
Ann Soehee - Tctap2021 - SPC
Ann Soehee - Tctap2021 - SPC
You might also like
- TM 11398Document592 pagesTM 11398krill.copco50% (2)
- UPSC New Syllabus & Tips To Crack IAS Preliminary & Mains Exam PDFDocument59 pagesUPSC New Syllabus & Tips To Crack IAS Preliminary & Mains Exam PDFPrateek SahniNo ratings yet
- Dyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDDocument15 pagesDyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيارNo ratings yet
- NCEP Hyperlipidemia GoalsDocument6 pagesNCEP Hyperlipidemia GoalsVictoria Eliza InguilloNo ratings yet
- Dipiro Edisi 9 KolestrolDocument10 pagesDipiro Edisi 9 KolestrolFriska tampuboLonNo ratings yet
- Triglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Document20 pagesTriglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Indah Pujiati DtNo ratings yet
- ATP III Guidelines at-A-Glance Quick Desk ReferenceDocument6 pagesATP III Guidelines at-A-Glance Quick Desk ReferenceAnna DangNo ratings yet
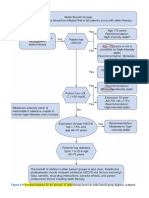
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNo ratings yet
- Management of Blood Cholesterol 2019Document2 pagesManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassNo ratings yet
- New Developments in The Management of Dyslipidemia: Widjanarko. W MDDocument62 pagesNew Developments in The Management of Dyslipidemia: Widjanarko. W MDyulanda fitrianaNo ratings yet
- 2019 - ESC - Guidelines SLIDESDocument23 pages2019 - ESC - Guidelines SLIDESFa CurieNo ratings yet
- New Developments in The Management of DyslipidemiaDocument63 pagesNew Developments in The Management of DyslipidemiaM Azmi HNo ratings yet
- Management of Dyslipidemia and The Prevention of Cardiovascular DiseaseDocument2 pagesManagement of Dyslipidemia and The Prevention of Cardiovascular DiseaseBenny TrisaktyariNo ratings yet
- Dislipidemia: Ulvi Nur RistaDocument29 pagesDislipidemia: Ulvi Nur RistaYogie 1290No ratings yet
- MG/DL MG/DL MG/DL MG/DL MG/DL MG/DLDocument3 pagesMG/DL MG/DL MG/DL MG/DL MG/DL MG/DLAli Shaikh AbdulNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- Role of Rosuvastatin in The Treatment of DyslipidemiaDocument16 pagesRole of Rosuvastatin in The Treatment of DyslipidemiaabcdefNo ratings yet
- 10-Year Risk of Fatal CVD Is Based On Risk Factors: Age, Smoking, Sex, Systolic Blood Pressure and Total CholesterolDocument3 pages10-Year Risk of Fatal CVD Is Based On Risk Factors: Age, Smoking, Sex, Systolic Blood Pressure and Total CholesterolDidik SiswandoroNo ratings yet
- ReferatDocument53 pagesReferatLia pramitaNo ratings yet
- 4.investigations of Serum LipidsDocument7 pages4.investigations of Serum LipidsMV ProductionNo ratings yet
- Dyslipidaemia 2019Document61 pagesDyslipidaemia 2019fatima.shqeratNo ratings yet
- Raza2004 PDFDocument12 pagesRaza2004 PDFIvana RuseskaNo ratings yet
- Dyslipidemia ATP4 GUIDLINESDocument9 pagesDyslipidemia ATP4 GUIDLINESSandy GunawanNo ratings yet
- 2018 Cholesterol Guidelines Made Simple ToolDocument22 pages2018 Cholesterol Guidelines Made Simple ToolLeoberto Batista Pereira SobrinhoNo ratings yet
- Guidelines Made Simple Tool 2018 CholesterolDocument22 pagesGuidelines Made Simple Tool 2018 CholesterolHussain HameedNo ratings yet
- Cardiometabolic RiskDocument1 pageCardiometabolic RiskVaidya Priyanka SharmaNo ratings yet
