Professional Documents
Culture Documents
Fisiopatologia Del TEC Severo
Fisiopatologia Del TEC Severo
Uploaded by
FabianPintoOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Fisiopatologia Del TEC Severo
Fisiopatologia Del TEC Severo
Uploaded by
FabianPintoCopyright:
Available Formats
©
or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other means which may allow access
COPYRIGHT 2018 EDIZIONI MINERVA MEDICA
cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo, or other proprietary information of the Publisher.
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies (either sporadically
to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is not permitted. It is not permitted to remove,
© 2018 EDIZIONI MINERVA MEDICA Journal of Neurosurgical Sciences 2018 October;62(5):542-8
Online version at http://www.minervamedica.it DOI: 10.23736/S0390-5616.18.04501-0
REVIEW
S E V E R E T R A U M AT I C B R A I N I N J U R Y
Pathophysiology of severe traumatic brain injury
Ruth A. O’LEARY 1, Alistair D. NICHOL 1, 2, 3 *
1Department of Intensive Care Medicine, Alfred Hospital, Melbourne, Australia; 2Australia and New Zealand Intensive Care-Research
Center, School of Public Health and Preventive Medicine, Monash University, Melbourne, Australia; 3University College Dublin Clinical
Research Centre, St Vincent’s University Hospital, Dublin, Ireland
*Corresponding author: Alistair D. Nichol, Department of Intensive Care Medicine, Alfred Hospital, Melbourne, Australia.
E-mail: alistair.nichol@monash.edu
A B S T RAC T
Traumatic brain injury is a leading cause of morbidity and mortality globally, particularly among young people, with significant social and
economic effects. The World Health Organization (WHO) estimates that more than five million people die each year from traumatic injuries
worldwide. While public health initiatives such as seatbelts and airbags have had a major impact, it will be impossible to prevent traumatic brain
injury.Therefore, it is important that we understand the pathophysiology of secondary brain injury to be able to effectively treat our patient and
also to develop novel targets of future interventions. The mechanisms of secondary brain injury are complex involving alterations in cerebral
perfusion, activation of inflammatory cytokines and excitotoxicity. While our understanding of these mechanisms has advanced greatly over
the last decade, there is still much to learn and great uncertainty at the bedside. There has been some recent success with the discovery of some
simple interventions that can reduce secondary brain injury and improve outcomes in patients after traumatic brain injury. In this review we
summarize the current understanding of mechanisms and pathophysiology of primary and secondary brain injury, the goals for current treatment
and potential targets for future therapy.
(Cite this article as: O’Leary RA, Nichol AD. Pathophysiology of severe traumatic brain injury. J Neurosurg Sci 2018;62:542-8. DOI: 10.23736/
S0390-5616.18.04501-0)
Key words: Traumatic brain injuries - Pathophysiology - Cerebrovascular circulation - Neurogenic inflammation.
T he World Health Organization (WHO) estimates that
more than five million people die each year from
traumatic injuries worldwide.1 These represent 9% of all
Classification of traumatic brain injury
TBI may be classified in a number of different ways. It was
deaths and are 1.7 times the number of fatalities that re- initially understood in terms of its effect on level of con-
sult from HIV/AIDS, tuberculosis and malaria combined.1 sciousness and clinical scores were used to classify TBI on
Over 1.3 million of these deaths are a result of road trauma: this basis. The Glasgow Coma Scale (GCS) has been used
by 2020 this is projected to increase to over 2 million.2 to classify TBIs according to severity — mild (GCS 14-15),
Traumatic brain injury (TBI) is the leading cause of mor- moderate (GCS 9-13), or severe (GCS 3-8).4 This scale is
tality in young people and as a result it has significant so- made up of verbal, eye and motor responses to increasing
cial and economic impact: globally the estimated annual stimulus and has been in use for more than forty years and
cost of road trauma alone is estimated to be in excess of $ still appears to have adequate reliability to determine long
500 billion.3 We summarize the current understanding of term outcome.5 For accurate assessment the components of
mechanisms and pathophysiology of primary and second- the scale should be reported separately rather than as a sum
ary brain injury, the goals for current treatment and poten- score. This is because the sum score is less reliable than the
tial targets for future therapy. component scores5 and also because the motor component
542 Journal of Neurosurgical Sciences October 2018
©
or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other means which may allow access
COPYRIGHT 2018 EDIZIONI MINERVA MEDICA
cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo, or other proprietary information of the Publisher.
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies (either sporadically
to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is not permitted. It is not permitted to remove,
PATHOPHYSIOLOGY OF SEVERE TBI O’LEARY
in its own right is a predictor of outcome in severe TBI.6 injury, although commonly focal and diffuse injuries co-
However, in the hospital setting clinical classification of exist.15 Injuries resulting from a direct impact (e.g. closed
TBI may be of limited use due to confounding factors such injury from focal blow or crush injury, penetrating wound)
as sedation.7, 8 In view of this other means of classification are characteristically focal, presenting as contusions or
have become widely adopted in both research and clinical hematomas. Focal contusions are the most common pre-
practice over the last number of years. senting lesion but intracranial hematomas may occur in up
Radiological classification is commonly used to aid in to 35% of patients with severe TBI.4, 15 These are readily
the prediction of prognosis. The presence of a number of visible on radiological imaging studies and may be graded
individual features such as midline shift and subarachnoid using the classification systems discussed above.10, 12 Ac-
hemorrhage are predictive of outcome in severe TBI9 and celeration and deceleration injuries are associated with
in addition to this a number of classification systems are in more diffuse injuries related to rotational, shearing forc-
use. The Marshall classification system10 has been widely es.15 These may not manifest in radiological abnormalities
used for over 15 years. It divides TBI into six categories initially although there may be vascular damage at higher
— diffuse 1-4 with progressive amounts of compression, shear rates, leading to microhemorrhages.4 Diffuse axonal
midline shift and mixed-density lesions and mass lesions injuries may result from these acceleration/deceleration
either evacuated or non-evacuated. It is useful in that it injuries and are characterized by coma and poor outcome
describes the injuries on the brain but it has a number of despite benign radiological appearances.
limitations. Firstly, it cannot be used as a grading system
as mortality does not increase with each grade. Specifi-
Secondary brain injury
cally the mortality for class 5 (an evacuated mass lesion)
is predictably lower than for class 6 (an unevacuated mass Secondary brain injury results from a complex cascade of
lesion).11 In addition to this, it fails to differentiate between events. Alterations in cerebral blood flow and metabolic
different types of hematoma and discounts traumatic sub- dysfunction are associated with poor outcomes. In addi-
arachnoid hemorrhage entirely. Due to these shortcomings tion to this, TBI leads to immune activation with the re-
the Rotterdam scoring system was developed — a linear lease of excitatory neurotransmitters and inflammatory cy-
grading system that correlates with increasing mortality.12 tokines. Our understanding of this complex interplay has
Both scores correlate with mortality and with each other improved significantly since the start of the millennium
and are used widely. Finally, a number of different prog- and the mechanisms detailed below have provided new
nostic models have been developed based on admission therapeutic targets.
