEVPSY Reviewer - Chapters 1-6Charmaine FloresNo ratings yet
- Development and Testing of ATime Resolved Personal Ozone MonitorDocument80 pagesDevelopment and Testing of ATime Resolved Personal Ozone MonitorJijo SagaiNo ratings yet
- A Study On Work From Home, Motivation & Productivity of Employees in Indian Population During COVID-19 PandemicDocument15 pagesA Study On Work From Home, Motivation & Productivity of Employees in Indian Population During COVID-19 Pandemicمعن الفاعوريNo ratings yet
- Laporan Bulanan Pasien CT - Scan 2016Document165 pagesLaporan Bulanan Pasien CT - Scan 2016Fera NurrizaNo ratings yet
- Oncology Nursing Must Knows by Dr. Chris G. SorongonDocument2 pagesOncology Nursing Must Knows by Dr. Chris G. SorongonAleandro DizonNo ratings yet