- Atp 3 Update by Grundy Et AlDocument16 pagesAtp 3 Update by Grundy Et AlcristiandertorossianNo ratings yet
- What's New in Lipid GuidelinesDocument31 pagesWhat's New in Lipid GuidelinesYunita WidyaningsihNo ratings yet
- Dyslipidemia: Signs and SymptomsDocument24 pagesDyslipidemia: Signs and Symptomschrissanto chandraNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- DyslipidemiaDocument53 pagesDyslipidemiaRey AlwiwikhNo ratings yet
- Aztor Cme NewDocument59 pagesAztor Cme NewSheikh Sharfuddin RajeevNo ratings yet
- Understanding The Needs of The High Productive DyslipidemiaDocument47 pagesUnderstanding The Needs of The High Productive DyslipidemiachchchchkNo ratings yet
- Jurnal HiperlipidDocument7 pagesJurnal HiperlipidAyu SaputriNo ratings yet
- Alfa ResultSubServices 4Document1 pageAlfa ResultSubServices 4ayaabouaufNo ratings yet
- Lipids JBDocument48 pagesLipids JBMuvenn KannanNo ratings yet
- Guidelines Made Simple Tool 2018 CholesterolDocument22 pagesGuidelines Made Simple Tool 2018 CholesterolSafira HalimatussadiahNo ratings yet
- Pediatric Patients (10-17 Years of Age)Document18 pagesPediatric Patients (10-17 Years of Age)asdwasdNo ratings yet
- 2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsDocument37 pages2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsIman SaksoukNo ratings yet
- Dyslipidemia 2008Document80 pagesDyslipidemia 2008Pucca' JernyNo ratings yet
- Cholesterol Guidelines Review 2020Document6 pagesCholesterol Guidelines Review 2020oriannaocantoNo ratings yet
- Leo Atp IvDocument25 pagesLeo Atp IvLeonardo MedinaNo ratings yet
- New Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesDocument6 pagesNew Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesJustinaNo ratings yet
- National Cholesterol Education ProgramDocument52 pagesNational Cholesterol Education Programi_top3No ratings yet
- 2017 DCP 1. Telmisartan Untuk KasusDocument26 pages2017 DCP 1. Telmisartan Untuk KasusOcto IndradjajaNo ratings yet
- I Am A Gentle: KillerDocument50 pagesI Am A Gentle: KillerMaltadillaNo ratings yet
- Lipid Profile: Test Name Result Units Biological Reference IntervalDocument2 pagesLipid Profile: Test Name Result Units Biological Reference IntervalArpanpatelNo ratings yet
- Intensity of Cholesterol Lowering With Statin in PatientsDocument23 pagesIntensity of Cholesterol Lowering With Statin in Patientsandri ansyahNo ratings yet
- Dyslipidaemias 2019Document30 pagesDyslipidaemias 2019Adinda DianNo ratings yet
- A Comprehensive Review On Metabolic SyndromeDocument41 pagesA Comprehensive Review On Metabolic Syndromeveerraju tvNo ratings yet
- Optimal Low-Density Lipoprotein Is 50 To 70 MG - DL - Lower Is Better and Physiologically Normal - ScienceDirectDocument13 pagesOptimal Low-Density Lipoprotein Is 50 To 70 MG - DL - Lower Is Better and Physiologically Normal - ScienceDirectJNo ratings yet
- Nicotinic Acid 10-20% 10-20% 14-35% 30-70% Reasonable To PoorDocument5 pagesNicotinic Acid 10-20% 10-20% 14-35% 30-70% Reasonable To PoorvmvlivNo ratings yet
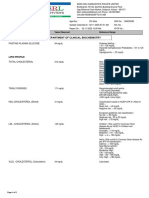
- Department of Clinical Biochemistry: Fasting Plasma GlucoseDocument2 pagesDepartment of Clinical Biochemistry: Fasting Plasma Glucosearavind sNo ratings yet
- BBM Lipoprotein Metabolism Related DisordersDocument26 pagesBBM Lipoprotein Metabolism Related Disorderskaterina KarinaNo ratings yet
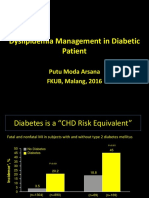