criteria. These have been developed from large patient
groups, such as those participating in the CRASH and IM-
PACT trial groups6, 13 and take into account demographic Cerebral perfusion
data, clinical and radiological findings and the presence
Alterations in cerebral blood flow (CBF) are commonly
of extracranial injuries. These models have found asso-
seen in the setting of traumatic brain injury. Inadequate
ciations between age, motor score and pupillary responses
CBF leads to ischemia and consequently worse outcomes
and outcome at 6 months. The addition of CT findings,
with increased morbidity and mortality. These changes re-
specifically the presence of subarachnoid blood, hemato-
sult from complex interactions between systemic hypoten-
ma and mass lesion and compression of the basal cisterns,
sion, impaired autoregulation, raised intracranial pressure
improves the predictive power of the model.6 Although the
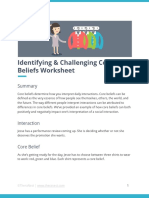
(ICP) and vasospasm (Figure 1).16
models developed from these large patient cohorts allow
It is well-recognized that TBI frequently results in hy-
classification by predicted outcome and may be of use on
poperfusion leading to cerebral ischemia. This may be fo-
an organizational level, they should be used to augment
cal or global and has been established by multiple different
rather than replace clinical judgement.14
imaging modalities.17, 18 Cerebral ischemia in this setting
occurs due to a number of different mechanisms including
Primary brain injury direct injury to vessels, mechanical compression, hypoten-
sion and reduced perfusion due to failure of autoregula-
Primary brain injury occurs when an external force results tion.19 Of note ischemia occurs at a higher rate of CBF
in brain damage, which may be focal or diffuse. The pat- than is found in ischemic stroke,20 even though cerebral
tern of damage seen differs according to the mechanism of metabolic rate for oxygen is reduced after severe TBI.21-23
Vol. 62 - No. 5 Journal of Neurosurgical Sciences 543
©
or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other means which may allow access
COPYRIGHT 2018 EDIZIONI MINERVA MEDICA
cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo, or other proprietary information of the Publisher.
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies (either sporadically
to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is not permitted. It is not permitted to remove,
O’LEARY PATHOPHYSIOLOGY OF SEVERE TBI
be difficult to assess due to the use of sedation. The mech-
anisms leading to vasospasm in this population include
chronic depolarization of vascular smooth muscle due to
reduced potassium channel activity16, 31 and reduced avail-
ability of smooth muscle relaxants such as nitric oxide and
cyclic GMP.32
Cerebral metabolism and oxygenation
Intracranial pressure
In the immediate aftermath of a severe TBI there is an
increase in energy needs but a decrease in CRMO. This
leads to metabolic uncoupling and energy dysfunction.33
This dysfunction is associated with poor neurological
Mass lesion size prognosis.21, 34 Lactate levels are commonly increased in
this setting and this has, in the past, been interpreted as
Figure 1.—The Monro Kellie hypothesis: this schema describes the re-
lationship between the non-compressible components of the intracranial a marker of anaerobic metabolism and a potential target
volume. The skull is a rigid compartment so an increase in the volume for hyperoxic therapy.35 However, in this setting lactate
of brain tissue, CSF or blood must result either in a decrease in the other production may be due to hyperglycolysis in the absence
two components or an increase in intracranial pressure.
of ischemia33 and it may become an alternative substrate
to glucose for metabolism.36 Similarly, mitochondrial dys-
In addition to hypoperfusion, patients with TBI may also function is also seen in non-ischemic areas. These areas
develop cerebral hyperperfusion, which is similarly detri- with injury-induced mitochondrial dysfunction are associ-
mental. This leads to increased cerebral blood volume and ated with worse outcomes.37 Hyperoxia has been investi-
consequently increased ICP.24 gated as a therapy for these metabolic derangements with
CBF is normally tightly autoregulated — blood vessels disappointing results.35
constrict or dilate to maintain a constant blood flow be-
tween mean arterial pressure ranges of 50-150 mmHg.25, 26 Oxidative stress and excitotoxicity
This autoregulation is impaired after TBI so CBF directly
correlates with MAP. As a result, patients are much more Oxidative stress plays a significant role in the development
susceptible to hypoperfusion after traumatic insults. Im- of secondary injury after severe TBI. Reactive oxygen and
pairment in autoregulation may occur immediately after nitrogen species are formed when there is an imbalance be-
the event or it may develop over time and it may persist for tween their production and the activity of antioxidants such
a variable amount of time. Autoregulation is more likely to as glutathione peroxidase and superoxide dismutase.38 Su-
be impaired in response to decreased MAP, suggesting that peroxide is the most common free radical seen after TBI39
patients post TBI are less likely to tolerate hypotension.16 and its production is associated with high intracellular cal-
Cerebrovascular response to changes in CO2 is relatively cium levels.40 The proliferation in free radicals causes tis-
preserved even in severe TBI, suggesting it as a target for sue damage by promoting hydroxyl radicals and through
ICP management. However, multiple studies have shown activation of matrix metalloproteinases (MMPs). MMPs
that arterial vasoconstriction in response to hypocapnia leads are responsible for extracellular matrix degradation of the
to worse outcomes due to cerebral hypoperfusion, rebound blood brain barrier (BBB) and their inappropriate activa-
intracranial hypertension on restoration of normocapnia and tion results in increased BBB permeability (Figure 2).41, 42
N-methyl-D-aspartate-receptor-mediated neurotoxicity.27 In Oxygen free radicals may also lead to the activation of
view of this hypocapnia is recommended only as emergent nuclear factor-kappa B (NF-κB).43 NF-κB increases the
management of life-threatening ICP rises. transcription of pro-inflammatory cytokines such as tu-
Vasospasm is well-described after subarachnoid hemor- mor necrosis factor-α (TNF-α) and interleukin-6 (IL-6).44
rhage and is associated with poor outcomes.28 A similar Although these mediators may be associated with normal
picture is seen in TBI patients with vasospasm occurring wound healing, inappropriate activation may be associat-
in up to 40% of patients.29, 30 However, vasospasm occurs ed with secondary brain injury. These pathophysiological
earlier in TBI patient, within 12 hours of injury and may changes are seen in other forms of brain injury, such as
544 Journal of Neurosurgical Sciences October 2018
©
or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other means which may allow access
COPYRIGHT 2018 EDIZIONI MINERVA MEDICA
cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo, or other proprietary information of the Publisher.