- Dyslipidemia Management in Diabetic Patient: Putu Moda Arsana FKUB, Malang, 2016Document31 pagesDyslipidemia Management in Diabetic Patient: Putu Moda Arsana FKUB, Malang, 2016aprinaaaNo ratings yet
- Slides The Evolving Need and Challenges To Reach LDL C Targets in High Risk PatientsDocument14 pagesSlides The Evolving Need and Challenges To Reach LDL C Targets in High Risk PatientsBasem HeshamNo ratings yet
- HYPERLIPIDEMIADocument33 pagesHYPERLIPIDEMIAatiqullah tarmiziNo ratings yet
- Dislipid 2 PDFDocument4 pagesDislipid 2 PDFWahyuningsih HamidNo ratings yet
- Lipid Profile TestDocument2 pagesLipid Profile TestPrateek KanadeNo ratings yet
- HypertensionDocument8 pagesHypertensionchandra9000No ratings yet
- Positioning Lecture 7Document31 pagesPositioning Lecture 7Saad KhanNo ratings yet
- Segmentation - Targeting Lecture 6Document34 pagesSegmentation - Targeting Lecture 6Saad KhanNo ratings yet
- Product Management Lecture 1Document44 pagesProduct Management Lecture 1Saad KhanNo ratings yet
- Promo Code Lecture 4Document22 pagesPromo Code Lecture 4Saad KhanNo ratings yet
- NACHC Statin Guideline Snapshot GenericDocument14 pagesNACHC Statin Guideline Snapshot GenericSaad KhanNo ratings yet
- Pm0320 DavisHarry Ezetimi SundayDocument27 pagesPm0320 DavisHarry Ezetimi SundaySaad KhanNo ratings yet
- 4 ACC Prevention CholesterolDocument88 pages4 ACC Prevention CholesterolSaad KhanNo ratings yet
- Key Lessons On LDL C and CV RiskDocument17 pagesKey Lessons On LDL C and CV RiskSaad KhanNo ratings yet
- Jupiter TrialDocument40 pagesJupiter TrialSaad KhanNo ratings yet
- Hypolipidemic Drugs and Plasma Expanders: Dr. Rishi PalDocument49 pagesHypolipidemic Drugs and Plasma Expanders: Dr. Rishi PalSaad KhanNo ratings yet
- 4.phases in Agricultural DevelopmentDocument16 pages4.phases in Agricultural Developmentakuril100% (3)
- Federal MogulDocument277 pagesFederal Mogulعبدالغني القباطي100% (1)
- En Mongolia 06Document39 pagesEn Mongolia 06Sandeep DasNo ratings yet
- Battles Fought On The Great Wall of China Qin DynastyDocument2 pagesBattles Fought On The Great Wall of China Qin DynastySachin NagmotiNo ratings yet
- Gas Pressure Reducing: Gas Pressure Reducing & Shut-Off Valve & Shut-Off Valve Series 71P11A Series 71P11ADocument4 pagesGas Pressure Reducing: Gas Pressure Reducing & Shut-Off Valve & Shut-Off Valve Series 71P11A Series 71P11AĐình Sơn HoàngNo ratings yet
- X PPT CH 12 ElectricityDocument12 pagesX PPT CH 12 ElectricityAakriti100% (1)
- TapingDocument3 pagesTapingEdeza MatarumNo ratings yet
- Exercise # 1: Statistics and ProbabilityDocument6 pagesExercise # 1: Statistics and ProbabilityAszyla ArzaNo ratings yet
- IllithidDocument5 pagesIllithidMattia La RosaNo ratings yet
- Earth Quake DesignDocument13 pagesEarth Quake DesignRanie boy CabanillaNo ratings yet
- Hybrid Vehicle A Study On Technology IJERTV3IS120917 PDFDocument8 pagesHybrid Vehicle A Study On Technology IJERTV3IS120917 PDFAshish MathurNo ratings yet
- Textbook Pediatric Behavioral Nutrition Factors Environment Education and Self Regulation 1St Edition Areej Hassan Ebook All Chapter PDFDocument39 pagesTextbook Pediatric Behavioral Nutrition Factors Environment Education and Self Regulation 1St Edition Areej Hassan Ebook All Chapter PDFjanet.galloway812100% (8)
- Case 621F, 721F Tier 4 Wheel Loader AxelDocument15 pagesCase 621F, 721F Tier 4 Wheel Loader AxelJose CarmonaNo ratings yet
- Tac85 11Document32 pagesTac85 11TateNo ratings yet
- SCM and TQM: by Junaid ShaheedDocument8 pagesSCM and TQM: by Junaid ShaheedjunaidsNo ratings yet
- LAB 2 - Running Speed (Method 2) OEL 1Document3 pagesLAB 2 - Running Speed (Method 2) OEL 1ZULFAQAR BIN MOHAMMAD NIZAMNo ratings yet
- Open-Circuit Time Constant Analysis: Asas As Hs K Bsbs BsDocument24 pagesOpen-Circuit Time Constant Analysis: Asas As Hs K Bsbs BsSHAIK MUSTHAFANo ratings yet
- Green Building Toward Construction Sustainability: Energy Efficiency With Material and Design AspectsDocument11 pagesGreen Building Toward Construction Sustainability: Energy Efficiency With Material and Design AspectsghchgNo ratings yet
- Carbon Capture Corrosion Current Practice 2023Document12 pagesCarbon Capture Corrosion Current Practice 2023Wayne MonneryNo ratings yet
- Cibse Solar AcDocument11 pagesCibse Solar Acdhananjay176No ratings yet
- MGje 6 Fix GX PK Yp RBJ LBRDocument9 pagesMGje 6 Fix GX PK Yp RBJ LBRBANOTH KUMARNo ratings yet
- Ignatian SpiritualityDocument16 pagesIgnatian SpiritualityMihai Frentz100% (2)
- Price List 2018Document20 pagesPrice List 2018Imml TasbiNo ratings yet
- UntitledDocument14 pagesUntitlednaresh kumarNo ratings yet
- 4 Poisonous & Venomous AnimalsDocument47 pages4 Poisonous & Venomous AnimalsAnyi Yulieth AMPUDIA MURILLONo ratings yet
- Wind EnergyDocument6 pagesWind EnergyRajat DubeyNo ratings yet
- Quatre Agro Enterprise Private LimitedDocument25 pagesQuatre Agro Enterprise Private Limitedp23pallavNo ratings yet
- LECLANCHE Cell Datasheet GL60 GNMC 60ahDocument2 pagesLECLANCHE Cell Datasheet GL60 GNMC 60ahChaitanyaNo ratings yet





























































































Download as pdf or txt
You might also like
- TM 11398Document592 pagesTM 11398krill.copco50% (2)
- UPSC New Syllabus & Tips To Crack IAS Preliminary & Mains Exam PDFDocument59 pagesUPSC New Syllabus & Tips To Crack IAS Preliminary & Mains Exam PDFPrateek SahniNo ratings yet
- Dyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDDocument15 pagesDyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيارNo ratings yet
- NCEP Hyperlipidemia GoalsDocument6 pagesNCEP Hyperlipidemia GoalsVictoria Eliza InguilloNo ratings yet
- Dipiro Edisi 9 KolestrolDocument10 pagesDipiro Edisi 9 KolestrolFriska tampuboLonNo ratings yet
- Triglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Document20 pagesTriglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Indah Pujiati DtNo ratings yet
- ATP III Guidelines at-A-Glance Quick Desk ReferenceDocument6 pagesATP III Guidelines at-A-Glance Quick Desk ReferenceAnna DangNo ratings yet
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNo ratings yet
- Management of Blood Cholesterol 2019Document2 pagesManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassNo ratings yet
- New Developments in The Management of Dyslipidemia: Widjanarko. W MDDocument62 pagesNew Developments in The Management of Dyslipidemia: Widjanarko. W MDyulanda fitrianaNo ratings yet
- 2019 - ESC - Guidelines SLIDESDocument23 pages2019 - ESC - Guidelines SLIDESFa CurieNo ratings yet
- New Developments in The Management of DyslipidemiaDocument63 pagesNew Developments in The Management of DyslipidemiaM Azmi HNo ratings yet