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies (either sporadically
to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is not permitted. It is not permitted to remove,
PATHOPHYSIOLOGY OF SEVERE TBI O’LEARY
ronal nitric oxide.40 This reacts with superoxide, discussed
above, to produce peroxynitrite, a highly reactive nitrating
free radical, which causes rapid cell death by a number of
processes.50, 51 The role of NMDA receptors in the devel-
opment of excitotoxicity has been confirmed by the obser-
vation that NMDA receptor agonists are more potent neu-
rotoxins than glutamate when delivered directly into the
brain.52 AMPA receptors are also found to be overactive
in the presence of neuronal injury, as seen after TBI. This
overactivity results in increased intracellular calcium, hy-
perexcitability and consequently cell damage and death.40
In view of these findings there is ongoing interest in target-
ing NMDA and AMPA receptors with the aim of mitigat-
ing glutamate associated neuroexcitotoxicity.
Figure 2.—Schematic representation of oxidative stress-induced BBB
disruption and neuroinflammation in traumatic brain injury. Reactive
oxygen species (ROS) and reactive nitrogen species (RNS) are the Calcium homeostasis
main sources of oxidative stress in brain injury. ROS include superox-
ide (O2−), hydroxyl radical (HO), hydrogen peroxide (H2O2), and hypo- Abnormalities in calcium homeostasis play a critical role
chlorous acid (HOCl). RNS refer to various nitric oxide (NO)-derived in the development of secondary injury after TBI. As dis-
compounds, such as peroxynitrite (ONOO–) and nitrogen dioxide (NO2).
O2− causes tissue damage by promoting hydroxyl radicals from H2O2 cussed above, increased intracellular free calcium levels
and ONOO– when combined with NO. ROS activate matrix metallo- lead to neuroexcitotoxicity resulting in cell death through
proteinases (MMPs) that further exacerbate the condition and lead to
BBB disruption via degradation of the extracellular matrix and tight activation of a number of enzymes. Mitochondrial swell-
junction proteins. Further, MMPs are involved in degradation of vas- ing occurs due to an increase in calcium sequestration and
cular endothelial growth factor (VEGFR) and lead to an increase in the this also leads to membrane depolarization with resultant
level of VEGF that in turn causes ROS and activates caspase-1/3, which
leads to cell death. At the same time, ROS or RNS also activate differ- release of factors that initiate programmed cell death.53, 54
ent inflammatory cytokines and growth factors such as IL-1β, TNF-α, The resultant mitochondrial dysfunction leads to further
and TGF-β, which cause BBB disruption and neuroinflammation (from
Abdul-Muneer et al.).39 calcium influx. Increased axonal membrane permeability
also allows an influx of calcium.55 This leads to activation
of a family of enzymes, calpains, which target and degrade
neurodegenerative disease and alcohol abuse.45, 46 There key structural proteins.56 Ultimately these cascades lead to
has been significant interest in the use of antioxidants to axonal damage and disconnection.40
reduce the impact of these free radicals, however to date
none have proven effective in phase III clinical trials.16, 47
Increased extracellular concentrations of the excitatory Neuroinflammation
neurotransmitter glutamate have been found after severe Traumatic brain injury results in an inflammatory response,
TBI.40 This increase is multifactorial in nature. Disruption described as a sterile immune reaction.57 This reaction is
of the BBB allows glutamate to move into the brain and initiated by purinergic receptor signaling triggered by
in addition to this extravasation of glutamate may occur ATP released by damaged cells58 and involves microglia,
at the site of traumatic vascular damage.48, 49 Excessive monocytes and neutrophils.
synaptic release of glutamate and impairment of glutamate Microglia are immune sentinels that reside in the CNS
transporters compounds this increase in interstitial gluta- and are first responders to inflammation.59 They may
mate.49 The result is overstimulation of glutamate recep- transform into phagocytic cells in response to an injury
tors leading to excitotoxicity. Glutamate mediates these and their response appears to be neuroprotective.57, 59, 60
adverse effects through the stimulation of NMDA and Microglia can respond to purinergic signals after cell death
alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic and become phagocytes known as jellyfish microglia.57
(AMPA) receptors. These microglia can take the place of the dead cells and
NMDA receptors are coupled with the generation of re- thus seal gaps. As such they provide a dual role, remov-
active oxygen and nitrogen species so their overstimula- ing the debris of dead cells and sealing gaps in the glial
tion leads to the release of free radicals, in particular neu- limitans barrier. Monocytes are capable of differentiating
Vol. 62 - No. 5 Journal of Neurosurgical Sciences 545
©
or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other means which may allow access
COPYRIGHT 2018 EDIZIONI MINERVA MEDICA
cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo, or other proprietary information of the Publisher.
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies (either sporadically
to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is not permitted. It is not permitted to remove,
O’LEARY PATHOPHYSIOLOGY OF SEVERE TBI
into macrophages and dendritic cells in response to inflam- Conclusions
mation or injury and their role appears to be destructive
after TBI. Meningeal macrophage death provides an early Management of traumatic brain injury remains a sig-
source of reactive oxygen species after cortical injury.61 nificant challenge for clinicians. Public health initiatives
Subsequently monocytes cross the blood brain barrier aimed at reducing rates of primary brain injury are of para-
through the production of CCL2 by the choroid plexus.62 mount importance,1 however therapies targeting second-
This response appears to be maladaptive with animal data ary brain injury are also required. A clear understanding
to suggest that outcomes are improved when this pathway of the complex pathophysiology of primary and secondary
is blocked.63 brain injury is necessary to guide the development of new
Neutrophils are rapidly recruited to the site of injury af- therapies. Few therapies to date have demonstrated benefit
ter TBI and their involvement may be neuroprotective or in clinical trials so ongoing research is needed to improve
destructive. There is data to suggest that neutrophils are outcomes in the future.
neuroprotective in the meningeal space, interacting with
dead cells in the acute response to injury. However, they
may also release harmful mediators including reactive ox- References
ygen species and metalloproteinases, which may result in 1. World Health Organization. Injuries and violence: the facts; 2014 [In-
neurotoxicity and damage to the BBB.64 ternet]. Available from: www.who.int/violence_injury_prevention/media/
news/2015/Injury_violence_facts_2014/en/ [cited 2018;May 18].
2. Mathers CD, Loncar D. Projections of global mortality and burden of
Targets for future therapy disease from 2002 to 2030. PLoS Med 2006;3:e442.
3. World Health Organization. The global burden of disease; 2012 [Inter-
net]. Available from: www.who.int/topics/global_burden_of_disease/en/
At present therapy for TBI is limited to surgical manage- [cited 2018, May 18].
ment of lesions and supportive care aimed at maintaining 4. Maas AI, Stocchetti N, Bullock R. Moderate and severe traumatic
adequate cerebral perfusion and oxygenation. However, brain injury in adults. Lancet Neurol 2008;7:728–41.
given our improved understanding of the pathophysiology 5. Reith FC, Van den Brande R, Synnot A, Gruen R, Maas AI. The reli-
ability of the Glasgow Coma Scale: a systematic review. Intensive Care
underpinning secondary brain injury, a number of phar- Med 2016;42:3–15.
macological targets have been identified. Unfortunately, to 6. Murray GD, Butcher I, McHugh GS, Lu J, Mushkudiani NA, Maas AI,
date most studies have failed to demonstrate clinical ben- et al. Multivariable prognostic analysis in traumatic brain injury: results
from the IMPACT study. J Neurotrauma 2007;24:329–37.
efit in stage III trials.44 This may be due to the difficulties 7. Balestreri M, Czosnyka M, Chatfield DA, Steiner LA, Schmidt EA,
in targeting one component of a complex cascade, as well Smielewski P, et al. Predictive value of Glasgow Coma Scale after brain
as the heterogeneity of this population. trauma: change in trend over the past ten years. J Neurol Neurosurg Psy-
chiatry 2004;75:161–2.
Progesterone was up until recently regarded as a bio-
8. Stocchetti N, Pagan F, Calappi E, Canavesi K, Beretta L, Citerio G, et
logically plausible therapy for TBI. It is known to inhibit al. Inaccurate early assessment of neurological severity in head injury. J
inflammatory cytokines and prevent excitotoxicity and va- Neurotrauma 2004;21:1131–40.
sogenic edema and two phase 2 trials showed a clinical 9. Chestnut RM, Ghajar J, Maas AI, Marion DW, Servadei F, Teasdale
GM, et al. Early Indicators of Prognosis in Severe Traumatic Brain Injury.
benefit in this population.65, 66 However, two recent phase J Neurotrauma 2000;17:557–627.
three trials67, 68 failed to show any benefit over placebo and 10. Marshall LF, Marshall SB, Klauber MR, Clark MB, Eisenberg HM,
consequently a systematic review concluded that there was Jane JA, et al. A new classification of head injury based on computerized
tomography. J Neurosurg. Journal of Neurosurgery 1991;75(1s):S14–20.
no evidence of benefit.69 In contrast to the limited evidence
11. Deepika A, Prabhuraj AR, Saikia A, Shukla D. Comparison of pre-
found for progesterone therapy, it has been demonstrated dictability of Marshall and Rotterdam CT scan scoring system in deter-
that simple ICU interventions, such as the choice of resus- mining early mortality after traumatic brain injury. Acta Neurochir (Wien)
2015;157:2033–8.
citative fluid, or the decision to conduct surgery or not, can
12. Maas AI, Hukkelhoven CW, Marshall LF, Steyerberg EW. Prediction
reduce both mortality and severe disability in critically ill of outcome in traumatic brain injury with computed tomographic charac-
trauma patients70, 71 with substantial healthcare cost sav- teristics: a comparison between the computed tomographic classification
and combinations of computed tomographic predictors. Neurosurgery
ings of greater than $ 271 million independently reported.72 2005;57:1173–82.
Prophylactic hypothermia is another therapy with prom- 13. Perel P, Arango M, Clayton T, Edwards P, Komolafe E, Poccock S, et
ise. The POLAR study is examining the role of prophy- al.; MRC CRASH Trial Collaborators. Predicting outcome after traumatic
lactic hypothermia to 33 °C initiated within three hours brain injury: practical prognostic models based on large cohort of interna-
tional patients. BMJ 2008;336:425–9.
of injury and maintained for 72 hours. Results from the 14. Steyerberg EW, Mushkudiani N, Perel P, Butcher I, Lu J, McHugh
POLAR study will be published in late 2018.73 GS, et al. Predicting outcome after traumatic brain injury: development
546 Journal of Neurosurgical Sciences October 2018
©
or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other means which may allow access
COPYRIGHT 2018 EDIZIONI MINERVA MEDICA
cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo, or other proprietary information of the Publisher.
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies (either sporadically
to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is not permitted. It is not permitted to remove,
PATHOPHYSIOLOGY OF SEVERE TBI O’LEARY
and international validation of prognostic scores based on admission char- 35. Magnoni S, Ghisoni L, Locatelli M, Caimi M, Colombo A, Valeriani
acteristics. PLoS Med 2008;5:e165. V, et al. Lack of improvement in cerebral metabolism after hyperoxia in
15. Gaetz M. The neurophysiology of brain injury. Clin Neurophysiol severe head injury: a microdialysis study. J Neurosurg 2003;98:952–8.
2004;115:4–18. 36. Carpenter KL, Jalloh I, Hutchinson PJ. Glycolysis and the signifi-
16. DeWitt DS, Prough DS. Traumatic cerebral vascular injury: the ef- cance of lactate in traumatic brain injury. Front Neurosci 2015;9:112.
fects of concussive brain injury on the cerebral vasculature. J Neurotrau- 37. Gajavelli S, Kentaro S, Diaz J, Yokobori S, Spurlock M, Diaz D, et
ma 2003;20:795–825. al. Glucose and oxygen metabolism after penetrating ballistic-like brain
17. Coles JP, Fryer TD, Smielewski P, Rice K, Clark JC, Pickard JD, et injury. J Cereb Blood Flow Metab 2015;35:773–80.
al. Defining ischemic burden after traumatic brain injury using 15O PET 38. Cornelius C, Crupi R, Calabrese V, Graziano A, Milone P, Pennisi G,
imaging of cerebral physiology. J Cereb Blood Flow Metab 2004;24:191– et al. Traumatic brain injury: oxidative stress and neuroprotection. Anti-
201. oxid Redox Signal 2013;19:836–53.
18. Bouma GJ, Muizelaar JP, Stringer WA, Choi SC, Fatouros P, Young 39. Abdul-Muneer PM, Chandra N, Haorah J. Interactions of oxidative
HF. Ultra-early evaluation of regional cerebral blood flow in severely stress and neurovascular inflammation in the pathogenesis of traumatic
head-injured patients using xenon-enhanced computerized tomography. J brain injury. Mol Neurobiol 2015;51:966–79.