- Management of Dyslipidemia and The Prevention of Cardiovascular DiseaseDocument2 pagesManagement of Dyslipidemia and The Prevention of Cardiovascular DiseaseBenny TrisaktyariNo ratings yet
- Dislipidemia: Ulvi Nur RistaDocument29 pagesDislipidemia: Ulvi Nur RistaYogie 1290No ratings yet
- MG/DL MG/DL MG/DL MG/DL MG/DL MG/DLDocument3 pagesMG/DL MG/DL MG/DL MG/DL MG/DL MG/DLAli Shaikh AbdulNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- Role of Rosuvastatin in The Treatment of DyslipidemiaDocument16 pagesRole of Rosuvastatin in The Treatment of DyslipidemiaabcdefNo ratings yet
- 10-Year Risk of Fatal CVD Is Based On Risk Factors: Age, Smoking, Sex, Systolic Blood Pressure and Total CholesterolDocument3 pages10-Year Risk of Fatal CVD Is Based On Risk Factors: Age, Smoking, Sex, Systolic Blood Pressure and Total CholesterolDidik SiswandoroNo ratings yet
- ReferatDocument53 pagesReferatLia pramitaNo ratings yet
- 4.investigations of Serum LipidsDocument7 pages4.investigations of Serum LipidsMV ProductionNo ratings yet
- Dyslipidaemia 2019Document61 pagesDyslipidaemia 2019fatima.shqeratNo ratings yet
- Raza2004 PDFDocument12 pagesRaza2004 PDFIvana RuseskaNo ratings yet
- Dyslipidemia ATP4 GUIDLINESDocument9 pagesDyslipidemia ATP4 GUIDLINESSandy GunawanNo ratings yet
- 2018 Cholesterol Guidelines Made Simple ToolDocument22 pages2018 Cholesterol Guidelines Made Simple ToolLeoberto Batista Pereira SobrinhoNo ratings yet
- Guidelines Made Simple Tool 2018 CholesterolDocument22 pagesGuidelines Made Simple Tool 2018 CholesterolHussain HameedNo ratings yet
- Cardiometabolic RiskDocument1 pageCardiometabolic RiskVaidya Priyanka SharmaNo ratings yet
- Atp 3 Update by Grundy Et AlDocument16 pagesAtp 3 Update by Grundy Et AlcristiandertorossianNo ratings yet
- What's New in Lipid GuidelinesDocument31 pagesWhat's New in Lipid GuidelinesYunita WidyaningsihNo ratings yet
- Dyslipidemia: Signs and SymptomsDocument24 pagesDyslipidemia: Signs and Symptomschrissanto chandraNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- DyslipidemiaDocument53 pagesDyslipidemiaRey AlwiwikhNo ratings yet
- Aztor Cme NewDocument59 pagesAztor Cme NewSheikh Sharfuddin RajeevNo ratings yet
- Understanding The Needs of The High Productive DyslipidemiaDocument47 pagesUnderstanding The Needs of The High Productive DyslipidemiachchchchkNo ratings yet
- Jurnal HiperlipidDocument7 pagesJurnal HiperlipidAyu SaputriNo ratings yet
- Alfa ResultSubServices 4Document1 pageAlfa ResultSubServices 4ayaabouaufNo ratings yet
- Lipids JBDocument48 pagesLipids JBMuvenn KannanNo ratings yet
- Guidelines Made Simple Tool 2018 CholesterolDocument22 pagesGuidelines Made Simple Tool 2018 CholesterolSafira HalimatussadiahNo ratings yet
- Pediatric Patients (10-17 Years of Age)Document18 pagesPediatric Patients (10-17 Years of Age)asdwasdNo ratings yet
- 2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsDocument37 pages2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsIman SaksoukNo ratings yet
- Dyslipidemia 2008Document80 pagesDyslipidemia 2008Pucca' JernyNo ratings yet
- Cholesterol Guidelines Review 2020Document6 pagesCholesterol Guidelines Review 2020oriannaocantoNo ratings yet
- Leo Atp IvDocument25 pagesLeo Atp IvLeonardo MedinaNo ratings yet