Neurosurg 1992;77:360–8. 40. Park E, Bell JD, Baker AJ. Traumatic brain injury: can the conse-
19. Rodríguez-Baeza A, Reina-de la Torre F, Poca A, Martí M, Garnacho quences be stopped? CMAJ 2008;178:1163–70.
A. Morphological features in human cortical brain microvessels after head 41. Kim GW, Gasche Y, Grzeschik S, Copin JC, Maier CM, Chan PH.
injury: a three-dimensional and immunocytochemical study. Anat Rec A Neurodegeneration in striatum induced by the mitochondrial toxin 3-ni-
Discov Mol Cell Evol Biol 2003;273:583–93. tropropionic acid: role of matrix metalloproteinase-9 in early blood-brain
20. Cunningham AS, Salvador R, Coles JP, Chatfield DA, Bradley barrier disruption? J Neurosci 2003;23:8733–42.
PG, Johnston AJ, et al. Physiological thresholds for irreversible tissue 42. Gasche Y, Fujimura M, Morita-Fujimura Y, Copin JC, Kawase M,
damage in contusional regions following traumatic brain injury. Brain Massengale J, et al. Early appearance of activated matrix metalloprotein-
2005;128:1931–42. ase-9 after focal cerebral ischemia in mice: a possible role in blood-brain
21. Vespa P, Bergsneider M, Hattori N, Wu HM, Huang SC, Martin NA, barrier dysfunction. J Cereb Blood Flow Metab 1999;19:1020–8.
et al. Metabolic crisis without brain ischemia is common after traumatic 43. Yang L, Tao LY, Chen XP. Roles of NF-kappaB in central nervous
brain injury: a combined microdialysis and positron emission tomography system damage and repair. Neurosci Bull 2007;23:307–13.
study. J Cereb Blood Flow Metab 2005;25:763–74.
44. McConeghy KW, Hatton J, Hughes L, Cook AM. A review of neu-
22. Bergsneider M, Hovda DA, Lee SM, Kelly DF, McArthur DL, Vespa roprotection pharmacology and therapies in patients with acute traumatic
PM, et al. Dissociation of cerebral glucose metabolism and level of con- brain injury. CNS Drugs 2012;26:613–36.
sciousness during the period of metabolic depression following human
traumatic brain injury. J Neurotrauma 2000;17:389–401. 45. Abdul Muneer PM, Alikunju S, Szlachetka AM, Haorah J. The
mechanisms of cerebral vascular dysfunction and neuroinflammation by
23. Diringer MN, Videen TO, Yundt K, Zazulia AR, Aiyagari V, Dacey MMP-mediated degradation of VEGFR-2 in alcohol ingestion. Arterio-
RG Jr, et al. Regional cerebrovascular and metabolic effects of hyperven- scler Thromb Vasc Biol 2012;32:1167–77.
tilation after severe traumatic brain injury. J Neurosurg 2002;96:103–8.
46. Rosenberg GA. Matrix metalloproteinases and their multiple roles in
24. Kelly DF, Martin NA, Kordestani R, Counelis G, Hovda DA, Bergs- neurodegenerative diseases. Lancet Neurol 2009;8:205–16.
neider M, et al. Cerebral blood flow as a predictor of outcome following
traumatic brain injury. J Neurosurg 1997;86:633–41. 47. Fernández-Gajardo R, Matamala JM, Carrasco R, Gutiérrez R, Melo
R, Rodrigo R. Novel therapeutic strategies for traumatic brain injury:
25. Rangel-Castilla L, Gasco J, Nauta HJ, Okonkwo DO, Robertson CS. acute antioxidant reinforcement. CNS Drugs 2014;28:229–48.
Cerebral pressure autoregulation in traumatic brain injury. Neurosurg Fo-
cus 2008;25:E7. 48. Koizumi H, Fujisawa H, Ito H, Maekawa T, Di X, Bullock R. Effects
of mild hypothermia on cerebral blood flow-independent changes in corti-
26. Enevoldsen EM, Jensen FT. Autoregulation and CO2 responses of cal extracellular levels of amino acids following contusion trauma in the
cerebral blood flow in patients with acute severe head injury. J Neurosurg rat. Brain Res 1997;747:304–12.
1978;48:689–703.
49. Yi JH, Hazell AS. Excitotoxic mechanisms and the role of astro-
27. Curley G, Kavanagh BP, Laffey JG. Hypocapnia and the injured cytic glutamate transporters in traumatic brain injury. Neurochem Int
brain: more harm than benefit. Crit Care Med 2010;38:1348–59. 2006;48:394–403.
28. Kassell NF, Sasaki T, Colohan AR, Nazar G. Cerebral vasospasm fol- 50. Trackey JL, Uliasz TF, Hewett SJ. SIN-1-induced cytotoxicity in
lowing aneurysmal subarachnoid hemorrhage. Stroke 1985;16:562–72. mixed cortical cell culture: peroxynitrite-dependent and -independent in-
29. Martin NA, Doberstein C, Zane C, Caron MJ, Thomas K, Becker DP. duction of excitotoxic cell death. J Neurochem 2001;79:445–55.
Posttraumatic cerebral arterial spasm: transcranial Doppler ultrasound, ce- 51. Arundine M, Aarts M, Lau A, Tymianski M. Vulnerability of central
rebral blood flow, and angiographic findings. J Neurosurg 1992;77:575–83. neurons to secondary insults after in vitro mechanical stretch. J Neurosci
30. Compton JS, Teddy PJ. Cerebral arterial vasospasm following severe 2004;24:8106–23.
head injury: a transcranial Doppler study. Br J Neurosurg 1987;1:435–9. 52. Obrenovitch TP, Urenjak J, Zilkha E. Intracerebral microdialysis
31. Sobey CG. Cerebrovascular dysfunction after subarachnoid haemor- combined with recording of extracellular field potential: a novel meth-
rhage: novel mechanisms and directions for therapy. Clin Exp Pharmacol od for investigation of depolarizing drugs in vivo. Br J Pharmacol
Physiol 2001;28:926–9. 1994;113:1295–302.
32. Todo H, Ohta S, Wang J, Ichikawa H, Ohue S, Kumon Y, et al. Im- 53. Saelens X, Festjens N, Vande Walle L, van Gurp M, van Loo G, Van-
pairment in biochemical level of arterial dilative capability of a cyclic denabeele P. Toxic proteins released from mitochondria in cell death. On-
nucleotides-dependent pathway by induced vasospasm in the canine basi- cogene 2004;23:2861–74.
lar artery. J Cereb Blood Flow Metab 1998;18:808–17. 54. Kim JS, He L, Lemasters JJ. Mitochondrial permeability transition: a
33. Patet C, Suys T, Carteron L, Oddo M. Cerebral Lactate Metabolism common pathway to necrosis and apoptosis. Biochem Biophys Res Com-
After Traumatic Brain Injury. Curr Neurol Neurosci Rep 2016;16:31. mun 2003;304:463–70.
34. Carre E, Ogier M, Boret H, Montcriol A, Bourdon L, Jean-Jacques R. 55. Wolf JA, Stys PK, Lusardi T, Meaney D, Smith DH. Traumatic axonal
Metabolic crisis in severely head-injured patients: is ischemia just the tip injury induces calcium influx modulated by tetrodotoxin-sensitive sodium
of the iceberg? Front Neurol 2013;4:146. channels. J Neurosci 2001;21:1923–30.
Vol. 62 - No. 5 Journal of Neurosurgical Sciences 547
©
or systematically, either printed or electronic) of the Article for any purpose. It is not permitted to distribute the electronic copy of the article through online internet and/or intranet file sharing systems, electronic mailing or any other means which may allow access
COPYRIGHT 2018 EDIZIONI MINERVA MEDICA
cover, overlay, obscure, block, or change any copyright notices or terms of use which the Publisher may post on the Article. It is not permitted to frame or use framing techniques to enclose any trademark, logo, or other proprietary information of the Publisher.
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this Article. It is not permitted to make additional copies (either sporadically
to the Article. The use of all or any part of the Article for any Commercial Use is not permitted. The creation of derivative works from the Article is not permitted. The production of reprints for personal or commercial use is not permitted. It is not permitted to remove,
O’LEARY PATHOPHYSIOLOGY OF SEVERE TBI
56. Maxwell WL, Povlishock JT, Graham DL. A mechanistic analysis of 66. Xiao G, Wei J, Yan W, Wang W, Lu Z. Improved outcomes from the
nondisruptive axonal injury: a review. J Neurotrauma 1997;14:419–40. administration of progesterone for patients with acute severe traumatic
57. Corps KN, Roth TL, McGavern DB. Inflammation and neuroprotec- brain injury: a randomized controlled trial. Crit Care 2008;12:R61.
tion in traumatic brain injury. JAMA Neurol 2015;72:355–62. 67. Skolnick BE, Maas AI, Narayan RK, van der Hoop RG, MacAllister
58. Eltzschig HK, Sitkovsky MV, Robson SC. Purinergic signaling dur- T, Ward JD, et al.; SYNAPSE Trial Investigators. A clinical trial of proges-
ing inflammation. N Engl J Med 2012;367:2322–33. terone for severe traumatic brain injury. N Engl J Med 2014;371:2467–76.
59. Nayak D, Roth TL, McGavern DB. Microglia development and func- 68. Wright DW, Yeatts SD, Silbergleit R, Palesch YY, Hertzberg VS, Fran-
tion. Annu Rev Immunol 2014;32:367–402. kel M, et al.; NETT Investigators. Very early administration of progester-
one for acute traumatic brain injury. N Engl J Med 2014;371:2457–66.
60. Hickman SE, Kingery ND, Ohsumi TK, Borowsky ML, Wang LC,
Means TK, et al. The microglial sensome revealed by direct RNA se- 69. Ma J, Huang S, Qin S, You C, Zeng Y. Progesterone for acute trau-
quencing. Nat Neurosci 2013;16:1896–905. matic brain injury. Cochrane Database Syst Rev 2016;12:CD008409.
61. Roth TL, Nayak D, Atanasijevic T, Koretsky AP, Latour LL, McGav- 70. Myburgh J, Cooper DJ, Finfer S, Bellomo R, Norton R, Bishop N,
ern DB. Transcranial amelioration of inflammation and cell death after et al.; SAFE Study Investigators; Australian and New Zealand Inten-
brain injury. Nature 2014;505:223–8. sive Care Society Clinical Trials Group; Australian Red Cross Blood
62. Szmydynger-Chodobska J, Strazielle N, Gandy JR, Keefe TH, Zink Service; George Institute for International Health. Saline or albumin for
BJ, Ghersi-Egea JF, et al. Posttraumatic invasion of monocytes across the fluid resuscitation in patients with traumatic brain injury. N Engl J Med
blood-cerebrospinal fluid barrier. J Cereb Blood Flow Metab 2012;32:93– 2007;357:874–84.
104. 71. Cooper DJ, Rosenfeld JV, Murray L, Arabi YM, Davies AR, D’Urso
63. Semple BD, Bye N, Rancan M, Ziebell JM, Morganti-Kossmann P, et al.; DECRA Trial Investigators; Australian and New Zealand Inten-
MC. Role of CCL2 (MCP-1) in traumatic brain injury (TBI): evidence sive Care Society Clinical Trials Group. Decompressive craniectomy in
from severe TBI patients and CCL2-/- mice. J Cereb Blood Flow Metab diffuse traumatic brain injury. N Engl J Med 2011;364:1493–502.
2010;30:769–82. 72. Australian Clinical Trials Alliance. Economic evaluation of investiga-
64. Nguyen HX, O’Barr TJ, Anderson AJ. Polymorphonuclear leuko- tor-initiated clinical trials conducted by networks Final report. ACSQHC.
cytes promote neurotoxicity through release of matrix metalloproteinases, 2017.
reactive oxygen species, and TNF-α. J Neurochem 2007;102:900–12. 73. Nichol A, Gantner D, Presneill J, Murray L, Trapani T, Bernard S,
65. Wright DW, Kellermann AL, Hertzberg VS, Clark PL, Frankel M, et al. Protocol for a multicentre randomised controlled trial of early and
Goldstein FC, et al. ProTECT: a randomized clinical trial of progesterone sustained prophylactic hypothermia in the management of traumatic brain
for acute traumatic brain injury. Ann Emerg Med 2007;49:391–402. injury. Crit Care Resusc 2015;17:92–100.
Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
Article first published online: May 22, 2018. - Manuscript accepted: May 8, 2018. - Manuscript received: May 3, 2018.