- New Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesDocument6 pagesNew Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesJustinaNo ratings yet
- National Cholesterol Education ProgramDocument52 pagesNational Cholesterol Education Programi_top3No ratings yet
- 2017 DCP 1. Telmisartan Untuk KasusDocument26 pages2017 DCP 1. Telmisartan Untuk KasusOcto IndradjajaNo ratings yet
- I Am A Gentle: KillerDocument50 pagesI Am A Gentle: KillerMaltadillaNo ratings yet
- Lipid Profile: Test Name Result Units Biological Reference IntervalDocument2 pagesLipid Profile: Test Name Result Units Biological Reference IntervalArpanpatelNo ratings yet
- Intensity of Cholesterol Lowering With Statin in PatientsDocument23 pagesIntensity of Cholesterol Lowering With Statin in Patientsandri ansyahNo ratings yet
- Dyslipidaemias 2019Document30 pagesDyslipidaemias 2019Adinda DianNo ratings yet
- A Comprehensive Review On Metabolic SyndromeDocument41 pagesA Comprehensive Review On Metabolic Syndromeveerraju tvNo ratings yet
- Optimal Low-Density Lipoprotein Is 50 To 70 MG - DL - Lower Is Better and Physiologically Normal - ScienceDirectDocument13 pagesOptimal Low-Density Lipoprotein Is 50 To 70 MG - DL - Lower Is Better and Physiologically Normal - ScienceDirectJNo ratings yet
- Nicotinic Acid 10-20% 10-20% 14-35% 30-70% Reasonable To PoorDocument5 pagesNicotinic Acid 10-20% 10-20% 14-35% 30-70% Reasonable To PoorvmvlivNo ratings yet
- Department of Clinical Biochemistry: Fasting Plasma GlucoseDocument2 pagesDepartment of Clinical Biochemistry: Fasting Plasma Glucosearavind sNo ratings yet
- BBM Lipoprotein Metabolism Related DisordersDocument26 pagesBBM Lipoprotein Metabolism Related Disorderskaterina KarinaNo ratings yet
- Dyslipidemia Management in Diabetic Patient: Putu Moda Arsana FKUB, Malang, 2016Document31 pagesDyslipidemia Management in Diabetic Patient: Putu Moda Arsana FKUB, Malang, 2016aprinaaaNo ratings yet
- Slides The Evolving Need and Challenges To Reach LDL C Targets in High Risk PatientsDocument14 pagesSlides The Evolving Need and Challenges To Reach LDL C Targets in High Risk PatientsBasem HeshamNo ratings yet
- HYPERLIPIDEMIADocument33 pagesHYPERLIPIDEMIAatiqullah tarmiziNo ratings yet
- Dislipid 2 PDFDocument4 pagesDislipid 2 PDFWahyuningsih HamidNo ratings yet
- Lipid Profile TestDocument2 pagesLipid Profile TestPrateek KanadeNo ratings yet
- HypertensionDocument8 pagesHypertensionchandra9000No ratings yet
- Positioning Lecture 7Document31 pagesPositioning Lecture 7Saad KhanNo ratings yet
- Segmentation - Targeting Lecture 6Document34 pagesSegmentation - Targeting Lecture 6Saad KhanNo ratings yet
- Product Management Lecture 1Document44 pagesProduct Management Lecture 1Saad KhanNo ratings yet
- Promo Code Lecture 4Document22 pagesPromo Code Lecture 4Saad KhanNo ratings yet
- NACHC Statin Guideline Snapshot GenericDocument14 pagesNACHC Statin Guideline Snapshot GenericSaad KhanNo ratings yet
- Pm0320 DavisHarry Ezetimi SundayDocument27 pagesPm0320 DavisHarry Ezetimi SundaySaad KhanNo ratings yet
- 4 ACC Prevention CholesterolDocument88 pages4 ACC Prevention CholesterolSaad KhanNo ratings yet
- Key Lessons On LDL C and CV RiskDocument17 pagesKey Lessons On LDL C and CV RiskSaad KhanNo ratings yet
- Jupiter TrialDocument40 pagesJupiter TrialSaad KhanNo ratings yet
- Hypolipidemic Drugs and Plasma Expanders: Dr. Rishi PalDocument49 pagesHypolipidemic Drugs and Plasma Expanders: Dr. Rishi PalSaad KhanNo ratings yet