548 Journal of Neurosurgical Sciences October 2018
You might also like
- MDMA SoloDocument173 pagesMDMA SoloHighernataraj100% (1)
- Theory PosterDocument2 pagesTheory PosterSonja LueNo ratings yet
- Goldstein 5e PPT Ch3 CEADADocument33 pagesGoldstein 5e PPT Ch3 CEADAMary Lynn100% (1)
- Psych Nursing CareplanDocument9 pagesPsych Nursing Careplanwrite4js100% (1)
- 100+ Happiness ActivitiesDocument22 pages100+ Happiness ActivitiesEduardoLeitão100% (1)
- ICF DysarthriaDocument2 pagesICF DysarthriaCamila Guerrero AravenaNo ratings yet
- Introduction To Health Counselling Introduction To Health CounsellingDocument5 pagesIntroduction To Health Counselling Introduction To Health CounsellingCheung Kong Yiu90% (10)
- Case Study: Lyonel ChildsDocument11 pagesCase Study: Lyonel ChildsVaneSsaNo ratings yet
- UCMAS Presentation ENGLISH PDFDocument30 pagesUCMAS Presentation ENGLISH PDFSaid Ben BrahimNo ratings yet
- Quantum MindDocument72 pagesQuantum Mindrabiya100% (1)
- SLA Question Bank Chapters 1Document33 pagesSLA Question Bank Chapters 1Ashrath Muhammad100% (8)
- Anest e NMD Minerva 2013 - Racca PDFDocument15 pagesAnest e NMD Minerva 2013 - Racca PDFO Mei NeilNo ratings yet
- R37Y2022N02A0146Document9 pagesR37Y2022N02A0146rezaferidooni00No ratings yet
- Henarejos (2019)Document15 pagesHenarejos (2019)fadila anggrainiNo ratings yet
- The Cochrane Rehabilitation Ebook: A Knowledge Translation Tool To Transfer Evidence To Different Rehabilitation AudiencesDocument3 pagesThe Cochrane Rehabilitation Ebook: A Knowledge Translation Tool To Transfer Evidence To Different Rehabilitation AudiencesPedro CoelhoNo ratings yet
- Active Exergames To Improve Cognitive FunctioningDocument13 pagesActive Exergames To Improve Cognitive FunctioningEvelyn HerreraNo ratings yet
- 07 7136 Ejprm - NDocument10 pages07 7136 Ejprm - NDana DumitruNo ratings yet
- Diferencia Clinica Minima Detectable GaitDocument5 pagesDiferencia Clinica Minima Detectable GaitresidenciailianatulaNo ratings yet
- Tognolo L. 2022. Myofascial Points Treatment fESWT For Plantar Fasciitis. Open Label Randomized.Document9 pagesTognolo L. 2022. Myofascial Points Treatment fESWT For Plantar Fasciitis. Open Label Randomized.Javier MartinNo ratings yet
- Efficacy of A Proprioceptive Exercise Program in Patients With Nonspecific Neck PainDocument9 pagesEfficacy of A Proprioceptive Exercise Program in Patients With Nonspecific Neck Painbcvaughn019No ratings yet
- Jurnal 1Document8 pagesJurnal 1Dela Amelia Nur SalehaNo ratings yet
- R33Y2019N02A0156Document6 pagesR33Y2019N02A0156Wen-Yu ShinNo ratings yet
- TCD in ICUDocument14 pagesTCD in ICUJorge HernandezNo ratings yet
- Artigo EngimplanDocument6 pagesArtigo EngimplanKevinNo ratings yet
- Perioperative Cardiac Arrest in The Operating Room Environment A Review MinervAnest 2017Document9 pagesPerioperative Cardiac Arrest in The Operating Room Environment A Review MinervAnest 2017RicardoNo ratings yet
- Esclerosis Multiple Test Resistencias 2Document16 pagesEsclerosis Multiple Test Resistencias 2Israel BlancoNo ratings yet
- Effects On Power, Strength and Lean Body MassDocument10 pagesEffects On Power, Strength and Lean Body MassTiago MendesNo ratings yet
- Jurnal Covid 2Document10 pagesJurnal Covid 2Elliot AndersonNo ratings yet
- Efectos Del Ejercicio de Schroth Sobre La Escoliosis IdiopaticaDocument13 pagesEfectos Del Ejercicio de Schroth Sobre La Escoliosis Idiopaticaivanvillota7510No ratings yet
- Muscle Stretching Exercises and Resistance Training in Fibromyalgia: Which Is Better? A Three-Arm Randomized Controlled TrialDocument8 pagesMuscle Stretching Exercises and Resistance Training in Fibromyalgia: Which Is Better? A Three-Arm Randomized Controlled TrialDariusNo ratings yet
- Stem Cell-Derived Exosomes For Wound Healing: Current Status and Promising DirectionsDocument17 pagesStem Cell-Derived Exosomes For Wound Healing: Current Status and Promising DirectionsValerie hongNo ratings yet
- Bell PalsyDocument10 pagesBell PalsyMirza IKFR9No ratings yet
- Hemodynamic Management of Septic Shock: Expert OpinionDocument11 pagesHemodynamic Management of Septic Shock: Expert OpinionKamal NasirNo ratings yet
- Maitland em Osteoartrite FISIOFSIODocument10 pagesMaitland em Osteoartrite FISIOFSIOg.paffettiNo ratings yet
- Minerva Anestesiol 2017 GruenewaldDocument15 pagesMinerva Anestesiol 2017 GruenewaldMarjorie Lisseth Calderón LozanoNo ratings yet
- Anesthesiology Resident Induction Month: A Pilot Study Showing An Effective and Safe Way To Train Novice Residents Through SimulationDocument10 pagesAnesthesiology Resident Induction Month: A Pilot Study Showing An Effective and Safe Way To Train Novice Residents Through SimulationEmily Garcia EspinozaNo ratings yet
- Patogénesis EPOCDocument19 pagesPatogénesis EPOCAna CaballeroNo ratings yet
- Jurnal 1Document7 pagesJurnal 1dinnaNo ratings yet
- Gait PaperDocument12 pagesGait Papermb.farooqui02No ratings yet
- Rehabilitación Posoperatoria Del Hematoma Subdural Crónico en Ancianos. Un Estudio Observacional Centrado en El Equilibrio, La Deambulación y El Destino Del Alta.Document7 pagesRehabilitación Posoperatoria Del Hematoma Subdural Crónico en Ancianos. Un Estudio Observacional Centrado en El Equilibrio, La Deambulación y El Destino Del Alta.Leandro AntivilNo ratings yet
- Crisis Suprarrenal SecundariaDocument15 pagesCrisis Suprarrenal SecundariaLizbeth PalomecNo ratings yet
- Intermediate Care Unit - An Efficient and Flexible Facility, or A "Limbo" Between ICU and Ward?Document3 pagesIntermediate Care Unit - An Efficient and Flexible Facility, or A "Limbo" Between ICU and Ward?JHNo ratings yet
- Effect of Sensorimotor Stimulation On Oropharyngeal DysphagiaDocument11 pagesEffect of Sensorimotor Stimulation On Oropharyngeal Dysphagiasneha duttaNo ratings yet
- Condyloma Acuminata (JURNAL)Document8 pagesCondyloma Acuminata (JURNAL)Renaldi RNo ratings yet
- Crio Na Artite ReumatoideDocument13 pagesCrio Na Artite ReumatoideThiago Penna ChavesNo ratings yet
- R33Y2019N04A0472Document8 pagesR33Y2019N04A0472Noura RoseNo ratings yet
- Antidoping Program: An Important Factor in The Promotion and Protection of The Integrity of Sport and Athlete's HealthDocument26 pagesAntidoping Program: An Important Factor in The Promotion and Protection of The Integrity of Sport and Athlete's HealthAlex BeltranNo ratings yet
- Niños Revista ItalanaDocument10 pagesNiños Revista ItalanaJesusErnestoAguirreLopezNo ratings yet
- R23Y2018N03A0403Document16 pagesR23Y2018N03A0403Andrés WunderwaldNo ratings yet
- G4-2017-Barbieri-Body Composition and Size in Sprint AthletesDocument5 pagesG4-2017-Barbieri-Body Composition and Size in Sprint AthletesJoaquin EstrellaNo ratings yet
- R34Y2021N04A0345Document13 pagesR34Y2021N04A0345r.barca98No ratings yet
- Anxitatea Periop - Review - 2018Document11 pagesAnxitatea Periop - Review - 2018Fiorel Loves EveryoneNo ratings yet
- 2016 BOTOX TERAPIA ESPEJO - European Journal of Physical and Rehabilitation MedicineDocument9 pages2016 BOTOX TERAPIA ESPEJO - European Journal of Physical and Rehabilitation MedicineSergio Navarrete VidalNo ratings yet
- Effect 5-Weeks Pre-Season Training With Small-Sided Game in RSA According To Physical FitnessDocument9 pagesEffect 5-Weeks Pre-Season Training With Small-Sided Game in RSA According To Physical Fitnessimededdine boutabbaNo ratings yet
- Fink 2018Document9 pagesFink 2018ChrisNo ratings yet
- 10-Week Core Stability TrainingDocument10 pages10-Week Core Stability TrainingWen-Yu ShinNo ratings yet
- Patient Blood Management. A Fresh Look at A Fresh Approach To Blood Transfusion PDFDocument11 pagesPatient Blood Management. A Fresh Look at A Fresh Approach To Blood Transfusion PDFMarcela Garzon O VelezNo ratings yet
- R07Y2022N03A0261Document3 pagesR07Y2022N03A0261Surya DharmaNo ratings yet
- ShimadzuJournal Vol.02 2Document20 pagesShimadzuJournal Vol.02 2Salvador GomezNo ratings yet
- Vitamin D and The Skin What Should A Dermatologist KnowDocument12 pagesVitamin D and The Skin What Should A Dermatologist Knowvanessa_werbickyNo ratings yet
- Psychological Reactions To Covid-19 and Epidemiological Aspects of Dental Practitioners During Lockdown in ItalyDocument12 pagesPsychological Reactions To Covid-19 and Epidemiological Aspects of Dental Practitioners During Lockdown in ItalyAlexandre ChisiniNo ratings yet
- Dental Occlusion and Sport Performance: ReviewDocument7 pagesDental Occlusion and Sport Performance: Reviewsolodont1No ratings yet
- Balance Versus Resistance Training On Postural Control in Patients With Parkinsons DiseaseDocument11 pagesBalance Versus Resistance Training On Postural Control in Patients With Parkinsons DiseaseSuislian MarjorieNo ratings yet
- Liver Trauma 2020Document12 pagesLiver Trauma 2020Florin BoteaNo ratings yet
- The Endocannabinoid System and Its Relevance For NDocument24 pagesThe Endocannabinoid System and Its Relevance For NtamaraNo ratings yet
- 10 23736@S1973-9087 17 04749-9Document8 pages10 23736@S1973-9087 17 04749-9Kings AndrewNo ratings yet
- Neuropsychological Rehabilitation: An International JournalDocument20 pagesNeuropsychological Rehabilitation: An International JournalRodrigoNo ratings yet
- Ozcwuck OndansetronDocument10 pagesOzcwuck OndansetronAldaherlen BangunNo ratings yet
- Sedation in Neurocritical Patients: Is It Useful?: ReviewDocument7 pagesSedation in Neurocritical Patients: Is It Useful?: ReviewAditiaPLNo ratings yet
- Nanomedicine: Application of Nanotechnology: ArticleDocument9 pagesNanomedicine: Application of Nanotechnology: ArticleAndres GomezNo ratings yet
- Billabong School Bhopal Holiday Homework For Grade 2Document5 pagesBillabong School Bhopal Holiday Homework For Grade 2ers57e8sNo ratings yet
- Neuro Anatomy Neuro AssessmentDocument96 pagesNeuro Anatomy Neuro AssessmentJulia Rae Delos SantosNo ratings yet
- 109 Questions On Psychotic DisordersDocument21 pages109 Questions On Psychotic Disordersmaryannrichelle100% (21)
- 2 - English8-Q3-Week4Document20 pages2 - English8-Q3-Week4Wyn DingalNo ratings yet
- Chapter - 7: Control and CoordinationDocument30 pagesChapter - 7: Control and Coordinationuma mishraNo ratings yet
- Core Beliefs Worksheet PDFDocument3 pagesCore Beliefs Worksheet PDFMarieSmithNo ratings yet
- Chapter 1 Introduction To Machine LearningDocument19 pagesChapter 1 Introduction To Machine LearningShreeji Modh100% (1)
- Insomnia .Sleep With HomoeopathyDocument3 pagesInsomnia .Sleep With HomoeopathyEditor IJTSRDNo ratings yet
- Affect Detection An Interdisciplinary Review of Models Methods and Their Applications PDFDocument20 pagesAffect Detection An Interdisciplinary Review of Models Methods and Their Applications PDFSumitha ArunNo ratings yet
- Unit Planning Flowchart WORDDocument1 pageUnit Planning Flowchart WORDMichelle PeutNo ratings yet
- LCS - SwearingDocument2 pagesLCS - SwearingMB FernandezNo ratings yet
- ILA-Form1-2-Sample-Lesson 1 Fact & OpinionDocument2 pagesILA-Form1-2-Sample-Lesson 1 Fact & OpinionRheymund CañeteNo ratings yet
- Journal of Family Therapy (1979) 1: 253-269Document17 pagesJournal of Family Therapy (1979) 1: 253-269Rita1976No ratings yet
- Attention-Deficit Hyperactivity DisorderDocument9 pagesAttention-Deficit Hyperactivity Disorderapi-608455943No ratings yet
- Eng211CO2021 22 DALUMAYDocument5 pagesEng211CO2021 22 DALUMAYCiarrah PosterNo ratings yet
- Why We Sleep PDFDocument9 pagesWhy We Sleep PDFEmine ToptaşNo ratings yet
- Lima-Cabello Et Al-2014-Journal of Pineal ResearchDocument9 pagesLima-Cabello Et Al-2014-Journal of Pineal ResearchElena Martínez CelisNo ratings yet
- Maladaptive Patterns of Behavior Psyche ConceptDocument273 pagesMaladaptive Patterns of Behavior Psyche Conceptsylphisochi83% (6)
- The Cognitive Process Dimension A Taxonomy For Learning Teaching and Assessing A Revision of Bloom's Taxonomy of Educational Objectives Lorin W. Anderson and David R. KrathwohlDocument1 pageThe Cognitive Process Dimension A Taxonomy For Learning Teaching and Assessing A Revision of Bloom's Taxonomy of Educational Objectives Lorin W. Anderson and David R. KrathwohlihsanNo ratings yet