- 4.phases in Agricultural DevelopmentDocument16 pages4.phases in Agricultural Developmentakuril100% (3)
- Federal MogulDocument277 pagesFederal Mogulعبدالغني القباطي100% (1)
- En Mongolia 06Document39 pagesEn Mongolia 06Sandeep DasNo ratings yet
- Battles Fought On The Great Wall of China Qin DynastyDocument2 pagesBattles Fought On The Great Wall of China Qin DynastySachin NagmotiNo ratings yet
- Gas Pressure Reducing: Gas Pressure Reducing & Shut-Off Valve & Shut-Off Valve Series 71P11A Series 71P11ADocument4 pagesGas Pressure Reducing: Gas Pressure Reducing & Shut-Off Valve & Shut-Off Valve Series 71P11A Series 71P11AĐình Sơn HoàngNo ratings yet
- X PPT CH 12 ElectricityDocument12 pagesX PPT CH 12 ElectricityAakriti100% (1)
- TapingDocument3 pagesTapingEdeza MatarumNo ratings yet
- Exercise # 1: Statistics and ProbabilityDocument6 pagesExercise # 1: Statistics and ProbabilityAszyla ArzaNo ratings yet
- IllithidDocument5 pagesIllithidMattia La RosaNo ratings yet
- Earth Quake DesignDocument13 pagesEarth Quake DesignRanie boy CabanillaNo ratings yet
- Hybrid Vehicle A Study On Technology IJERTV3IS120917 PDFDocument8 pagesHybrid Vehicle A Study On Technology IJERTV3IS120917 PDFAshish MathurNo ratings yet
- Textbook Pediatric Behavioral Nutrition Factors Environment Education and Self Regulation 1St Edition Areej Hassan Ebook All Chapter PDFDocument39 pagesTextbook Pediatric Behavioral Nutrition Factors Environment Education and Self Regulation 1St Edition Areej Hassan Ebook All Chapter PDFjanet.galloway812100% (8)
- Case 621F, 721F Tier 4 Wheel Loader AxelDocument15 pagesCase 621F, 721F Tier 4 Wheel Loader AxelJose CarmonaNo ratings yet
- Tac85 11Document32 pagesTac85 11TateNo ratings yet
- SCM and TQM: by Junaid ShaheedDocument8 pagesSCM and TQM: by Junaid ShaheedjunaidsNo ratings yet
- LAB 2 - Running Speed (Method 2) OEL 1Document3 pagesLAB 2 - Running Speed (Method 2) OEL 1ZULFAQAR BIN MOHAMMAD NIZAMNo ratings yet
- Open-Circuit Time Constant Analysis: Asas As Hs K Bsbs BsDocument24 pagesOpen-Circuit Time Constant Analysis: Asas As Hs K Bsbs BsSHAIK MUSTHAFANo ratings yet
- Green Building Toward Construction Sustainability: Energy Efficiency With Material and Design AspectsDocument11 pagesGreen Building Toward Construction Sustainability: Energy Efficiency With Material and Design AspectsghchgNo ratings yet
- Carbon Capture Corrosion Current Practice 2023Document12 pagesCarbon Capture Corrosion Current Practice 2023Wayne MonneryNo ratings yet
- Cibse Solar AcDocument11 pagesCibse Solar Acdhananjay176No ratings yet
- MGje 6 Fix GX PK Yp RBJ LBRDocument9 pagesMGje 6 Fix GX PK Yp RBJ LBRBANOTH KUMARNo ratings yet
- Ignatian SpiritualityDocument16 pagesIgnatian SpiritualityMihai Frentz100% (2)
- Price List 2018Document20 pagesPrice List 2018Imml TasbiNo ratings yet
- UntitledDocument14 pagesUntitlednaresh kumarNo ratings yet
- 4 Poisonous & Venomous AnimalsDocument47 pages4 Poisonous & Venomous AnimalsAnyi Yulieth AMPUDIA MURILLONo ratings yet
- Wind EnergyDocument6 pagesWind EnergyRajat DubeyNo ratings yet
- Quatre Agro Enterprise Private LimitedDocument25 pagesQuatre Agro Enterprise Private Limitedp23pallavNo ratings yet
- LECLANCHE Cell Datasheet GL60 GNMC 60ahDocument2 pagesLECLANCHE Cell Datasheet GL60 GNMC 60ahChaitanyaNo ratings yet